Management of Acute diarrhoea
Reading File
Finding Sources
Searching PubMed
"acute diarrhea" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed answer.
Management of Acute Diarrhoea
Acute diarrhea is defined as diarrhea of fewer than 14 days' duration. The majority of cases are infectious in origin (viral > bacterial > parasitic) and self-limiting. Management follows a structured approach based on severity, clinical appearance, and likely etiology.
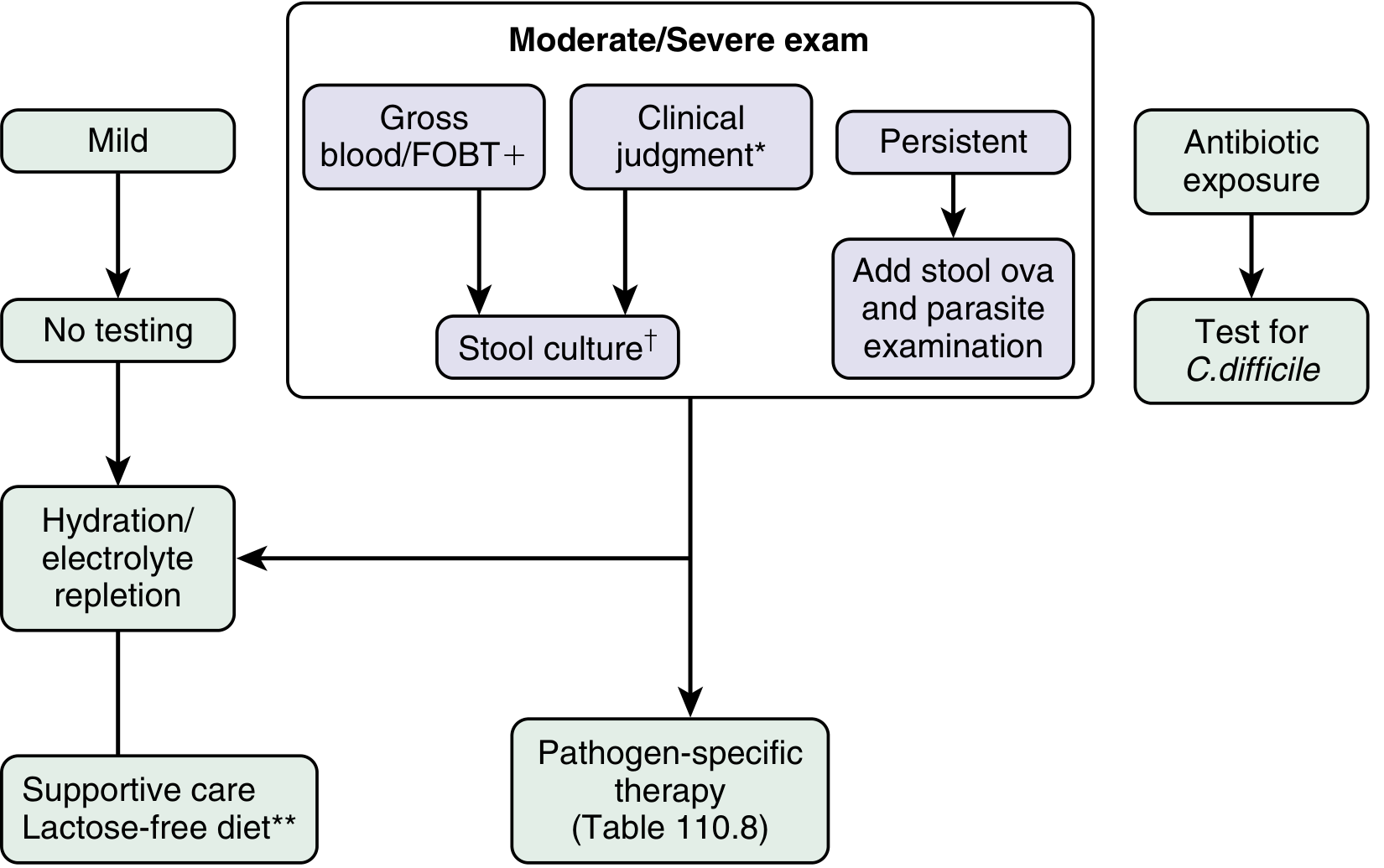
Algorithm Overview
The following diagnostic and treatment algorithm from Sleisenger & Fordtran's Gastrointestinal and Liver Disease guides clinical decision-making:
Step 1: Severity Assessment
| Appearance of Patient | Management |
|---|---|
| Nontoxic / Mild | Symptomatic therapy + rehydration. No testing required. |
| Toxic / Severe | Fluid and electrolyte repletion + CBC + serum electrolytes, BUN, creatinine + stool tests (culture, O&P, C. difficile, multiplex PCR) ± sigmoidoscopy/colonoscopy |
Table 16.3 - Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Red flags warranting urgent evaluation:
- Blood in stool (indicates invasive organism)
- High fever (>38.5°C)
- Severe dehydration (dry mouth, decreased urine output, weakness)
- Duration > 7 days (consider parasitic causes, C. difficile)
- Nocturnal diarrhea (organic cause, not functional)
- Recent antibiotic use (screen for C. difficile)
Step 2: Rehydration (CORNERSTONE of Management)
Rehydration is the primary and most important treatment for all diarrheal illnesses.
Oral Rehydration Solution (ORS)
The WHO reduced-osmolarity ORS (recommended since 2002) is better tolerated and more effective than the original formula. Composition per liter of water:
| Component | Amount |
|---|---|
| Sodium chloride | 2.6 g |
| Trisodium citrate | 2.9 g |
| Potassium chloride | 1.5 g |
| Glucose (or 27 g sucrose) | 13.5 g |
- ORS works by exploiting the intact glucose-Na+ cotransport mechanism in the small intestine - this remains functional even in the presence of cholera toxin.
- Give ORS ad libitum with free water. Rice-based ORS may be even more effective than glucose-based solutions.
- Breast-feeding should continue in infants with diarrhea.
- Zinc supplementation is recommended for children >6 months in developing areas (reduces diarrhea volume).
When IV Fluids Are Needed
Patients who are severely dehydrated, unable to drink, or vomiting should receive IV Ringer's lactate, in addition to ORS when oral intake becomes possible.
Harrison's Principles of Internal Medicine 22E, p. 1124; Goldman-Cecil Medicine
Step 3: Diet
- Avoid milk and dairy products (risk of transient secondary lactase deficiency).
- Avoid caffeine (coffee, tea, cola) and alcohol - these can worsen cramps and diarrhea.
- Recommended foods: soups, saltine crackers, bananas, mashed potatoes, rice.
- Bowel rest is NOT the goal - eating judiciously is preferred, especially in children where early refeeding is important.
Sleisenger & Fordtran's GI and Liver Disease
Step 4: Symptomatic (Non-Antimicrobial) Therapy
Antimotility Agents
- Loperamide: 2-4 mg as a single dose, then 2 mg after each loose stool; maximum 16 mg/day in adults.
- Reduces frequency of diarrheal stools.
- Contraindicated when fever or bloody diarrhea is present - risk of toxic megacolon or hemolytic-uremic syndrome (HUS).
- Do not use if Shigella or other invasive organisms are suspected.
Bismuth Subsalicylate
- 262-524 mg up to four times a day.
- Useful in traveler's diarrhea and vomiting-predominant illness.
- Use with caution to avoid salicylate toxicity.
Racecadotril (Enkephalinase Inhibitor)
- Available in Europe (not currently in North America).
- Also reduces diarrheal symptoms without the risks of antimotility agents.
Goldman-Cecil Medicine, p. 3123; Harrison's
Step 5: Antimicrobial Therapy
General Principles
Only a limited subset of acute infectious diarrhea benefits from antibiotics. Even when indicated, clinical impact is modest and mostly effective only when started within 2 days of symptom onset. Rising antimicrobial resistance is an important concern.
Clear indications for antimicrobial treatment in the immunocompetent host:
- Clostridioides difficile infection
- Vibrio cholerae
- Traveler's diarrhea (moderate-severe)
- Dysentery (bloody stools + fever) - empiric treatment pending culture
Situations where antibiotics should be AVOIDED:
- Enterohemorrhagic E. coli (EHEC/STEC) / suspected E. coli O157:H7 - antibiotics induce Shiga toxin-producing bacteriophages, increasing HUS risk by up to 20-fold.
- Uncomplicated Salmonella gastroenteritis in healthy adults (antibiotics prolong fecal carriage).
Empiric Antibiotic Regimens
Adults:
- Fluoroquinolone: Ciprofloxacin 750 mg single dose or 500 mg twice daily x 3 days; or levofloxacin 500 mg once daily x 3 days.
- Azithromycin: 1000 mg single dose or 500 mg once daily x 3 days. (Preferred over fluoroquinolones for suspected fluoroquinolone-resistant Campylobacter - common after travel to Southeast Asia, India, Nepal; also safer in pregnancy and children.)
- Rifaximin: 200 mg three times daily or 400 mg twice daily x 3 days. (Non-absorbable; useful for non-invasive traveler's diarrhea.)
Children:
- Azithromycin: 10 mg/kg on day 1, then 5 mg/kg on days 2-3 if diarrhea persists.
- Fluoroquinolones generally not recommended in children or pregnant women.
Treatment duration: Typically 3-5 days; antibiotic therapy for 3-7 days for shigellosis.
Important safety note regarding fluoroquinolones: The FDA now advises against fluoroquinolones for uncomplicated infections given the spectrum of serious adverse effects - tendinitis, tendon rupture, peripheral neuropathy, CNS toxicity, QT prolongation, and risk of aortic dissection/aneurysm.
Sleisenger & Fordtran's, Harrison's 22E; Goldman-Cecil Medicine
Step 6: Pathogen-Specific Considerations
| Pathogen | Notes |
|---|---|
| Norovirus / Rotavirus | Supportive care only; self-limiting |
| ETEC (Traveler's diarrhea) | Rehydration + bismuth/loperamide; antibiotic only if moderate-severe |
| Campylobacter | Azithromycin preferred (high fluoroquinolone resistance in Asia) |
| Shigella | Fluoroquinolone or azithromycin x 3-7 days |
| Salmonella (non-typhoidal) | Supportive only in healthy adults; antibiotics for infants, >50 years, immunocompromised, prosthetic devices |
| EHEC / E. coli O157:H7 | No antibiotics - risk of HUS |
| C. difficile | Vancomycin (oral) or fidaxomicin first-line; see AGA 2026 guidelines |
| Cholera | ORS (cornerstone) + azithromycin or doxycycline |
| Giardia / Cryptosporidium | Metronidazole (Giardia); nitazoxanide (both) |
Step 7: Investigation - When to Test
| Indication | Investigation |
|---|---|
| Mild, community-acquired | No stool testing needed |
| Moderate-severe / toxic-appearing | Stool culture, fecal WBC/lactoferrin, multiplex PCR panel |
| Blood in stool / FOBT positive | Stool culture including STEC/Shiga toxin assay |
| Diarrhea lasting >7 days | Add stool ova and parasite examination |
| Recent antibiotic exposure | Test for C. difficile (toxin B PCR or EIA) |
| Nosocomial diarrhea | Focus on C. difficile first |
| HIV/immunocompromised | Colonoscopy preferred (pathology in right colon) |
| CBC | Leukocytosis suggests bacterial invasion; lymphocytosis suggests viral cause |
Multiplex PCR stool panels are increasingly replacing conventional culture as they are faster, more sensitive, and detect viral, bacterial, and parasitic pathogens simultaneously. However, the CDC recommends culture follow-up when nucleic acid amplification tests detect bacterial pathogens, to allow susceptibility testing and public health surveillance.
Sleisenger & Fordtran's, Harrison's 22E
Special Populations
- Infants (<2 years): ORS/Pedialyte; continue breast-feeding; seek medical attention for moderate dehydration, fever >24h, bloody stools, or diarrhea >few days.
- Children: Zinc supplementation in developing countries; azithromycin if antibiotics needed; no fluoroquinolones.
- Pregnant women: Azithromycin preferred; avoid fluoroquinolones.
- Immunocompromised: Lower threshold for testing and treatment; colonoscopy may be needed.
- Hospitalized patients: C. difficile is the priority pathogen; routine bacterial culture is low yield.
Recent Evidence (PubMed, 2025-2026)
- A 2025 meta-analysis (PMID: 40739406) confirmed probiotics reduce duration and severity of acute gastroenteritis in children - particularly Lactobacillus rhamnosus GG and Saccharomyces boulardii, though effect sizes are modest.
- 2024 Chinese pediatric guidelines (PMID: 40437180) reinforce ORS and zinc as first-line for children with acute infectious diarrhea.
- A 2026 AGA Clinical Practice Update (PMID: 42383946) provides updated guidance on C. difficile management in adults, emphasizing fidaxomicin and fecal microbiota transplant (FMT) for recurrent disease.
Summary in brief: Rehydrate first (ORS is the cornerstone), modify diet (BRAT-type foods, no dairy/caffeine/alcohol), use loperamide or bismuth for symptomatic relief in non-bloody/non-febrile illness, withhold antibiotics unless clearly indicated, and reserve targeted antimicrobials (azithromycin preferred over fluoroquinolones) for dysentery, traveler's diarrhea, cholera, C. difficile, and severely ill patients.
This is a shared conversation. Sign in to Orris to start your own chat.