Apd apparatus procedure and diagrams
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
APD automated peritoneal dialysis apparatus procedure cycler diagram
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC4311757
Here is a comprehensive overview of APD (Automated Peritoneal Dialysis) - its apparatus, procedure, and diagrams.
Automated Peritoneal Dialysis (APD)
What is APD?
APD (also called Continuous Cycling Peritoneal Dialysis, CCPD) is a form of renal replacement therapy for end-stage kidney disease (ESKD). Unlike CAPD (Continuous Ambulatory PD, which is done manually during the day), APD uses a machine called a cycler to automatically perform fluid exchanges - typically overnight while the patient sleeps (8-12 hours).
About 60% of PD patients in the US choose APD/CCPD over manual CAPD. - Automated cyclers in PD, PMC
APD Apparatus (Equipment)
The APD Cycler Machine
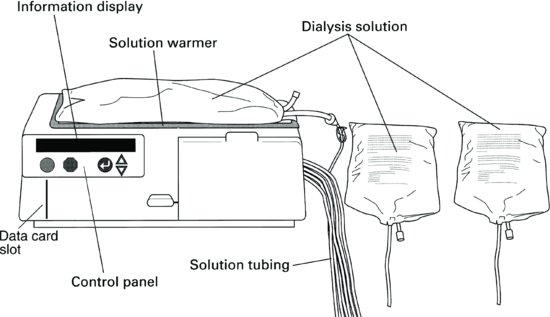
The cycler is the central piece of equipment. Its main components are:
| Component | Function |
|---|---|
| Information display | Shows treatment status, alarms, volume data |
| Control panel | Allows programming of prescription parameters |
| Solution warmer / heater bag | Warms dialysate to body temperature (~37°C) before infusion |
| Data card slot | Stores therapy data for the last 30-90 days; downloaded at clinic visits |
| Solution tubing / cassette | Directs fluid flow between bags, heater, and patient |
| Dialysis solution bags | 10-15 liters of dialysate loaded at the start of each session |
| Effluent/drain bag | Collects used dialysate after each dwell |
| Patient line | Connects the cycler to the patient's peritoneal catheter |
Key brands include Baxter (HomeChoice/Amia series) and Fresenius Medical Care (Sleep•Safe / Newton IQ). Both offer digital card technology for remote data transmission.
The Peritoneal Access Catheter (Tenckhoff Catheter)
The catheter is the permanent abdominal access through which dialysate flows in and out. Features:
- Made of silicone rubber or polyurethane
- Most common design: double-cuff, swan-neck, coiled Tenckhoff catheter
- The coiled intraperitoneal tip sits near the pouch of Douglas (prevents migration, reduces infusion pain)
- Inner cuff anchors in the rectus abdominis muscle (prevents leaks)
- Outer cuff sits in subcutaneous tissue (acts as a barrier against exit-site infection)
- Swan-neck design keeps the exit site pointing downward/laterally (reduces cuff extrusion and infection)
Diagram: Peritoneal Dialysis Setup
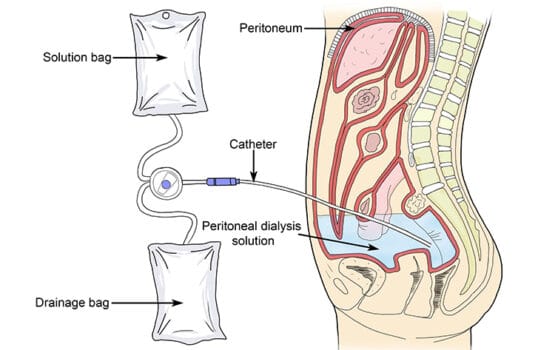
The diagram above shows how dialysis solution from the bag flows through the catheter into the peritoneal cavity, dwells against the peritoneum (the natural membrane acting as a filter), and drains out into a drainage bag - carrying waste products and excess fluid with it.
Catheter Insertion Procedure
Three main techniques are used:
1. Fluoroscopic + Ultrasound Technique (Interventional Nephrology)
(Brenner and Rector's The Kidney)
- Abdomen prepped and draped in sterile fashion; conscious sedation given (midazolam + fentanyl)
- Insertion site: 2 cm left or right and below the umbilicus
- A 21-gauge needle guided under ultrasound (5-12 MHz transducer) through: skin → subcutaneous tissue → rectus fascia → rectus muscle → inner fascia → parietal peritoneum
- 3-5 mL radiocontrast injected under fluoroscopy to confirm peritoneal placement (outer bowel delineation pattern)
- A 0.018-inch cope-mandrel wire inserted through the needle; needle exchanged for a 6-French catheter sheath
- 2 cm skin incision made; subcutaneous tissue digitally dissected to rectus muscle
- Serial dilators (8, 12, 14-French) passed over stiff glide-wire; 18-French peel-away sheath placed
- Double-cuff swan-neck Tenckhoff catheter introduced over glide-wire; coiled tip placed in lower abdominal cavity
- Inner cuff pushed into rectus muscle; tunnel created with exit site distal, lateral, and below the incision
- Final fluoroscopic image taken to verify placement
- Inflow/outflow tested with 500 mL normal saline; catheter flushed with 10-15 mL heparin
- Wound sutured and dressed
- Catheter NOT used for 10-14 days to allow healing; PD usually started 2-4 weeks post-insertion
2. Peritoneoscopic Technique (Y-TEC)
Catheter inserted through the rectus muscle using a peritoneoscope for direct visual confirmation of peritoneal entry. Same skin prep as above; 500 mL air is insufflated into the cavity for visualization.
3. Surgical / Laparoscopic Technique
Performed in the operating theatre, preferred for patients with prior abdominal surgery or adhesions.
APD Treatment Procedure (Each Session)
Setup (Before Bed)
- Wash hands thoroughly; prepare a clean work surface
- Connect 10-15 liters of dialysis solution bags to the cycler tubing/cassette
- Load the cassette into the cycler
- Program the cycler with the prescribed settings: fill volume, number of cycles, dwell time, total therapy duration
- Connect the patient line to the peritoneal catheter using aseptic technique
The Cycler Cycle - Three Phases
Initial Drain (I-Drain)
↓
┌──────────────────────────────────┐
│ FILL → Dialysate pumped │
│ into peritoneal │ × Repeated
│ cavity │ several
├──────────────────────────────────┤ cycles
│ DWELL → Fluid dwells; waste │ overnight
│ and fluid cross │
│ peritoneal membrane │
├──────────────────────────────────┤
│ DRAIN → Used dialysate │
│ pumped to effluent │
│ bag │
└──────────────────────────────────┘
↓
Last fill (optional daytime dwell)
↓
Disconnect in the morning
Step-by-step:
- Initial Drain - cycler first empties any existing fluid from the peritoneal cavity
- Fill phase - fresh dialysate (warmed to body temperature) flows into the abdomen via the patient line; cassette pumps measure exact fill volume
- Dwell phase - fluid remains in the cavity for a set time; uremic toxins (urea, creatinine) and excess water diffuse across the peritoneal membrane into the dialysate by osmosis/diffusion
- Drain phase - used dialysate pumped out into effluent bag; ultrafiltrate volume calculated
- Cycle repeats 4-6 times over 8-12 hours
- Last fill (optional) - the final bag of fresh dialysate may be left in the abdomen as a daytime dwell ("wet day"), or the patient disconnects with an empty abdomen ("dry day") - depends on prescription
Modes of APD
| Mode | Description |
|---|---|
| CCPD (standard APD) | Multiple overnight cycles + optional daytime dwell |
| NIPD | Nocturnal intermittent PD - cycles overnight, dry during the day |
| Tidal PD (TPD) | Only partial drain each cycle (leaves a "tidal" volume) - reduces discomfort and improves efficiency |
| Hi-Dose CCPD / TPD | Higher fill volumes or more exchanges for patients needing increased clearance |
| IPD | Intermittent PD - done 3-4 times/week in a clinical setting |
Prescription Parameters
Each patient's cycler is programmed with:
- Fill volume (typically 1.5-3 L per cycle)
- Number of exchanges (usually 3-6 per night)
- Dwell time per cycle
- Total therapy duration (8-12 hours)
- Dialysate concentration (glucose 1.5%, 2.5%, or 4.25% - higher glucose = more fluid removal by osmosis)
Key Advantages of APD over CAPD
- Exchanges happen during sleep - daytime is free for work/activities
- Reduced risk of peritonitis (fewer manual connections during the day)
- Automated measurement of ultrafiltration volumes
- Remote data monitoring via digital card / cloud-based systems (healthcare team can review treatment data between visits)
References
- Brenner and Rector's The Kidney (9780323532655), Chapter 68: Peritoneal Dialysis - Catheter Procedures, pp. 2914-2916
- Automated cyclers used in peritoneal dialysis - PMC/NIH
- Mayo Clinic - Peritoneal Dialysis
Intermittent pd apparatus procedure and diagrams
Finding Sources
Searching the Web
intermittent peritoneal dialysis IPD apparatus procedure diagram cycler manual
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading Web Page
https://www.merckmanuals.com/professional/nephrology/renal-r…
Finding Sources
Finding Sources
Reading File
Loading Image
Excellent - I now have comprehensive textbook content, diagrams, and clinical detail. Here is the full answer:
Intermittent Peritoneal Dialysis (IPD)
Overview
IPD is the oldest and simplest form of peritoneal dialysis. Unlike continuous methods (CAPD/APD), IPD is scheduled and interrupted - dialysis sessions are performed for a defined number of hours, after which the peritoneal cavity is left completely dry between sessions. It is primarily used for acute kidney injury (AKI) and for patients newly starting PD who still have residual kidney function (RKF).
IPD has largely fallen out of favor for chronic ESKD due to concerns about inadequate small solute clearance, replaced by more efficient APD/CCPD techniques. - Merck Manual - Peritoneal Dialysis
Diagram 1: IPD Apparatus Setup - Tenckhoff Catheter and Gravity Drainage

This diagram shows:
- Left panel: Cross-section of the Tenckhoff catheter passing through skin, fat, muscle, and peritoneum with two Dacron cuffs securing it in place
- Right panel: The classic IPD gravity setup - dialysate bag hung on an IV pole flows downward by gravity into the peritoneal cavity; effluent drains by gravity into a collection bag below the patient
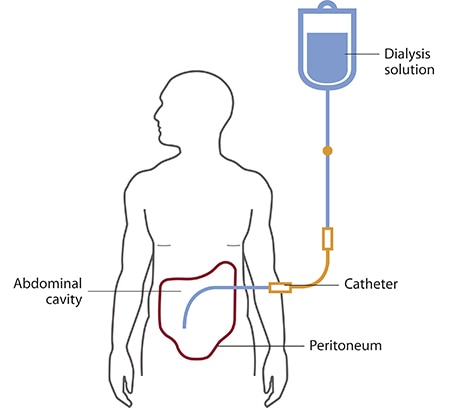
Diagram 2: Anatomical Overview of Peritoneal Dialysis Access
Apparatus
1. Peritoneal Access Catheter
The Tenckhoff catheter is the standard access device. Key features:
| Feature | Detail |
|---|---|
| Material | Silicone rubber or polyurethane |
| Tip design | Straight or coiled (coiled preferred - less migration and pain) |
| Cuffs | Two Dacron cuffs - inner cuff anchors in rectus muscle, outer cuff in subcutaneous tissue |
| Tunnel design | Swan-neck or straight; exit site directed downward/laterally |
| Intraperitoneal tip | Sits in the pouch of Douglas (pelvic cul-de-sac) |
2. Dialysate Solution
- Composition: Glucose-based (1.36%, 2.27%, or 3.86% glucose) or icodextrin; buffered with lactate or bicarbonate; contains electrolytes (Na⁺, Ca²⁺, Mg²⁺, Cl⁻)
- Volume: 2-3 L per exchange in adults; 30-40 mL/kg in children
- Temperature: Warmed to 37°C before infusion (prevents pain and vasoconstriction)
- Packaging: Supplied in sterile PVC bags (1.5 L, 2 L, 2.5 L, 3 L)
3. Delivery System
Manual/Gravity IPD (traditional, especially for AKI):
| Component | Function |
|---|---|
| IV pole / infusion stand | Holds dialysate bag elevated above patient for gravity fill |
| Transfer set / PVC tubing | Connects dialysate bag to catheter; includes roller clamp |
| Spike and Y-connector | Allows fill and drain through same line |
| Drain bag / effluent container | Placed below the patient to collect used dialysate by gravity |
| Warming device | Water bath or dry warmer to pre-warm bags to 37°C |
Automated/Cycler-based IPD (modern):
The APD cycler (e.g., Fresenius Liberty, Baxter HomeChoice) is programmed in "IPD mode":
- Performs all exchanges at night
- Fully drains the peritoneal cavity at the end of the session (dry day)
- No fluid left in the abdomen between sessions
Diagram 3: The Three Phases of One IPD Exchange
FILL PHASE (10-15 min)
┌────────────────────────────────────────────────────┐
│ Dialysate bag (hanging high) → gravity or pump │
│ Fresh 2-3 L dialysate flows into peritoneal │
│ cavity via Tenckhoff catheter │
└────────────────────────────────────────────────────┘
↓
DWELL PHASE (30-40 min)
┌────────────────────────────────────────────────────┐
│ Clamps closed; fluid dwells in peritoneum │
│ Uremic toxins (urea, creatinine, K⁺) diffuse │
│ across peritoneal membrane into dialysate │
│ Excess water removed by osmosis (glucose gradient)│
└────────────────────────────────────────────────────┘
↓
DRAIN PHASE (10-15 min)
┌────────────────────────────────────────────────────┐
│ Drain clamp opened; effluent flows by gravity │
│ (or pump) into collection bag below patient │
│ Peritoneal cavity left COMPLETELY EMPTY (dry) │
└────────────────────────────────────────────────────┘
↓
Cycle repeated multiple times (typically 8-24 cycles)
Total time per exchange cycle = ~55-70 minutes
IPD Procedure - Step by Step
Preparation
- Patient is positioned supine or reclined (recumbency improves drainage)
- Dialysate bags warmed to 37°C (water bath, dry warmer, or cycler heater bag)
- Hands washed thoroughly; sterile field prepared
- Catheter exit site inspected for signs of infection
- Transfer set spiked onto dialysate bag aseptically; tubing primed to remove air
Exchange Technique (Manual Gravity)
- Clamp the drain line and open the fill line
- Hang dialysate bag on IV pole above patient level
- Allow 2-3 L to infuse over 10-15 minutes by gravity
- Close fill line when bag is empty
- Patient may move gently to distribute fluid across the peritoneum
- Dwell for 30-40 minutes (clamps closed)
- Open drain line; lower drain bag below patient level
- Drain over 10-15 minutes - peritoneal cavity fully emptied
- Measure effluent volume - compare to fill volume to calculate ultrafiltration
- Inspect effluent: should be clear/straw-colored (cloudy = suspect peritonitis)
- Disconnect drain bag; attach fresh dialysate bag for next exchange
- Repeat cycle as prescribed
Session Duration and Frequency
- Acute IPD (AKI): Multiple exchanges over 12-48 hours continuous; can extend to 72 hours if needed
- Chronic IPD: Historically 3 sessions per week, each lasting 10-14 hours (20-24 exchanges per session); done in hospital/outpatient dialysis unit
- NIPD (Nocturnal IPD - modern variant): Exchanges overnight (8-10 hours) via cycler; cavity left dry during the day; typically every night or 5-6 nights per week
Comparison of IPD Variants
| Parameter | Classic IPD | NIPD (Nocturnal IPD) |
|---|---|---|
| Setting | Hospital / outpatient unit | Home (cycler) |
| Frequency | 3×/week | Nightly (5-7×/week) |
| Session duration | 10-14 hours | 8-10 hours |
| Exchanges/session | 8-24 cycles | 3-6 cycles |
| Fill volume/cycle | 2-3 L | 1.5-2.5 L |
| Daytime fluid | Dry (cavity empty) | Dry (cavity empty) |
| Automation | Manual or cycler | Cycler (APD machine) |
| Main indication | AKI; newly started PD | Chronic PD with RKF; incremental PD |
| Adequacy concern | High (poor clearance in anuric patients) | Better with preserved RKF |
Incremental IPD (Starting PD)
For patients newly starting PD who still have significant residual kidney function, NIPD is the preferred incremental starting option (Comprehensive Clinical Nephrology, 7th Ed.):
- Start with 2-3 overnight exchanges at 1.5 L fill volume per exchange
- As RKF declines, increase fill volumes by 20-30% increments (up to max 2.5 L)
- If more clearance needed: increase number of exchanges
- Eventually add a daytime dwell (converts NIPD → CCPD/APD)
Monitoring During IPD
| Parameter | What to Check |
|---|---|
| Ultrafiltration | Drain volume minus fill volume (positive = fluid removed) |
| Effluent appearance | Clear = normal; cloudy/turbid = peritonitis |
| Blood pressure / weight | Fluid balance |
| Serum electrolytes | K⁺, Na⁺, bicarbonate |
| Glucose | Especially in diabetics (glucose absorbed from dialysate) |
| Kt/V urea | Adequacy target: weekly Kt/V ≥ 1.7 (combined peritoneal + renal) |
Advantages and Limitations of IPD
Advantages
- Simple to set up and perform
- Effective for AKI (no need for systemic anticoagulation unlike hemodialysis)
- Safe in hemodynamically unstable patients
- Lower infection risk vs CAPD (fewer daytime connections)
- NIPD variant allows a free daytime schedule
Limitations
- Inadequate clearance in anuric/oliguric patients (dry day = no continuous dialysis)
- Not recommended for chronic ESKD patients without RKF
- Less efficient than CAPD or CCPD for solute removal
- Requires hospital/clinic attendance (classic IPD)
- Patient remains recumbent during session
References
- Brenner and Rector's The Kidney (9780323532655), Chapter 64: Frequency of Exchanges, p. 2787
- Comprehensive Clinical Nephrology, 7th Edition (9780323825924), Chapter 13: Prescribing Incremental PD, p. 1323
- Merck Manual - Peritoneal Dialysis
- PMC - Automated cyclers in peritoneal dialysis
- Fresenius Liberty Cycler User's Guide (IPD mode description)
This is a shared conversation. Sign in to Orris to start your own chat.