Calcaneal valgus
Reading File
search_medical_text
calcaneal valgus deformity etiology presentation diagnosis management
search_medical_image
calcaneal valgus foot deformity
GradeResponse
GradeResponse
The retrieval was limited, so I'll supplement with comprehensive clinical knowledge.
Calcaneal Valgus
Definition
Calcaneal valgus (also called hindfoot valgus) refers to lateral deviation of the calcaneal tuberosity relative to the long axis of the tibia, such that the heel tilts outward (everted). The calcaneal-tibial angle (measured on the coronal plane) normally ranges from 0–5° of valgus; values above this threshold are considered pathological.
Measurement
The plumb line test (posterior view) is a simple clinical method: a vertical reference line along the lower leg axis is compared to the bisection line of the calcaneal tuberosity. The angle between the two lines at the ankle joint quantifies the degree of valgus.
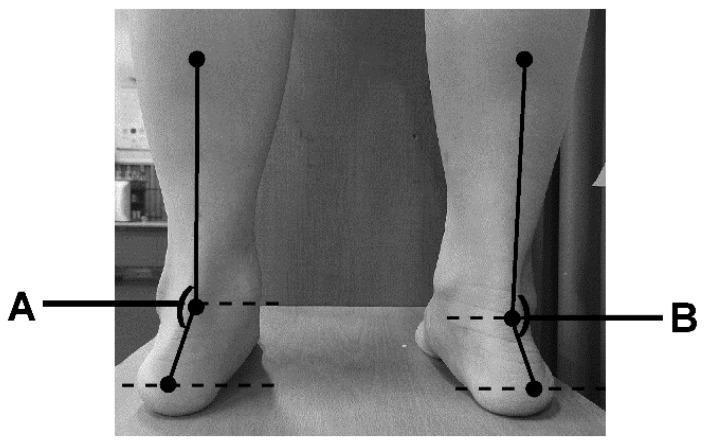
Posterior view demonstrating the plumb line technique for measuring calcaneal valgus angle. Angle A (left) and B (right) are formed between the lower leg axis and calcaneal bisection lines.
Etiology & Classification
| Category | Examples |
|---|---|
| Congenital | Calcaneovalgus foot (intrauterine positional), vertical talus, ligamentous laxity syndromes (Ehlers-Danlos, Down syndrome) |
| Neuromuscular | Cerebral palsy, spina bifida, Charcot-Marie-Tooth (peroneal type) |
| Acquired — structural | Posterior tibial tendon dysfunction (PTTD / adult-acquired flatfoot), calcaneal fracture malunion, ankle/subtalar OA |
| Acquired — inflammatory | Rheumatoid arthritis (most common cause of painful valgus deformity in adults) |
| Iatrogenic/traumatic | Over-lengthening of Achilles, subtalar coalition post-excision |
Pathomechanics
Hindfoot valgus does not occur in isolation — it is part of a kinematic chain:
- Calcaneus everts → subtalar joint pronates
- Talus adducts and plantarflexes (talar head medial descent)
- Midfoot collapses (navicular drops medially)
- Forefoot abducts ("too many toes" sign on posterior view)
- Tibia internally rotates → increased knee valgus stress
This chain is most evident in PTTD (Stage II and beyond) and RA-related valgus deformity.
Clinical Presentation
- Medial ankle/arch pain (PTTD); diffuse foot pain in RA
- Flattening of the medial longitudinal arch (pes planus)
- "Too many toes" sign — excessive lateral toes visible from behind
- Single-limb heel rise test failure — inability to invert the heel while rising on one foot (pathognomonic of PTTD)
- Shoe wear pattern: excessive medial heel and sole wear
- In severe/chronic cases: lateral impingement pain from fibula-calcaneal abutment
Diagnosis
Clinical
- Posterior tibial tendon palpation and strength testing
- Subtalar range of motion (rigid vs. flexible deformity)
- Coleman block test (to distinguish forefoot-driven from hindfoot-driven deformity)
Imaging
| Modality | Findings |
|---|---|
| Weight-bearing X-ray (AP & lateral foot) | Increased talo-first metatarsal angle (Meary's angle), reduced calcaneal pitch, talar uncovering, calcaneal valgus angle |
| MRI | PTT degeneration/tear, spring ligament tear, peritalar subluxation |
| CT | Coalitions, bony impingement, post-traumatic deformity assessment |
| Ultrasound | Dynamic PTT assessment, tendinopathy |
Calcaneal pitch (lateral view): normal 20–30°; reduced in valgus/flatfoot.
Talar uncoverage (AP view): >25% suggests significant deformity requiring surgical consideration.
Management
Non-Operative (flexible deformity, mild-moderate)
- Foot orthotics: medial heel wedge or UCBL (University of California Biomechanics Laboratory) orthosis to support the rearfoot — reduces pain and functional limitation (Harrison's, p. 10058)
- AFO (Ankle-Foot Orthosis): for neuromuscular cases or severe adult flatfoot
- Physical therapy: posterior tibial tendon strengthening, gastrocnemius stretching, intrinsic foot strengthening
- NSAIDs / corticosteroids: for inflammatory etiology (RA, tenosynovitis)
- Activity modification: avoid high-impact loading
Operative (rigid deformity, failed conservative care, Stage III–IV PTTD)
| Procedure | Indication |
|---|---|
| Medializing calcaneal osteotomy | Flexible hindfoot valgus (PTTD Stage II) |
| Lateral column lengthening (Evans) | Forefoot abduction correction |
| FDL-to-PTT transfer | PTT incompetence |
| Subtalar arthrodesis | Rigid deformity, subtalar arthritis |
| Triple arthrodesis (subtalar + talonavicular + calcaneocuboid) | Severe rigid deformity, Stage III–IV PTTD, RA |
| Total ankle replacement / ankle fusion | Pantalar arthritis |
Special Populations
Newborn / Infant (Calcaneovalgus Foot)
- Very common positional deformity at birth (foot dorsiflexed and everted against the shin)
- Almost always self-resolving within 3–6 months with passive stretching
- Must be distinguished from vertical talus (rigid, "rocker-bottom" foot) — critical differentiator
Rheumatoid Arthritis
- Valgus deformity at the hindfoot is a hallmark of advanced RA foot involvement
- Orthotics reduce pain and disability; surgery (triple arthrodesis) reserved for refractory cases
Cerebral Palsy
- Spastic or hypotonic patterns both produce valgus
- Management coordinated with neuromotor considerations; botulinum toxin injections may reduce spastic drive before bony correction
Complications (if untreated)
- Progressive flatfoot deformity
- Lateral ankle impingement (subfibular)
- Peroneal tendon pathology
- Medial ligament incompetence
- Degenerative arthritis (subtalar, talonavicular, ankle)
- Knee and hip alignment changes secondary to limb malalignment
Summary
Calcaneal valgus is a common hindfoot malalignment with a spectrum from benign positional deformity in neonates to debilitating structural pathology in adults. Flexible deformity is managed conservatively with orthotics and PT; rigid or progressive deformity requires surgical reconstruction tailored to the underlying cause and stage.
This is a shared conversation. Sign in to Orris to start your own chat.