Chronic kidney disease for nurses
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching PubMed
"chronic kidney disease" AND nursing
Searching Images
chronic kidney disease stages GFR diagram
Loading Image
Loading Image
Finding Sources
I now have comprehensive information from the medical library to deliver a thorough, nursing-oriented overview of CKD. Let me compile this into a well-structured response.
Chronic Kidney Disease (CKD) — Nursing Overview
Definition
CKD is defined as kidney damage or decreased kidney function persisting for ≥ 3 months, regardless of cause. It is a major public health burden, affecting approximately 1 in 7 adults in the United States. — Textbook of Family Medicine 9e
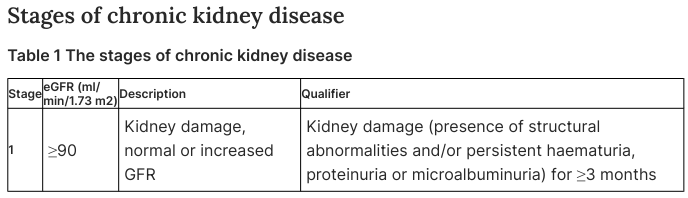
Staging (KDIGO Classification)
CKD is staged by estimated GFR (eGFR) and albuminuria category:
| Stage | eGFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥ 90 | Kidney damage with normal/increased GFR |
| G2 | 60–89 | Mildly decreased GFR |
| G3 | 30–59 | Moderately decreased GFR |
| G4 | 15–29 | Severely decreased GFR |
| G5 | < 15 | Kidney failure (ESKD) |
Kidney damage is defined by structural abnormalities and/or persistent haematuria, proteinuria, or microalbuminuria for ≥ 3 months.
GFR Estimation Formulas
Nurses need to understand how GFR is calculated to interpret lab results and dose medications:
- Cockcroft-Gault:
CrCl (mL/min) = (140 − Age) × Weight / (72 × SCr)× 0.85 if female - MDRD equation:
GFR = 1.86 × (SCr)^−1.154 × (Age)^−0.203× 0.742 if female × 1.210 if Black
Key nursing point: A "normal" serum creatinine does not rule out CKD — eGFR can be substantially reduced even when creatinine appears normal, especially in elderly or low-muscle-mass patients.
— Textbook of Family Medicine 9e
Common Causes & Risk Factors
- Diabetes mellitus (leading cause — ~40%)
- Hypertension (second leading cause)
- Glomerulonephritis
- Polycystic kidney disease
- Recurrent UTIs / pyelonephritis
- Nephrotoxic drugs (NSAIDs, aminoglycosides, contrast agents)
- Cardiovascular disease (shared risk factors)
- Tobacco use
Assessment & Monitoring (Nursing Priorities)
Laboratory Values to Monitor
| Lab | Normal | CKD Concern |
|---|---|---|
| eGFR | ≥ 60 | < 60 for ≥ 3 months |
| Serum creatinine | 0.6–1.2 mg/dL | Rising trend |
| BUN (Blood Urea Nitrogen) | 7–20 mg/dL | Elevated → uremia |
| Potassium | 3.5–5.0 mEq/L | Hyperkalemia risk |
| Phosphate | 2.5–4.5 mg/dL | Elevated in CKD |
| Calcium | 8.5–10.5 mg/dL | Low (hypocalcemia) |
| Hemoglobin | ≥ 12 g/dL | Anemia of CKD |
| Albumin | 3.5–5.0 g/dL | Low → malnutrition |
| HbA1c | < 7% (diabetics) | Poor control accelerates CKD |
| Urine albumin-to-creatinine ratio (UACR) | < 30 mg/g | ≥ 30 = albuminuria |
Diagnostic Workup
- Complete urinalysis (protein, casts, RBCs)
- Renal ultrasound (size, echogenicity, obstruction)
- Serum electrolytes, creatinine, albumin
- UACR on spot urine sample
Complications: The "AEIOU" Mnemonic
1. Anemia
- Due to decreased erythropoietin (EPO) production
- Treated with erythropoiesis-stimulating agents (ESAs, e.g., epoetin alfa) and IV iron
- Target Hgb: 10–12 g/dL (avoid > 13 g/dL due to CV risk)
2. Electrolyte & Acid-Base Disturbances
- Hyperkalemia — life-threatening; restrict dietary potassium; use kayexalate or patiromer
- Metabolic acidosis — treat with oral sodium bicarbonate if bicarbonate < 22 mEq/L
- Hyperphosphatemia — use phosphate binders (calcium carbonate, sevelamer) with meals
3. Immune & Infection Risk
- Impaired leukocyte function → increased infection susceptibility
- Ensure vaccinations: pneumococcal, influenza, hepatitis B (give early — response declines with lower eGFR)
4. Osteodystrophy (CKD-MBD)
- Elevated phosphate → suppressed calcitriol (active Vit D) → secondary hyperparathyroidism → bone disease
- PTH monitoring; activated Vit D supplementation (calcitriol)
5. Uremia (advanced CKD/Stage 5)
- Accumulation of urea and uremic toxins
- Symptoms: nausea, vomiting, confusion, pruritus, pericarditis, asterixis ("uremic flap")
- Indicates need for dialysis initiation
Additional Complications
- Hypertension (contributes to and results from CKD — vicious cycle)
- Cardiovascular disease (leading cause of death in CKD)
- Fluid overload / edema — monitor weight daily, assess for pulmonary edema
- Malnutrition — protein-energy wasting common in advanced CKD
Medical Management (Key Medications)
| Drug Class | Example | Purpose |
|---|---|---|
| ACE inhibitors / ARBs | Lisinopril, losartan | Slow CKD progression (especially with diabetes/proteinuria) |
| SGLT-2 inhibitors | Empagliflozin, dapagliflozin | Nephroprotection in diabetic CKD |
| Loop diuretics | Furosemide | Fluid/edema management |
| Phosphate binders | Sevelamer, calcium carbonate | Hyperphosphatemia |
| ESAs | Epoetin alfa | Anemia of CKD |
| IV Iron | Ferric gluconate | Iron deficiency + anemia |
| Sodium bicarbonate | Oral | Metabolic acidosis |
| Antihypertensives | Amlodipine, metoprolol | BP < 130/80 mmHg target |
Nursing alert: Many medications require dose adjustment or are contraindicated in CKD (e.g., metformin, NSAIDs, certain antibiotics). Always check eGFR before administering renally-cleared drugs.
Dietary & Fluid Management
| Restriction | Rationale |
|---|---|
| Protein restriction (~0.6–0.8 g/kg/day in non-dialysis) | Reduces urea load and slows progression |
| Potassium restriction | Prevent hyperkalemia |
| Phosphorus restriction | Prevent renal osteodystrophy |
| Sodium restriction (< 2 g/day) | BP control and fluid management |
| Fluid restriction | Individualized — important in advanced CKD and dialysis patients |
Diet is an underused strategy for preventing CKD progression to ESKD. — Brenner and Rector's The Kidney
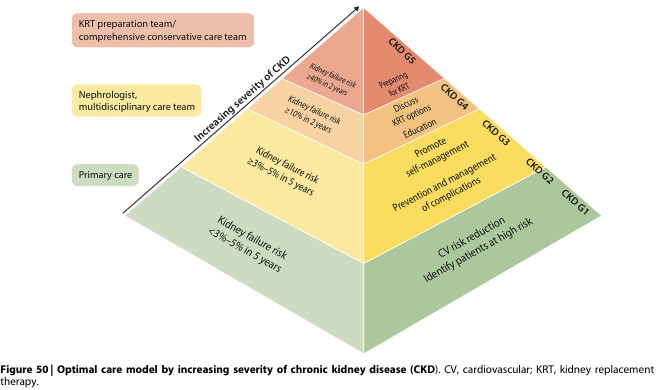
Renal Replacement Therapy (RRT) — Preparing Patients
Patients with Stage 4 CKD (eGFR < 30) should be educated and prepared for RRT options:
1. Hemodialysis (HD)
- Blood filtered via dialyzer 3× per week (~4 hrs/session)
- Requires arteriovenous fistula (AVF), graft, or central venous catheter access
- Nursing: monitor pre/post vitals, weight, vascular access site, hypotension, cramps
2. Peritoneal Dialysis (PD)
- Peritoneum acts as dialysis membrane
- Patient performs exchanges at home (CAPD or APD)
- Nursing: teach sterile technique for exchanges, exit-site care, signs of peritonitis
3. Kidney Transplantation
- Best long-term outcomes; requires immunosuppression
- Pre-transplant workup begins early at Stage 4–5
4. Conservative Management
- For patients who decline dialysis; focused on symptom management and quality of life
Nursing Care Priorities Summary
🔍 Assessment
- Daily weight (fluid status)
- BP and HR (target < 130/80 mmHg)
- Urine output (oliguria/anuria = concern)
- Edema: peripheral, pulmonary
- Skin: pallor (anemia), pruritus (uremia), bruising
- Neurological: confusion, asterixis (uremia)
- Pain, fatigue, dyspnea
🩺 Nursing Diagnoses
- Excess fluid volume r/t decreased urine output
- Risk for electrolyte imbalance (hyperkalemia, acidosis)
- Imbalanced nutrition: less than body requirements
- Activity intolerance r/t anemia
- Deficient knowledge r/t disease management and diet
- Risk for infection (access site, decreased immunity)
📋 Patient Education Priorities
- Diet: low potassium, phosphorus, sodium, and protein
- Medications: importance of adherence; avoid NSAIDs and nephrotoxins
- Fluid management: daily weights, fluid targets
- Dialysis access care (fistula/graft/PD catheter)
- Signs of complications: worsening edema, dyspnea, palpitations (hyperkalemia)
- Vaccinations (hep B, flu, pneumococcal)
- BP monitoring at home
- Referrals: dietitian, social work, nephrology
📊 Referral Triggers
- eGFR < 30 → refer to nephrologist
- eGFR < 20 → begin RRT planning and vascular access placement
- eGFR < 15 → initiate dialysis or conservative care planning
Sources
- Textbook of Family Medicine, 9e (Brenner & Rector approach)
- Brenner and Rector's The Kidney, 2-Volume Set
- Acute Kidney Injury: Prevention, Detection and Management
- Evaluation and Management of Chronic Kidney Disease
This is a shared conversation. Sign in to Orris to start your own chat.