in breech baby presentation tell me the Manoeuvres used, Hands Off and on approach and foetal and maternal Complications
Breech Presentation: Manoeuvres, Hands-Off vs. Hands-On, and Complications
Types of Breech (Quick Orientation)
| Type | Features | Cord Prolapse Risk |
|---|---|---|
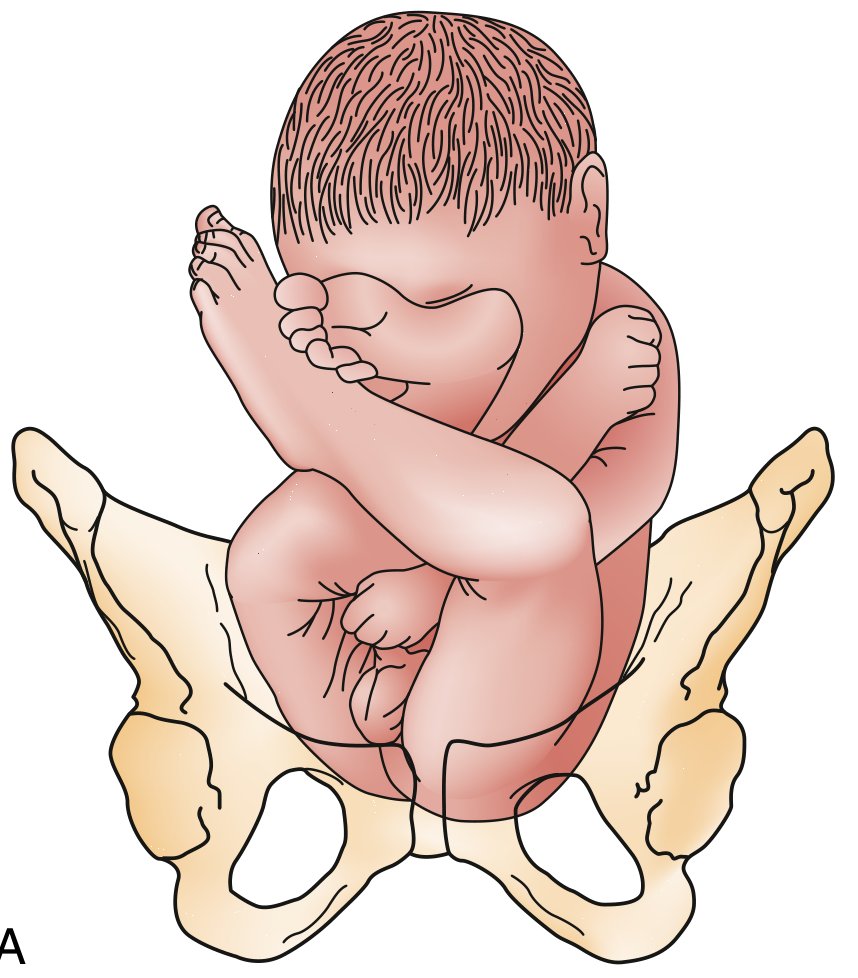
| Frank breech | Hips flexed, knees extended - 60-65% of breeches | ~0.5% |
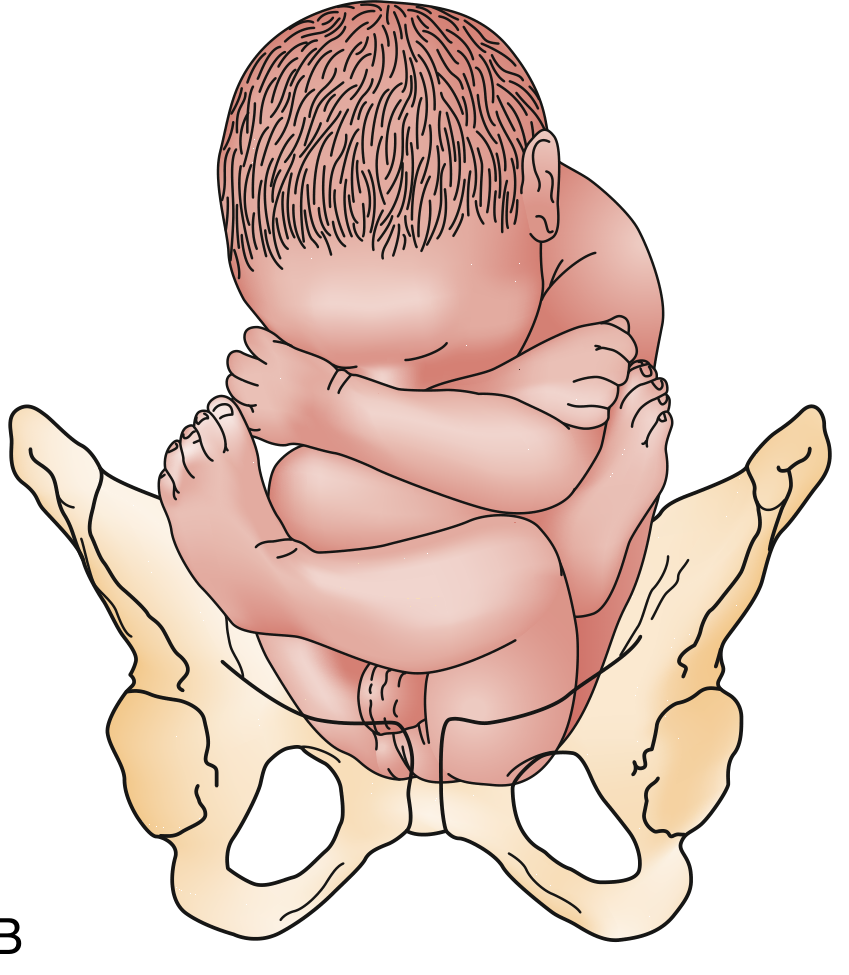
| Complete breech | Hips and knees flexed - ~5% of breeches | ~5-6% |
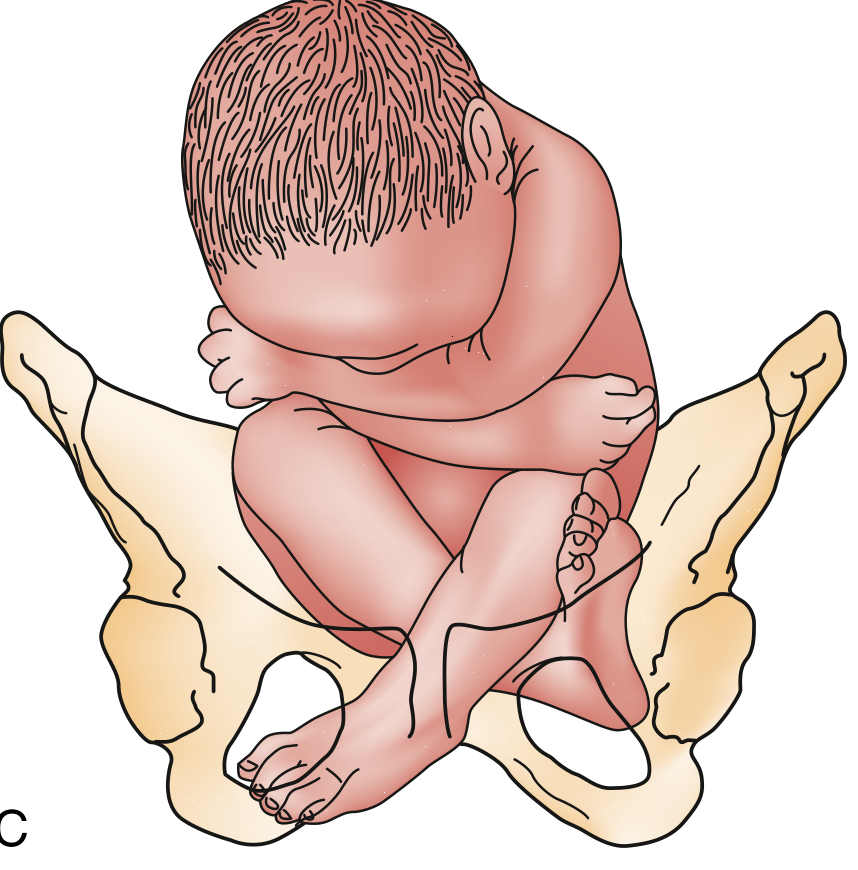
| Incomplete (footling) | Incomplete hip flexion, single/double footling - 25-35% | 15-18% |
Mechanism of Labour in Breech
Manoeuvres in Breech Delivery
1. Delivery of the Legs
- Place two fingers along the fetal femur toward the popliteal fossa
- Abduct and flex the knee to bring the foot down into the vagina
- This converts a frank breech into a footling presentation for delivery
2. Delivery of the Trunk/Shoulders
- Grasp the fetal bony pelvis (thumbs on sacrum, fingers on anterior superior iliac crests) - never grip the abdomen or soft tissues
- Rotate the trunk 180° while maintaining downward traction, bringing the posterior shoulder (which was above the symphysis) to the anterior position
- Sweep the arm down across the chest and deliver it
- Reverse the rotation 180° to deliver the other arm by the same method
- This works because the posterior arm is always below the pelvic brim and can be swept out
3. Delivery of the After-Coming Head
Mauriceau-Smellie-Veit Manoeuvre (most commonly used)
- Rest the fetal body on the clinician's palm and forearm
- Place the index and middle fingers of one hand over the maxilla (not the mandible) to maintain head flexion and draw the chin in
- Hook two fingers of the other hand over the fetal neck, grasping the shoulders
- Apply downward traction until the suboccipital region appears under the symphysis
- Then elevate the body toward the mother's abdomen - this delivers the mouth, nose, brow, and occiput over the perineum
- An assistant can apply suprapubic pressure to help flex and deliver the head
- Avoid excessive elevation (hyperextension of the neck)
Burns-Marshall Method (alternative for after-coming head)
- Allow the baby to hang by its own weight for up to 1-2 minutes to encourage flexion and descent of the head
- Then hold the feet and swing the body in a wide arc upward over the mother's abdomen
- This delivers the chin, mouth, nose, and forehead in sequence over the perineum
- (Note: not favoured as much as Mauriceau because it relies on the neck as a lever)
Piper Forceps
- Applied to the after-coming head when the Mauriceau manoeuvre fails or there is difficulty
- Requires an assistant to hold the body elevated while forceps are applied from below
- Milner's data showed that application of forceps to the after-coming head was associated with reduced neonatal mortality from breech delivery
- Piper forceps should be available even at caesarean section - they can be applied through the uterine incision if there is difficulty extracting the after-coming head
The "Hands-Off" vs "Hands-On" Approach
Hands-Off (Passive / Spontaneous Delivery)
| Principle | Detail |
|---|---|
| Allow spontaneous expulsion to the umbilicus before intervening | Ensures full cervical dilatation and adequate pelvic space |
| Support - do not traction - the presenting part | Premature traction can trap the after-coming head |
| In frank breech: allow descent to the umbilicus before any manipulation | "The mere appearance of feet through the vulva is NOT an indication to proceed" |
| Grip the bony pelvis, not the abdomen | Abdominal pressure can cause liver/splenic injury |
When to Use Hands-On (Active/Assisted Delivery)
- After delivery to the umbilicus - sweep out the legs (Pinard)
- Grasp bony pelvis for trunk rotation with downward traction
- Lovset's manoeuvre for nuchal arms
- Mauriceau manoeuvre for the after-coming head
- Piper forceps if Mauriceau fails
Summary Table
| Hands-Off Scenarios | Hands-On Scenarios |
|---|---|
| Spontaneous descent of buttocks | After umbilicus delivers - assist legs |
| Allow legs to deliver spontaneously | Lovset's for nuchal/extended arms |
| Maternal effort delivering trunk | Grasp bony pelvis for body rotation |
| Waiting for full cervical dilatation | Mauriceau for after-coming head |
| Do NOT rupture membranes prematurely | Piper forceps for failed Mauriceau |
Complications
Fetal / Neonatal Complications
| Complication | Mechanism / Notes |
|---|---|
| Umbilical cord prolapse | Most common in footling breech (15-18%); presenting part does not occlude the os - cord can slip past |
| Entrapment of the after-coming head | Especially in preterm infants (<1500 g) and with CPD; cervix closes around the neck after body delivers |
| Intracranial haemorrhage / tentorial tears | Rapid, uncontrolled delivery of the head; also from inadequate pelvic capacity |
| Brachial plexus injury | Excessive lateral traction during shoulder delivery |
| Nuchal arm entrapment | Arm extends behind the neck, greatly increases dystocia of the head |
| Spinal cord injury | If neck is hyperextended; vaginal delivery with hyperextended neck is associated with a high incidence of cord injuries |
| Birth asphyxia | From cord compression, head entrapment, or traumatic delivery |
| Liver / splenic rupture | Abdominal grip (instead of bony pelvis grip) during extraction |
| Hip dislocation / femur fracture | Inappropriate traction on legs |
| Perinatal death | Overall, one-third of breech fetal deaths are considered preventable; primarily from asphyxia (cord prolapse or head entrapment) |
Maternal Complications
| Complication | Notes |
|---|---|
| Perineal lacerations (3rd/4th degree) | Larger presenting part, need for episiotomy, especially with delivery of after-coming head |
| Cervical and vaginal lacerations | From rapid forceful delivery or instrumentation |
| Postpartum haemorrhage | Higher operative delivery rates; uterine atony following prolonged/traumatic labour |
| Uterine rupture | From obstructed labour, especially with footling or transverse lie |
| Increased caesarean section rate | Primary planned CS is now standard for most term breeches; failed trial of labour leads to emergency CS with higher morbidity |
| Complications of general/regional anaesthesia | More operative deliveries |
| Psychological trauma | Emergency unplanned breech delivery in an obstetric/ED setting |
Key Clinical Pearls
- ECV (External Cephalic Version) at 36 weeks has ~65% success and reduces CS rate by 50% - it is the preferred first step if the fetus is breech at term with intact membranes
- Vaginal breech delivery requires: frank or complete breech, fetal weight 2000-3800 g, normal gynecoid pelvis, and a flexed fetal head
- A hyperextended fetal neck on ultrasound = contraindication to vaginal delivery (high spinal injury risk)
- Oxytocin in breech labour must be used with extraordinary caution - a disproportionate number of perinatal deaths in the Term Breech Trial occurred with oxytocin-augmented labours
- Pull a 10-15 cm loop of cord after the umbilicus clears the perineum to allow working room and prevent cord traction
can all the manoeuvres in picture form
Medical obstetrics illustration: Pinard's Manoeuvre for breech delivery. Clean clinical diagram showing two fingers placed along the fetal femur reaching into the vagina toward the popliteal fossa. Arrow shows knee being flexed and foot swept down and out of the birth canal. Labels: "2 fingers along femur", "Flex knee", "Foot swept down". Title at top: "PINARD'S MANOEUVRE - Frank Breech Leg Delivery". White background, blue and red anatomical color scheme, professional medical textbook style.
Medical obstetrics illustration: Lovset's Manoeuvre for breech delivery - nuchal arm delivery. Three-panel diagram. Panel 1: baby body delivered to shoulders, arms extended/nuchal. Panel 2: clinician grips bony pelvis (thumbs on sacrum, fingers on iliac crests) and rotates trunk 180 degrees with downward traction - curved arrow shows rotation direction. Panel 3: posterior arm now anterior, two fingers sweep arm down across chest and deliver it. Labels: "Grip bony pelvis only", "180° rotation + downward traction", "Sweep arm across chest". Title: "LOVSET'S MANOEUVRE - Nuchal/Extended Arm Delivery". White background, professional medical illustration style, blue and pink tones.
Medical obstetrics illustration: Mauriceau-Smellie-Veit Manoeuvre for after-coming head in breech delivery. Side view clinical diagram. Baby body resting on clinician's forearm and palm, face down. One hand: index and middle fingers placed on maxilla (upper jaw) maintaining head flexion - labeled "Fingers on MAXILLA (not mandible)". Other hand: two fingers hooked over back of fetal neck grasping shoulders - labeled "Hook fingers over neck". Large arrows: first pointing downward labeled "1. Downward traction until suboccipital region at symphysis", then curved upward labeled "2. Elevate body toward abdomen". Symphysis pubis bone visible as landmark. Assistant applying suprapubic pressure shown. Title: "MAURICEAU-SMELLIE-VEIT MANOEUVRE - After-Coming Head". White background, professional medical textbook illustration, blue/red anatomical colors.
Medical obstetrics illustration: Burns-Marshall Method for after-coming head in breech delivery. Two-panel side view diagram. Panel A: Baby hanging by own weight - labeled "Allow to hang 1-2 minutes for gravity-assisted descent and head flexion". Panel B: Clinician holds both ankles and swings baby body in wide upward arc over mother's abdomen - large curved arrow showing the arc movement - labeled "Swing body upward over abdomen". Sequential face delivery shown: chin, mouth, nose, forehead delivered over perineum. Warning note: "Do NOT use if head not engaged". Title: "BURNS-MARSHALL METHOD - After-Coming Head". White background, professional medical illustration, blue and pink color scheme.
Medical obstetrics illustration: Piper Forceps application to after-coming head in breech delivery. Clinical diagram showing assistant holding baby body elevated upward with hands (labeled "Assistant elevates body"). Clinician below applies long-handled Piper forceps blades to sides of after-coming fetal head from below. Forceps handles pointing downward and forward. Labels: "Piper forceps blades applied to sides of head", "Applied BELOW the baby's body", "Traction downward then arc upward". Small inset showing Piper forceps instrument shape. Title: "PIPER FORCEPS - Failed Mauriceau / Difficult After-Coming Head". White background, professional medical textbook illustration style.
Medical obstetrics illustration: Breech delivery trunk grip and shoulder delivery sequence. Two panels. Panel A: Correct bony pelvis grip - clinician's hands shown with thumbs on sacrum and fingers on anterior superior iliac crests. Large red X over incorrect soft tissue/abdominal grip. Label: "CORRECT: Thumbs on sacrum, fingers on ASIS" and "WRONG: Never grip abdomen (causes organ injury)". Panel B: Shoulder delivery - scapulae visible, trunk rotated to bring anterior arm to vulva, two fingers sweep arm across chest. Then reverse rotation for second arm. Labels with step numbers. Title: "TRUNK GRIP & SHOULDER DELIVERY". White background, professional clinical illustration, clear anatomical labels, blue/red color scheme.
Breech Manoeuvres - Picture Guide
Breech Types (from Rosen's Emergency Medicine)
Manoeuvre 1 - PINARD'S MANOEUVRE
Used for: Frank breech - converting to footling to deliver legs
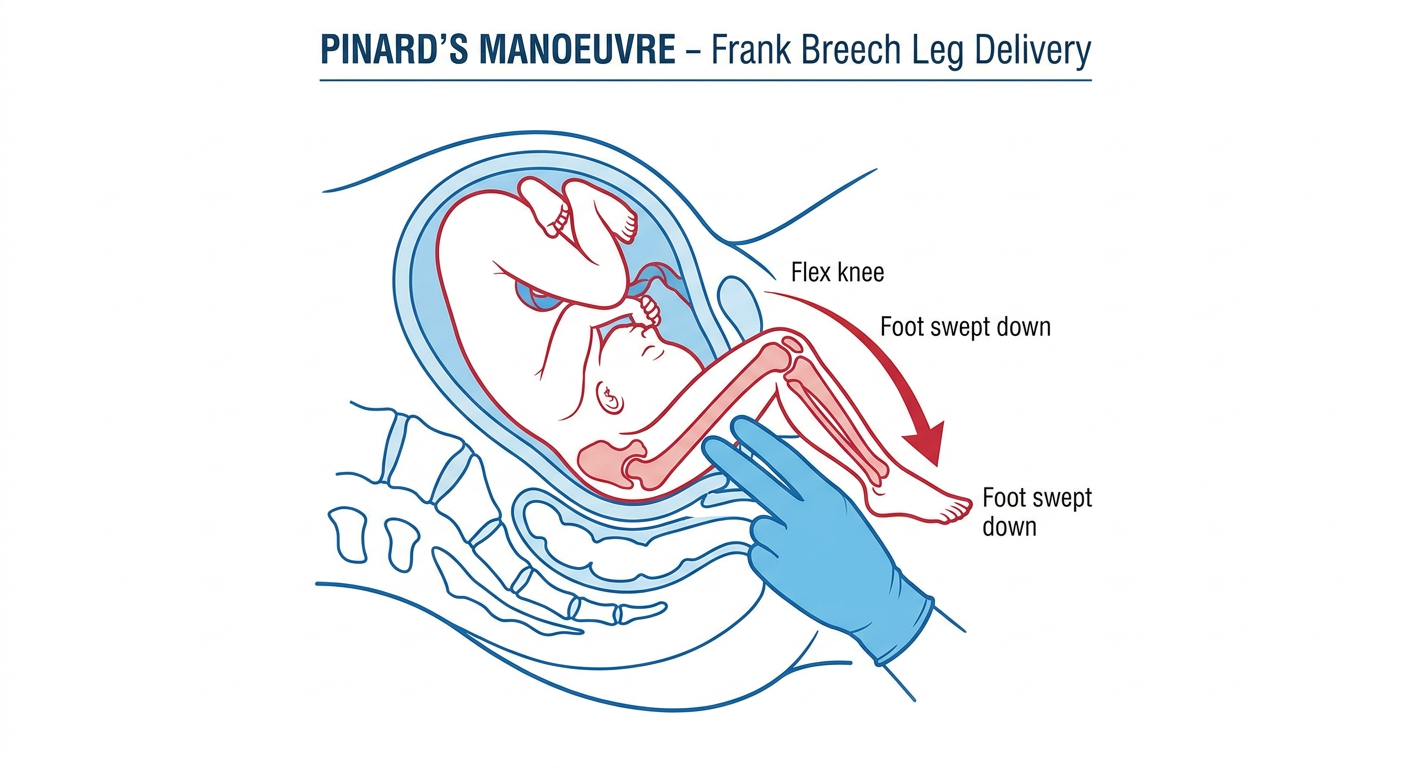
Steps: Two fingers along femur → reach popliteal fossa → abduct and flex the knee → foot swept down into vagina. Do this for each leg.
Manoeuvre 2 - LOVSET'S MANOEUVRE
Used for: Nuchal / extended arms - prevents arm entrapment
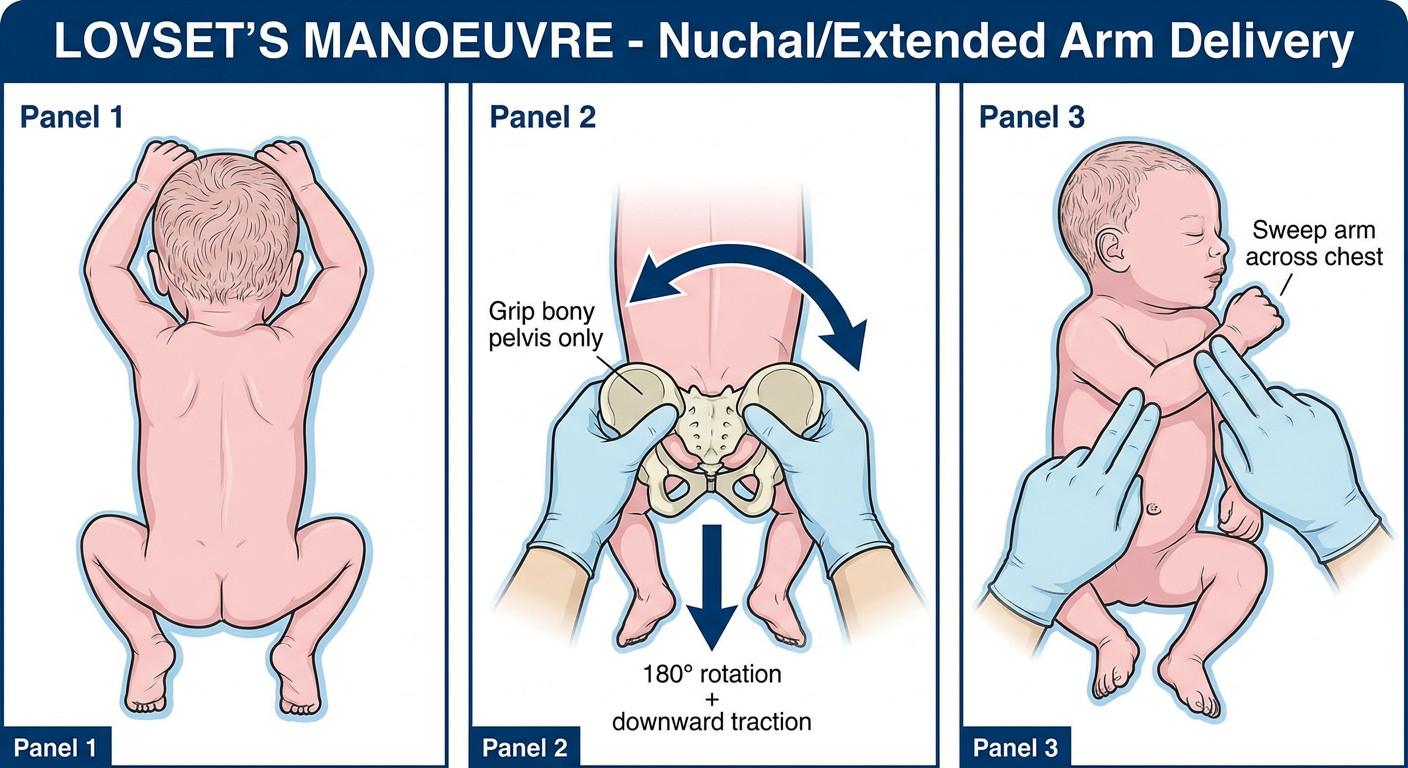
Steps: Grip bony pelvis (thumbs on sacrum, fingers on iliac crests) → rotate trunk 180° with downward traction → posterior arm becomes anterior → sweep arm across chest → reverse 180° for the other arm.
Manoeuvre 3 - TRUNK GRIP & SHOULDER DELIVERY
Used for: Delivering trunk and shoulders safely
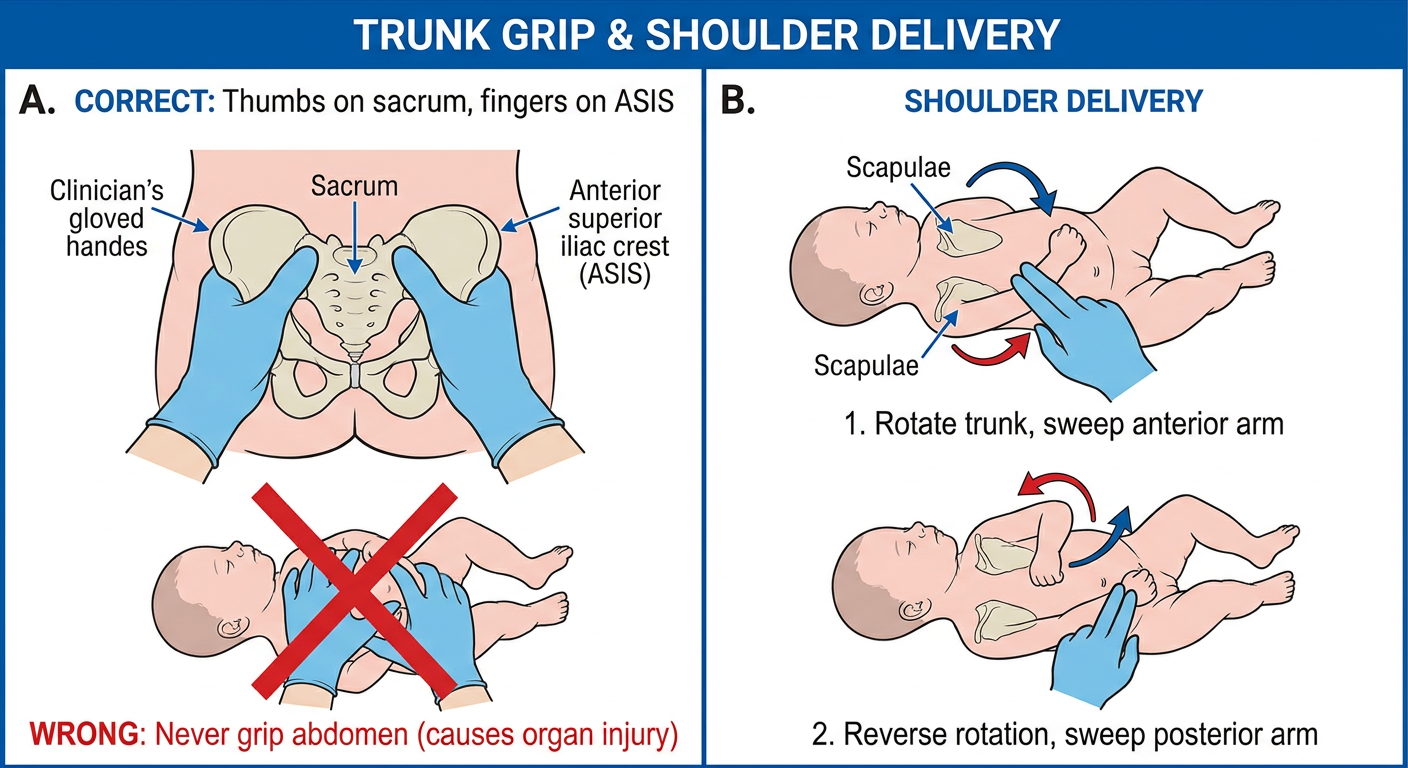
Key rule: ALWAYS grip the bony pelvis - thumbs on sacrum, fingers on ASIS. NEVER grip the abdomen (causes liver/spleen rupture). Wrap body in a towel for grip.
Manoeuvre 4 - MAURICEAU-SMELLIE-VEIT MANOEUVRE
Used for: Delivering the after-coming head (first-line)
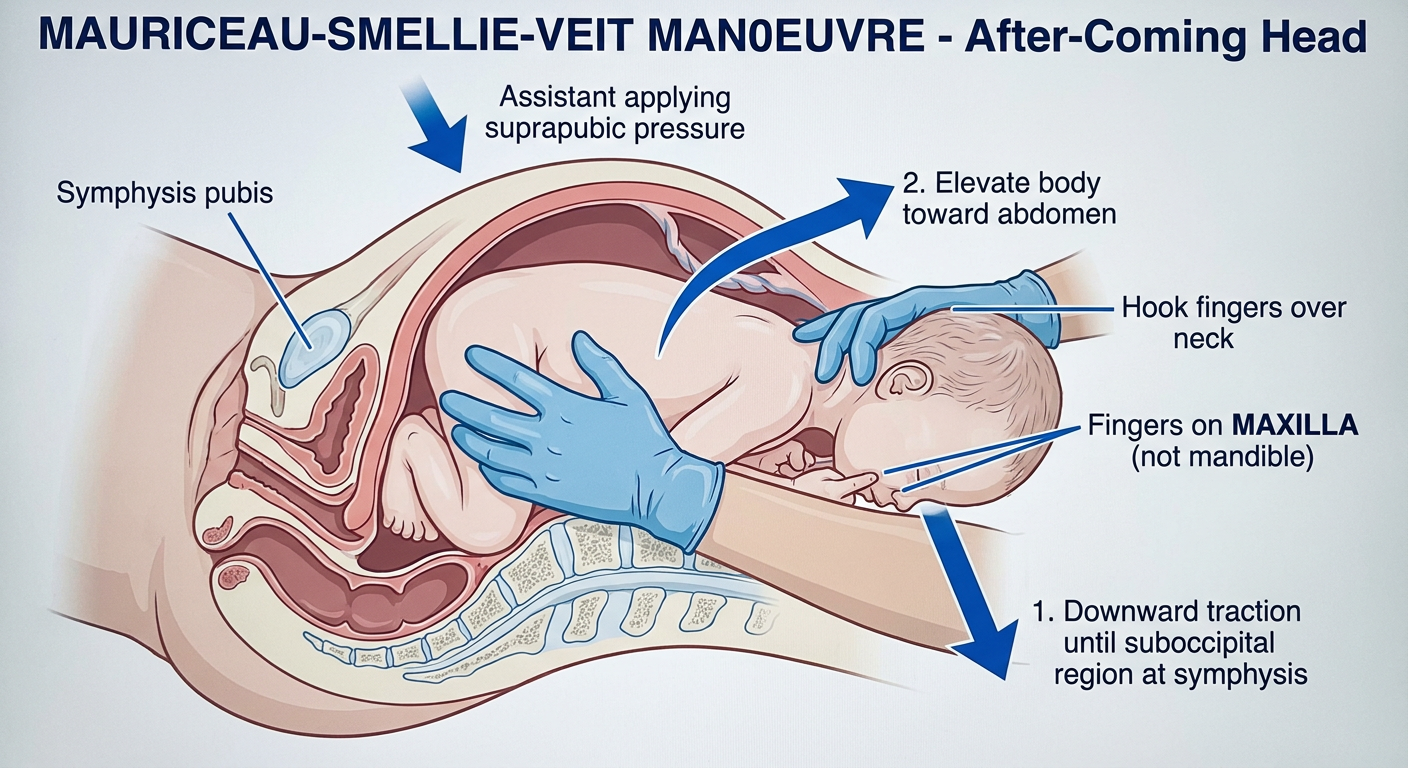
Steps: Body rests on forearm → index + middle fingers on maxilla (not mandible!) to flex head → other hand hooks two fingers over back of neck → downward traction until subocciput under symphysis → elevate body toward abdomen → mouth, nose, brow, occiput deliver. Assistant can apply suprapubic pressure.
Manoeuvre 5 - BURNS-MARSHALL METHOD
Used for: Delivering the after-coming head (alternative)
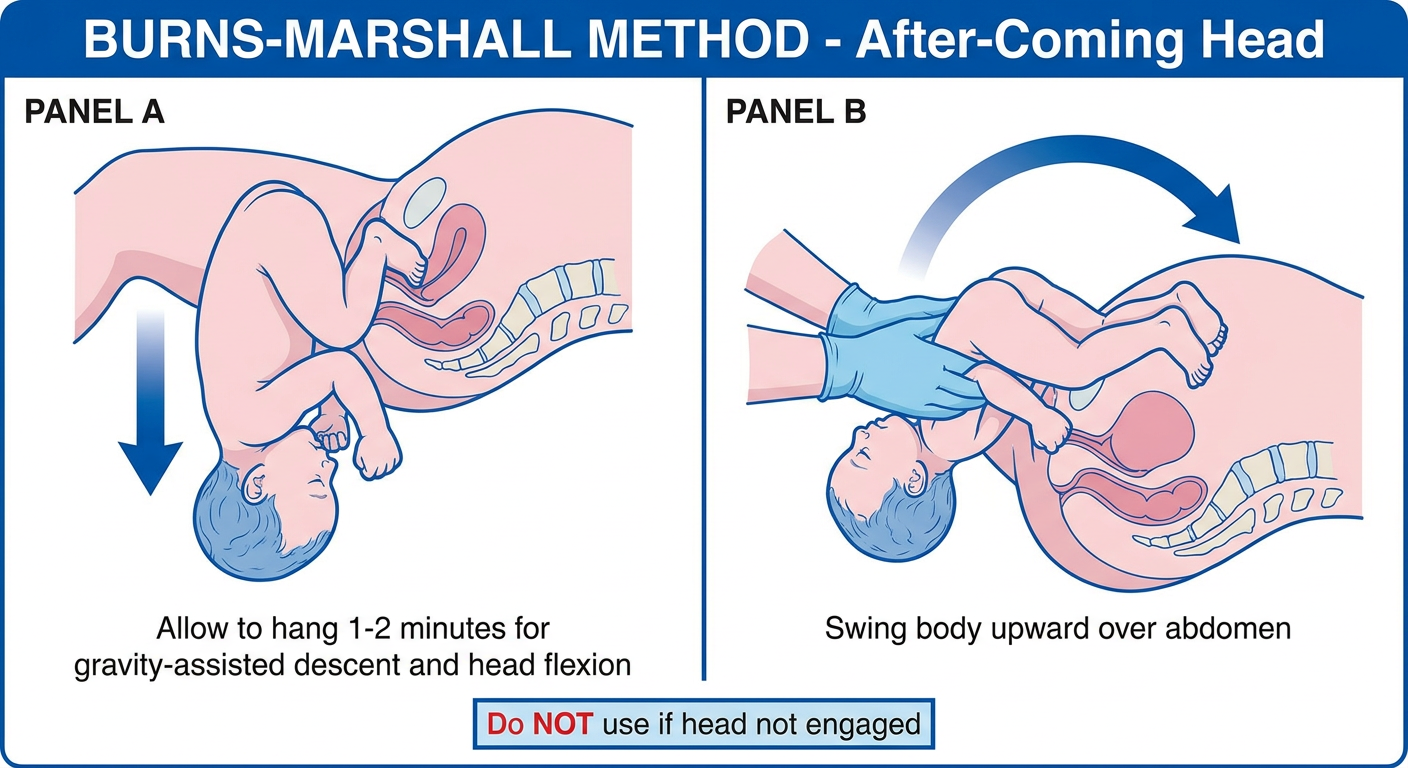
Steps: Allow baby to hang by own weight 1-2 minutes (gravity assists head descent and flexion) → grasp both ankles → swing body in a wide arc upward over mother's abdomen → chin, mouth, nose, forehead deliver over perineum sequentially.
Manoeuvre 6 - PIPER FORCEPS
Used for: After-coming head when Mauriceau fails
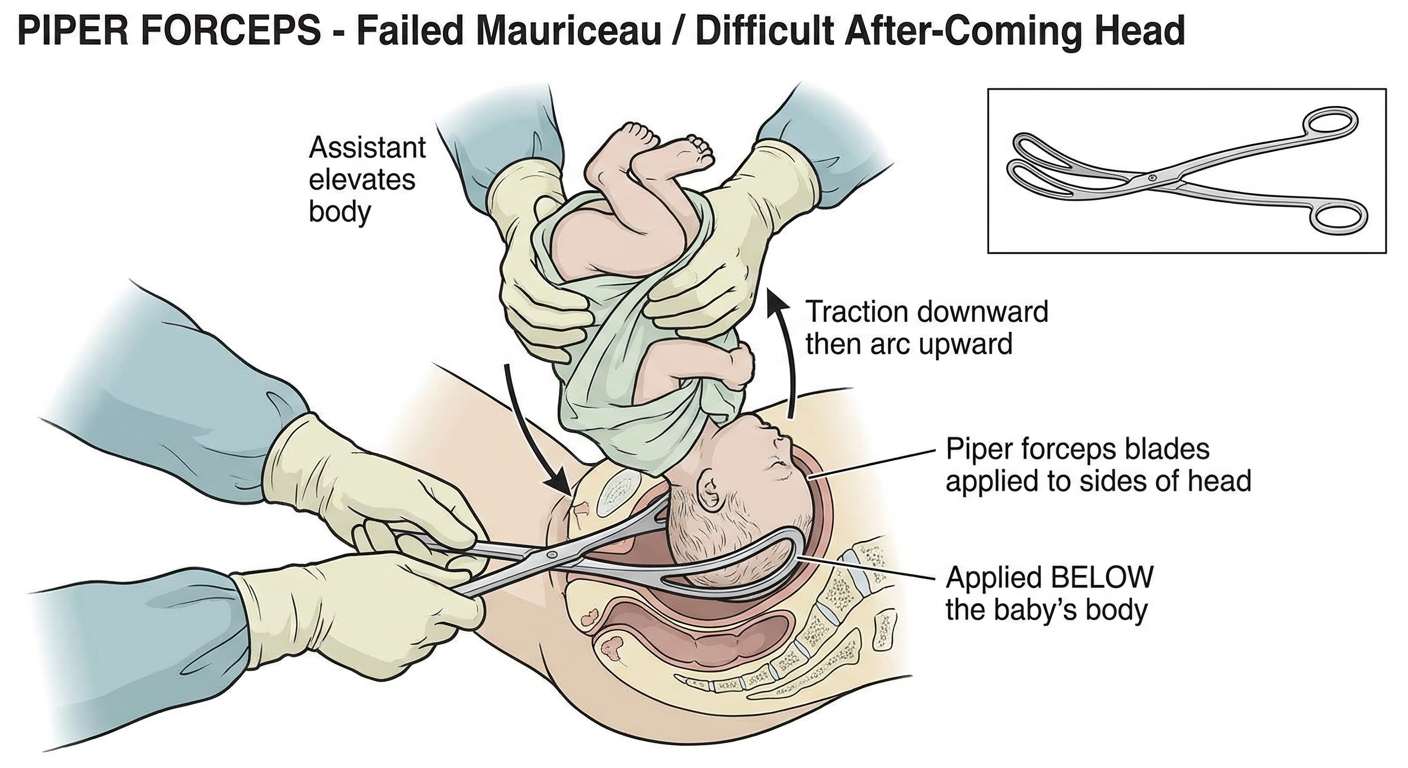
Steps: Assistant holds baby body elevated upward → clinician applies Piper forceps blades to sides of the head from below → traction downward first, then arc upward to deliver head. Also used through uterine incision at caesarean if head delivery is difficult.
Summary Sequence
LEGS born → PINARD'S (frank breech)
↓
TRUNK descends → LOVSET'S (if arms nuchal/extended)
↓
SHOULDER DELIVERY → correct bony pelvis grip + rotation
↓
AFTER-COMING HEAD → MAURICEAU-SMELLIE-VEIT (first line)
→ BURNS-MARSHALL (alternative)
→ PIPER FORCEPS (if above fail)