Eye manifestation in syphillis
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
syphilis ocular manifestations
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
syphilis eye uveitis retinitis interstitial keratitis
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive data from multiple authoritative textbooks. Here is a detailed synthesis:
Ocular Manifestations of Syphilis
Ocular syphilis is considered a subset of neurosyphilis and should be managed as such per CDC guidelines. It can occur at any stage of infection and may involve virtually any structure of the eye. Bilateral involvement is seen in 50–70% of cases. Clinicians should always ask about eye symptoms when evaluating any patient with syphilis.
By Stage of Infection
Primary Syphilis
- Eyelid/conjunctival chancre — painless ulcerated lesion
- Madarosis — loss of eyelashes or eyebrows
- Regional lymphadenopathy near periorbital area
Secondary Syphilis (Most common stage for ocular involvement)
- Uveitis — most frequent manifestation; posterior and panuveitis more common than anterior; anterior uveitis occurs in 5–10% of secondary syphilis cases
- Patchy iris hyperemia with fleshy pink nodules near the iris sphincter is a classic presentation
- Optic neuritis / papillitis
- Chorioretinitis and retinitis
- Acute posterior placoid chorioretinitis (APPC) — multifocal white placoid lesions in the posterior pole; strongly suggestive of syphilis
- Punctate inner retinitis — superficial punctate creamy-white lesions; strongly suggestive of syphilis
- Serous retinal detachment
- Retinal vasculitis
- Interstitial keratitis
- Conjunctivitis, episcleritis, scleritis, dacryoadenitis, dacryocystitis
- Pupillary abnormalities
"The diagnosis of ocular syphilis is often considered only after patients fail to respond to topical steroid therapy" — Harrison's, 22nd Ed.
Tertiary / Late Syphilis (Neurosyphilis)
- Argyll Robertson pupil — the classic finding; small, irregular pupil that accommodates but does not react to light ("prostitute's pupil"); seen in ~90% of tabes dorsalis
- Optic atrophy — seen in ~20% of tabes dorsalis
- Cranial nerve palsies — III, IV, VI (due to syphilitic basilar meningitis)
- Chronic anterior uveitis
- Old chorioretinitis scar
- Bitemporal hemianopia — from chiasmal syndrome due to gummas or basilar meningitis
- Retinal detachment, cataracts, glaucoma (advanced)
- Stroke syndromes involving optic/oculomotor nerves
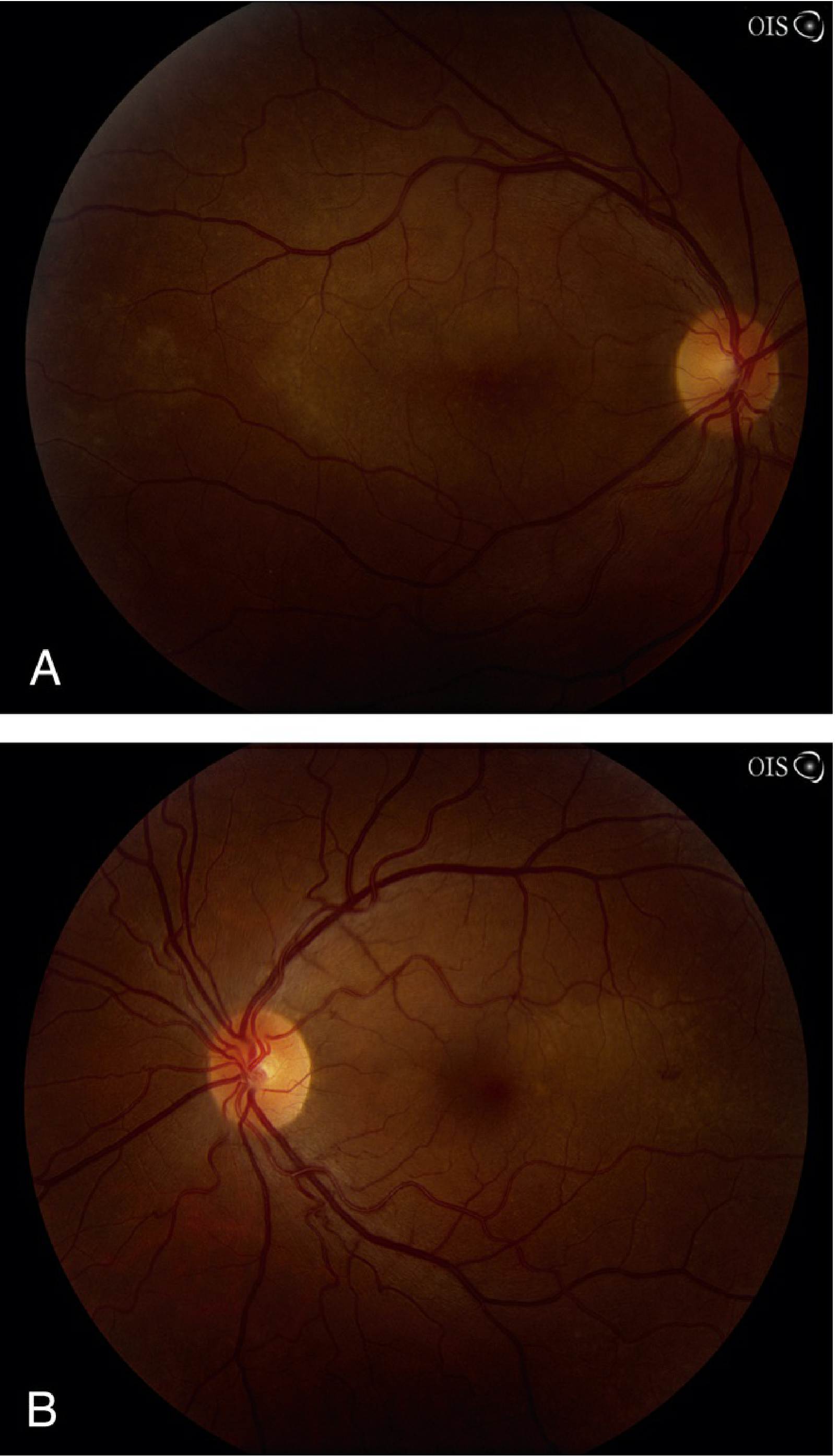
Fundus Photographs — Ocular Syphilis
Placoid Retinopathy in Secondary Syphilis
(Right eye [A] and left eye [B] — from Wills Eye Manual)
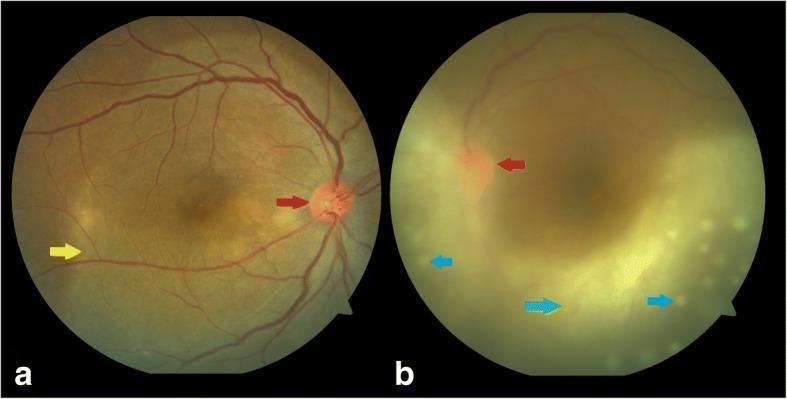
Syphilitic Posterior Uveitis with Disc Edema and Retinitis (HIV co-infected patient)
(Right eye [a] shows disc hyperemia [red arrow] and posterior placoid retinochoroiditis [yellow arrow]; left eye [b] shows vitritis [green arrow] and punctate lesions [blue arrows])
Congenital Syphilis — Ocular Findings
| Finding | Notes |
|---|---|
| Interstitial keratitis | Hallmark; bilateral; may be active (early) or old/quiet (late) |
| Salt-and-pepper chorioretinitis | Classic fundus appearance |
| Chronic anterior uveitis | |
| Secondary cataracts | |
| Optic atrophy | Late manifestation |
| Choroiditis |
Hutchinson's Triad (Late Congenital Syphilis)
- Interstitial keratitis
- Hutchinson teeth — peg-shaped, widely spaced, notched incisors
- Eighth-nerve (sensorineural) deafness
Summary Table: Ocular Structures Affected
| Structure | Manifestations |
|---|---|
| Eyelids | Chancre, condylomata lata, madarosis |
| Conjunctiva | Conjunctivitis, chancre, gumma, scleroconjunctivitis |
| Cornea | Interstitial keratitis |
| Sclera/Episclera | Episcleritis, scleritis |
| Iris/Uveal tract | Anterior, posterior, panuveitis; iris nodules |
| Retina | Retinitis, vasculitis, APPC, punctate inner retinitis, serous detachment, salt-and-pepper |
| Optic nerve | Papillitis, retrobulbar neuritis, optic atrophy, gumma |
| Pupils | Argyll Robertson pupil |
| Cranial nerves | CN III, IV, VI palsies |
| Visual pathways | Bitemporal hemianopia (chiasmal) |
| Lens | Secondary cataract (congenital) |
Key Clinical Points
- "The great imitator" — ocular syphilis can mimic almost any uveitic or retinal condition
- All patients with confirmed syphilitic uveitis should have lumbar puncture (VDRL, FTA, protein, cell count) as the condition is managed as neurosyphilis
- In 70% of ocular syphilis cases, concomitant CSF abnormalities are found
- HIV co-infection increases risk of ocular and neurologic complications; HIV testing is mandatory in all syphilis patients
- Men who have sex with men (MSM) are at highest risk
Diagnosis
- Reverse algorithm: Treponemal test first (FTA-ABS, EIA, MHA-TP) → if reactive, confirm with nontreponemal test (RPR/VDRL) for disease activity and treatment response
- CSF VDRL: highly specific for neurosyphilis (insensitive but diagnostic when positive)
Treatment
- Aqueous penicillin G IV — treated as neurosyphilis regardless of CSF findings
- RPR/VDRL titers should decrease fourfold within 6–12 months post-treatment
- For congenital syphilis: IV penicillin G managed by pediatrician/ID specialist
Sources: Wills Eye Manual, 7th Ed. • Harrison's Principles of Internal Medicine, 22nd Ed. (2025) • Goldman-Cecil Medicine • Fitzpatrick's Dermatology, 9th Ed. • Robbins Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.