Explain me 10 common heart diseases with ECG charts and ECG images of those diseases
Reading File
Finding Sources
Searching the Web
common heart diseases ECG patterns with images atrial fibrillation MI heart block
Finding Sources
Finding Sources
Searching the Web
ECG image STEMI atrial fibrillation ventricular tachycardia heart block site:litfl.com OR site:ecgwaves.com
Reading File
Reading Web Page
https://litfl.com/inferior-stemi-ecg-library
Loading Image
Loading Image
Loading Image
Searching the Web
ECG images site:litfl.com atrial flutter ventricular fibrillation bradycardia sinus tachycardia WPW Brugada
Loading Image
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Finding Sources
Searching the Web
ECG electrocardiogram 10 common arrhythmias labeled diagram free medical education
Loading Image
Reading File
Loading Image
I now have all the material I need. Let me compile the comprehensive guide:
10 Common Heart Diseases: ECG Patterns & Images
Below is a detailed guide to 10 common cardiac conditions, each with their ECG characteristics and visual references.
Understanding the ECG Baseline
Before diving in, a quick reference on normal ECG components:
- P wave = atrial depolarization
- PR interval = AV conduction time (normal: 0.12-0.20 sec)
- QRS complex = ventricular depolarization (normal: <0.12 sec)
- ST segment = early ventricular repolarization
- T wave = ventricular repolarization
1. Atrial Fibrillation (AF)
What it is: The most common sustained cardiac arrhythmia. Chaotic, disorganized electrical activity in the atria replaces the normal coordinated atrial contraction.
Causes: Heart failure, hypertension, coronary artery disease, hyperthyroidism, COPD, alcohol use, mitral valve disease.
Symptoms: Palpitations, fatigue, dyspnea, dizziness; can be asymptomatic. Major risk of stroke from atrial thrombus formation.
ECG Features:
- No distinct P waves - replaced by fine, irregular fibrillatory baseline (f waves at 300-600 bpm)
- Irregularly irregular RR intervals (the hallmark)
- QRS complexes are usually narrow and normal morphology
- Ventricular rate typically 100-180 bpm if uncontrolled
ECG Image - Atrial Fibrillation (Lead II):
Note the irregularly spaced QRS complexes with no visible P waves - only chaotic baseline activity

Source: Guyton and Hall Textbook of Medical Physiology - Fig. 13.20. The waves visible are ventricular QRS and T waves only; no organized P waves are present.
Treatment: Rate control (beta-blockers, calcium channel blockers), rhythm control (cardioversion, antiarrhythmics), anticoagulation (warfarin or DOACs) to prevent stroke.
2. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery causing full-thickness myocardial necrosis. A medical emergency requiring immediate reperfusion.
Causes: Atherosclerotic plaque rupture with superimposed thrombosis, coronary vasospasm (Prinzmetal angina).
Symptoms: Severe crushing chest pain radiating to arm/jaw, diaphoresis, nausea, shortness of breath.
ECG Features (Rosen's Emergency Medicine):
- ST segment elevation >1 mm in 2+ contiguous leads (the defining feature)
- Hyperacute T waves (tall, peaked) - earliest sign
- Q waves develop over hours (irreversible necrosis)
- Reciprocal ST depression in opposite leads
- Location by leads:
- Anterior STEMI: ST elevation in V1-V4 (LAD territory)
- Inferior STEMI: ST elevation in II, III, aVF (RCA or LCx territory)
- Lateral STEMI: ST elevation in I, aVL, V5-V6
ECG Image - Posterior MI (V1-V2 indirect + Posterior leads V8-V9):
Indirect findings in V1-V2 (mirror image of posterior STEMI):
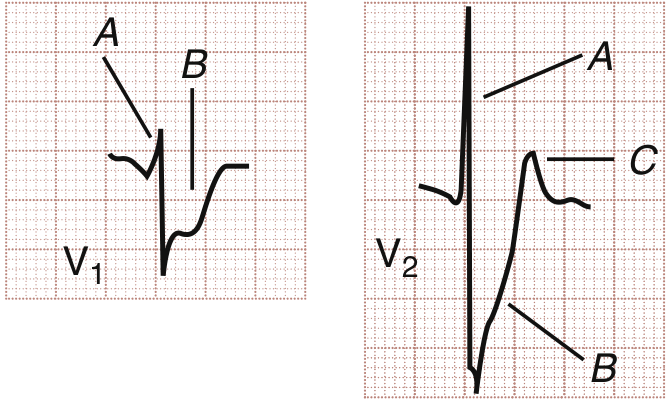
- Lead V1: A = tall R wave (mirror of posterior Q), B = ST depression
- Lead V2: A = tall R wave, B = ST depression, C = upright T wave
Direct posterior leads V8-V9 showing ST elevation:
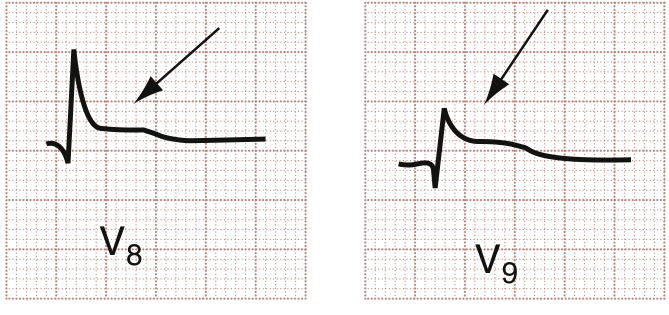 Arrows indicate subtle ST elevation - direct evidence of posterior wall infarction
Arrows indicate subtle ST elevation - direct evidence of posterior wall infarction
Source: Rosen's Emergency Medicine - Figs. 64.12 & 64.13
Treatment: Immediate percutaneous coronary intervention (PCI) - "door-to-balloon" time <90 minutes. If PCI unavailable, thrombolysis within 12 hours. Aspirin + P2Y12 inhibitor, heparin, statin.
3. Ventricular Fibrillation (VF)
What it is: Completely chaotic ventricular electrical activity with no coordinated contraction - no cardiac output. The most common cause of sudden cardiac death.
Causes: Ischemic heart disease (most common), electrolyte imbalances (hypokalemia, hypomagnesemia), drug toxicity, cardiomyopathy, Brugada syndrome.
Symptoms: Sudden cardiac arrest - loss of consciousness, no pulse.
ECG Features:
- Completely chaotic, irregular waveforms with no identifiable P waves, QRS complexes, or T waves
- Variable amplitude and frequency oscillations
- No organized rhythm whatsoever
- Coarse VF = higher amplitude (more likely to respond to defibrillation)
- Fine VF = low amplitude (longer duration, harder to convert)
ECG Pattern Reference:
From the physiology comparison chart above (panel d), the ECG shows chaotic irregular oscillations with total lack of normal electrical activity - the classic "bag of worms" appearance.
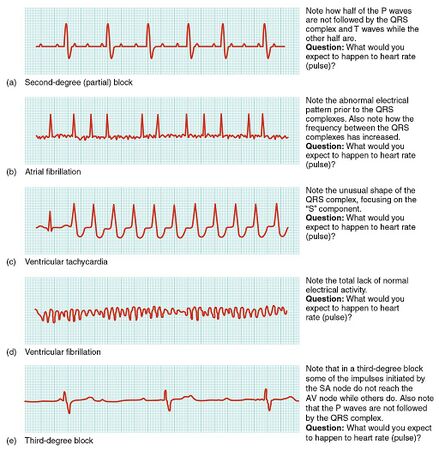
Panel (d) = Ventricular fibrillation: chaotic, irregular oscillations with no organized waveforms
Treatment: Immediate CPR + defibrillation (unsynchronized DC shock). ACLS protocol: adrenaline 1 mg IV, amiodarone 300 mg IV after 3rd shock. Treat reversible causes (4 H's and 4 T's).
4. Ventricular Tachycardia (VT)
What it is: A rapid, potentially life-threatening arrhythmia originating in the ventricles at rate >100 bpm (usually 150-250 bpm).
Causes: Coronary artery disease (most common in adults), cardiomyopathy, electrolyte abnormalities, drug toxicity, channelopathies (Long QT, Brugada).
Symptoms: Palpitations, dizziness, syncope, chest pain. Hemodynamic collapse if sustained.
ECG Features (Goldman-Cecil Medicine):
- Wide QRS complexes (>0.12 sec, usually >0.14 sec)
- Monomorphic VT: All QRS complexes have the same morphology
- Rate typically 150-250 bpm
- AV dissociation (P waves independent of QRS) - pathognomonic when seen
- Fusion beats and capture beats - highly specific for VT
- Concordance in precordial leads (all positive or all negative)
Panel (c) in the arrhythmia chart above shows the unusual wide, rapid QRS complexes of ventricular tachycardia with increased frequency.
Treatment: If pulseless - CPR + defibrillation. If with pulse - cardioversion (synchronized) if unstable; amiodarone or procainamide if stable. Long-term: ICD implantation, catheter ablation.
5. Second-Degree AV Block (Heart Block)
What it is: Intermittent failure of conduction from the atria to the ventricles. Two main types:
- Mobitz Type I (Wenckebach): Progressive PR prolongation until a P wave is blocked
- Mobitz Type II: Sudden non-conducted P waves without PR prolongation - more dangerous
Causes: Inferior MI (Mobitz I - usually reversible), anterior MI (Mobitz II - often requires pacing), myocarditis, drug toxicity (digoxin, beta-blockers), degenerative conduction disease.
ECG Features:
- Mobitz I: PR interval gets progressively longer until one P wave is not followed by QRS; then cycle repeats (group beating pattern)
- Mobitz II: Constant PR interval, then sudden dropped beat (P wave with no QRS); often with bundle branch block
Panel (a) in the physiology chart shows second-degree (partial) block - note how half of the P waves are not followed by QRS complexes.
Treatment: Mobitz I - usually monitor, treat underlying cause, atropine if symptomatic. Mobitz II - urgent pacing (temporary then permanent pacemaker).
6. Third-Degree (Complete) AV Block
What it is: Complete failure of conduction between atria and ventricles. The atria and ventricles beat completely independently, maintained by a slow escape rhythm.
Causes: Degenerative conduction disease (most common in elderly), inferior or anterior MI, myocarditis, Lyme disease, drug toxicity, congenital.
Symptoms: Bradycardia, syncope (Stokes-Adams attacks), heart failure, sudden death risk.
ECG Features (LITFL):
- Complete AV dissociation - P waves and QRS complexes have NO relationship
- P waves at atrial rate (usually 60-100 bpm)
- QRS complexes at escape rate (40-60 bpm if junctional; 20-40 bpm if ventricular)
- Ventricular escape rhythm - wide QRS if below His bundle
- Junctional escape rhythm - narrow QRS (faster, more stable)
- PP intervals regular; RR intervals regular - but completely independent of each other
Panel (e) in the physiology chart shows third-degree block - impulses from SA node do not reach AV node for some beats, P waves are not followed by QRS.
Treatment: Emergency transcutaneous pacing or temporary transvenous pacing, followed by permanent pacemaker implantation.
7. Atrial Flutter
What it is: A rapid, organized atrial arrhythmia caused by a single reentrant circuit in the right atrium, producing atrial rates of 250-350 bpm.
Causes: Heart failure, mitral/tricuspid valve disease, COPD, pulmonary embolism, hyperthyroidism, post-cardiac surgery.
Symptoms: Palpitations, dyspnea, fatigue; can degenerate into AF.
ECG Features (Guyton and Hall):
- Classic "sawtooth" flutter waves (F waves) at 250-350 bpm - best seen in leads II, III, aVF, V1
- Regular atrial activity (unlike AF)
- Fixed AV conduction ratio - usually 2:1 (ventricular rate ~150 bpm), 3:1, or 4:1
- QRS complexes are normal/narrow (unless aberrant conduction)
- No isoelectric baseline between flutter waves
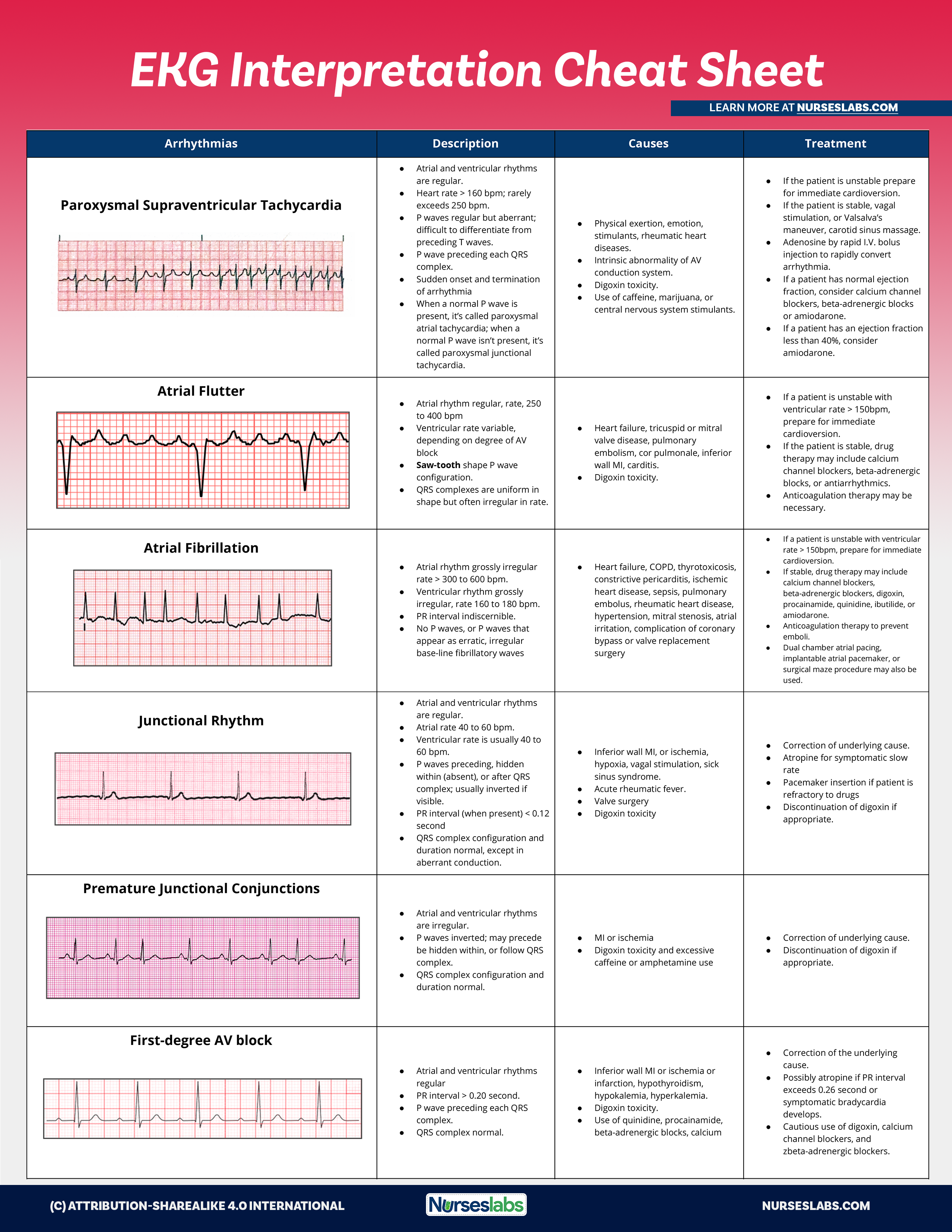
The EKG cheat sheet above shows atrial flutter with the characteristic sawtooth pattern and regular QRS response.
Treatment: Rate control with AV nodal blocking agents, cardioversion (electrical or chemical with ibutilide), radiofrequency ablation of the cavotricuspid isthmus (highly effective, ~95% cure rate).
8. Left Ventricular Hypertrophy (LVH)
What it is: Thickening of the left ventricular myocardium in response to chronic pressure or volume overload. A major risk factor for heart failure, arrhythmias, and sudden death.
Causes: Long-standing hypertension (most common), aortic stenosis, hypertrophic cardiomyopathy, aortic regurgitation.
Symptoms: Often asymptomatic until complications develop. Can cause dyspnea, chest pain, palpitations.
ECG Features:
- High-voltage QRS complexes:
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 >35 mm
- Cornell criteria: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- Left axis deviation
- ST depression and T wave inversion in lateral leads (V5-V6, I, aVL) - "strain pattern"
- Prolonged QRS duration (often 0.10-0.12 sec)
- Left atrial enlargement - broad, notched P waves in II ("P mitrale")
Treatment: Address underlying cause - aggressive blood pressure control (target <130/80 mmHg), treat aortic stenosis/regurgitation, ACE inhibitors/ARBs can promote LVH regression.
9. Wolff-Parkinson-White Syndrome (WPW)
What it is: Pre-excitation syndrome caused by an accessory pathway (Bundle of Kent) that bypasses the AV node, allowing direct electrical conduction from atria to ventricles. Predisposes to dangerous tachyarrhythmias.
Causes: Congenital. Can be associated with Ebstein's anomaly.
Symptoms: Palpitations, syncope, sudden cardiac death risk (especially if AF develops with rapid conduction down the accessory pathway).
ECG Features:
- Short PR interval (<0.12 sec) - accessory pathway bypasses AV node delay
- Delta wave - slurred, slow upstroke at the beginning of QRS (slow conduction through ventricular myocardium via accessory pathway)
- Widened QRS complex (>0.12 sec) due to delta wave
- Discordant ST-T changes (secondary to abnormal ventricular activation)
- During tachycardia: can be narrow complex (orthodromic AVRT) or wide complex (antidromic AVRT, or AF with rapid accessory pathway conduction)
Danger: AF in WPW can conduct at very rapid rates (>300 bpm) down the accessory pathway, potentially triggering VF and sudden death. Never use AV nodal blocking agents (digoxin, verapamil, adenosine) in AF with WPW.
Treatment: Radiofrequency catheter ablation of the accessory pathway (definitive, >95% success). Acute AVRT: adenosine (if narrow complex, no AF). Acute AF with WPW: procainamide or electrical cardioversion.
10. Long QT Syndrome
What it is: Prolongation of the QT interval representing delayed ventricular repolarization. Predisposes to a specific polymorphic VT called Torsades de Pointes (TdP), which can degenerate into VF and cause sudden death.
Causes:
- Congenital: Romano-Ward syndrome (autosomal dominant), Jervell and Lange-Nielsen syndrome (with deafness)
- Acquired (more common): Drugs (antiarrhythmics, antibiotics like azithromycin/fluoroquinolones, antipsychotics, antihistamines), hypokalemia, hypomagnesemia, hypothyroidism, bradycardia, myocarditis
ECG Features:
- Prolonged QT interval - corrected QT (QTc) using Bazett formula: QTc = QT / √RR
- Normal QTc: <440 ms (men), <460 ms (women)
- Borderline: 440-470 ms
- Prolonged: >470 ms (men), >480 ms (women)
- Very high risk: >500 ms
- T wave abnormalities - broad-based, notched, or biphasic T waves
- U waves may be prominent (especially in hypokalemia)
- Torsades de Pointes: Polymorphic VT with characteristic twisting of QRS axis around the isoelectric line ("twisting of the points")
Treatment: Remove offending drugs/correct electrolytes. Congenital LQTS: beta-blockers (especially nadolol), ICD in high-risk patients, left cardiac sympathetic denervation. Acquired TdP: IV magnesium sulfate 2g, increase heart rate (overdrive pacing or isoproterenol).
ECG Reference Charts
Comprehensive Arrhythmia Comparison:
The image below shows ECG strip comparisons of multiple arrhythmias side-by-side:
EKG Interpretation Quick Reference (Arrhythmias with ECG Strips):
Quick Summary Table
| # | Condition | Key ECG Finding | Rate | Rhythm |
|---|---|---|---|---|
| 1 | Atrial Fibrillation | No P waves, fibrillatory baseline | 100-180 bpm | Irregularly irregular |
| 2 | STEMI | ST elevation ≥1mm in 2+ leads | Variable | Regular |
| 3 | Ventricular Fibrillation | Chaotic oscillations, no organized waveforms | Undetectable | Chaotic |
| 4 | Ventricular Tachycardia | Wide QRS (>0.12s), AV dissociation | 150-250 bpm | Regular |
| 5 | 2nd-Degree AV Block | Dropped beats (Mobitz I: progressive PR; Mobitz II: sudden block) | Variable | Irregular |
| 6 | Complete Heart Block | P waves & QRS completely independent | Atria 60-100; Ventricles 20-60 | Two independent regular rhythms |
| 7 | Atrial Flutter | Sawtooth F waves 250-350 bpm, 2:1 AV block | ~150 bpm | Regular |
| 8 | LVH | Tall QRS voltage (S V1 + R V5 >35mm), lateral strain pattern | Normal | Normal sinus |
| 9 | WPW Syndrome | Short PR, delta wave, wide QRS | Normal (or tachycardia) | Variable |
| 10 | Long QT Syndrome | QTc >470 ms, abnormal T waves; TdP if arrhythmia | Normal baseline; TdP rapid | Normal baseline; TdP polymorphic |
Sources:
- Guyton and Hall Textbook of Medical Physiology, Fig. 13.20
- Rosen's Emergency Medicine, Figs. 64.12-64.13
- Goldman-Cecil Medicine, Chapter 53 (Ventricular Arrhythmias)
- Harrison's Principles of Internal Medicine 22E
- LITFL ECG Library (litfl.com)
- Nurseslabs EKG Interpretation Reference
This is a shared conversation. Sign in to Orris to start your own chat.