Icd patient in respiratory department
Reading File
Asking for Preferences
Finding Sources
Searching the Web
ICD implantable cardioverter defibrillator patient respiratory department management considerations
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Intercoastal drainage
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from two major textbooks. Here is a complete, structured answer on Intercostal Drainage (ICD):
Intercostal Drainage (ICD) / Chest Tube Thoracostomy
An intercostal tube connected to an underwater seal is central to the management of chest disease, though pleural and drain management can be troublesome even in experienced hands.
Indications
- Pneumothorax - especially tension, large spontaneous, or failed aspiration
- Haemothorax
- Empyema / complicated parapneumonic effusion
- Large pleural effusion causing respiratory compromise
- Chylothorax
- Post-operatively following thoracic surgery
Surgical indications for drainage in pneumothorax include:
- Second ipsilateral pneumothorax
- First contralateral pneumothorax
- Bilateral spontaneous pneumothorax
- Pneumothorax failing to settle despite drainage
- Pregnancy, or professions at risk (pilots, divers)
Equipment Required
- Sterile drapes, gown, gloves, mask, goggles
- 10-20 mL syringe + needles for local anaesthetic (1-2% lidocaine)
- Antiseptic solution
- Scalpel (No. 10 blade)
- Large Kelly clamps
- Chest tubes - 12-42 Fr (smaller for pneumothorax; minimum 36 Fr for haemothorax/empyema)
- Paediatric: 14, 16, 20, or 24 Fr
- No. 0 or 1-0 silk suture, needle holder, forceps
- Petroleum gauze (occlusive dressing)
- Drainage apparatus with sterile water for underwater seal
Site of Insertion - "Triangle of Safety"
The safest insertion site is the "triangle of safety":
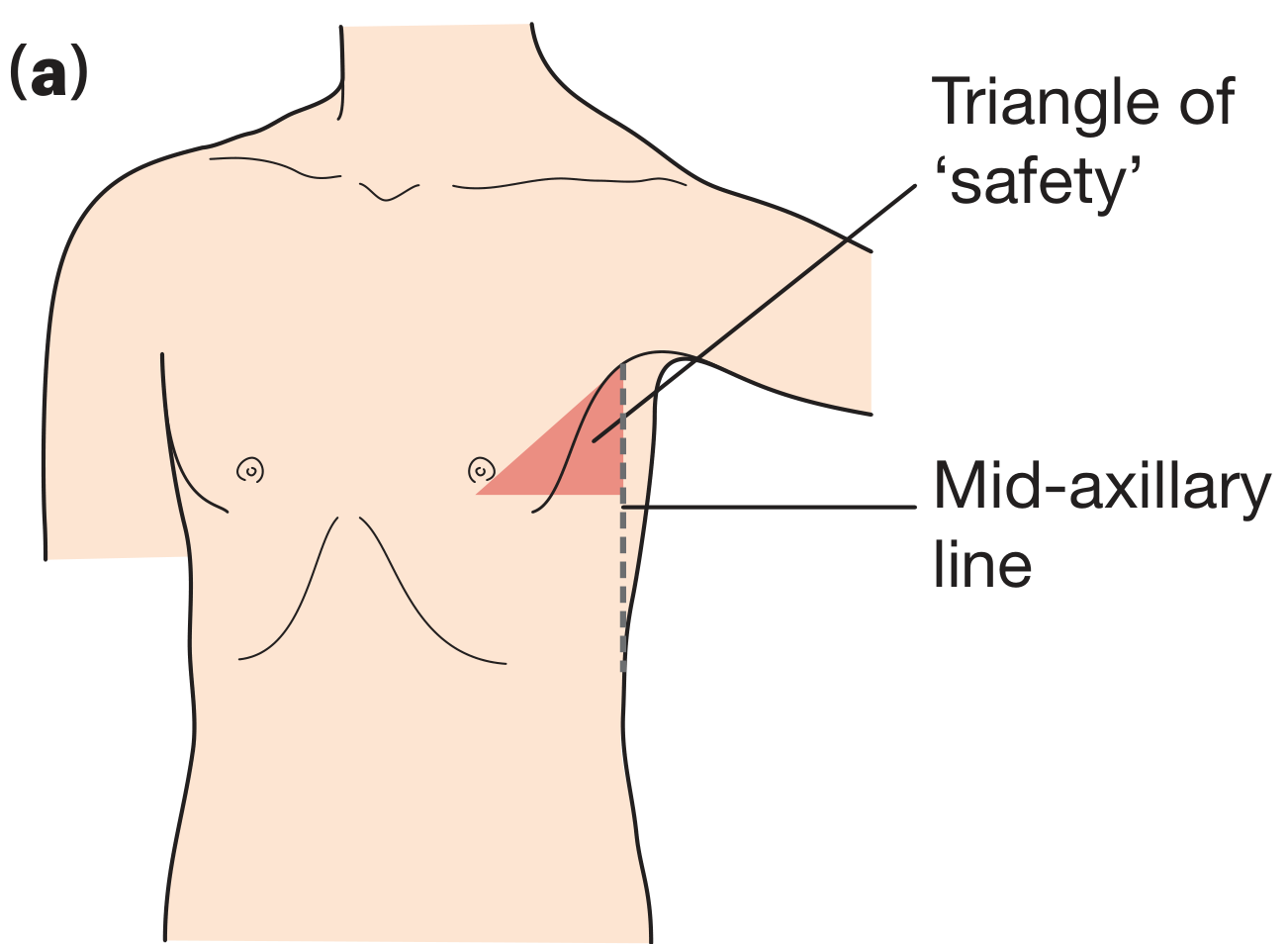
- Anterior to the mid-axillary line
- Above the level of the nipple
- Below and lateral to the pectoralis major muscle
This typically corresponds to the 4th or 5th intercostal space. The second intercostal space, mid-clavicular line is used for needle aspiration only.
Insertion Technique (Step by Step)
-
Meticulous sterility throughout
-
Local anaesthesia - infiltrate generously, including down to the pleura (this is the most painful step)
-
Make a transverse skin incision 3-5 cm long, lateral to pectoralis major and breast tissue
-
Blunt dissection with Kelly clamps through muscle layers (serratus anterior + intercostals)
-
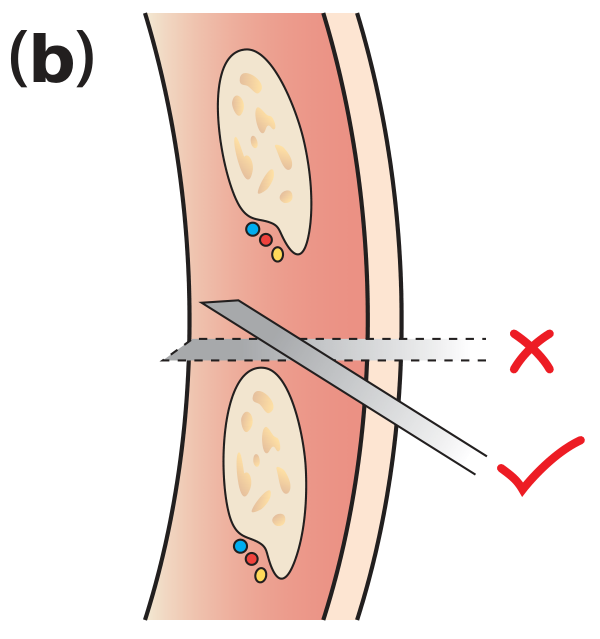
Always pass over the upper border of the rib - the neurovascular bundle (intercostal vessels and nerve) runs beneath each rib
-
Penetrate the parietal pleura with firm forward pressure - a palpable "pop" and rush of air/fluid confirms entry
-
Digital examination - sweep 360 degrees to verify correct space, feel for adhesions, ensure no solid organ penetration
-
Insert the tube over/beside the guiding finger:
- For pneumothorax or haemothorax - direct towards the apex
- For pleural effusion or empyema - direct towards the base
-
Ensure all drainage holes are within the pleural space
-
Secure with stay suture; insert a vertical mattress suture for later wound closure (omit for empyema if pleura is adherent, so the tract stays open)
-
Apply occlusive dressing (petroleum-impregnated gauze at skin)
-
Chest X-ray to confirm position - the gap in the radiopaque line must be within the pleural cavity
Underwater Seal Drainage System
The system has two essential components:
- A one-way valve (prevents air re-entry)
- A suction mechanism to increase drainage rate
How it works:
- The fluid level in the drainage tube fluctuates with respiration when functioning correctly (swings in with inspiration, out with expiration)
- The collection bottle must remain below chest level at all times
- Bubbling in the air-leak chamber indicates an air leak - check connections and tube position first; persistent bubbling = ongoing lung air leak
- Absence of fluctuation = tube blocked or lung fully expanded
Suction:
- Use suction initially for pneumothorax and haemothorax
- Replace with water seal once drainage is satisfactory and no air leak persists
- Wall suction at -80 mmHg is standard; suction amount depends on depth of water in chamber, not wall dial setting
- Vigorous bubbling does NOT equal more suction
Important Management Rules
| Rule | Rationale |
|---|---|
| Never clamp a bubbling drain | Risk of tension pneumothorax |
| Never clamp for transport - use Heimlich valve or water seal | Clamp may be forgotten |
| Do NOT apply suction routinely from the outset | Inserting the drain is the life-saving step, not the suction |
| Collection bottle always below chest level | Prevents siphoning back into pleural space |
| Remove drain when it no longer has a function | Reduces infection risk |
| Avoid clamping as a trial before removal | Risk of tension pneumothorax |
Drain Removal
Criteria for removal:
- Lung fully re-expanded on CXR
- No air leak (no bubbling)
- Fluid drainage < 100-200 mL/day (for effusions)
Remove during Valsalva or end-expiration (reduces risk of air entry). Close wound immediately with the pre-placed mattress suture.
Surgical intervention is indicated if an air leak persists for >72 hours or the lung fails to re-expand.
Complications
| Complication | Comment |
|---|---|
| Haemorrhage - intercostal vessel injury | Avoided by passing over upper rib border |
| Organ puncture (lung, liver, spleen, heart) | Digital check before tube insertion |
| Subcutaneous emphysema | Tube not fully in pleural space |
| Drain blockage | Strip tube; replace if needed |
| Empyema/infection | Higher with larger-bore tubes and repeated procedures |
| Re-expansion pulmonary oedema | Drain large effusions gradually |
| Tube dislodgement | Secure well; occlusive dressing |
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1001-1002; Roberts and Hedges' Clinical Procedures in Emergency Medicine, pp. 274-280
History of this par
History of this patient
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive material. Here is a complete structured history for a respiratory patient requiring intercostal drainage (ICD):
History Taking - Respiratory Patient for Intercostal Drainage
A thorough history should cover the following domains:
1. Presenting Complaint (PC)
The main symptoms that bring a patient requiring ICD to attention are typically:
- Chest pain - onset, site, character, radiation, severity (1-10), timing, aggravating/relieving factors
- Breathlessness (Dyspnoea) - onset (sudden vs gradual), at rest or on exertion, quantify (how many stairs/meters before stopping)
- Cough - dry or productive, duration
- Fever / rigors - suggests infection/empyema
- Trauma - history of chest injury (haemothorax)
2. History of Presenting Complaint (HPC)
Ask specifically about features pointing to the likely cause of the pleural pathology:
For Pneumothorax:
- Sudden onset sharp pleuritic chest pain + breathlessness
- Tall, thin young male? (primary spontaneous)
- Previous pneumothorax on same or opposite side?
- Underlying lung disease (COPD, asthma, cystic fibrosis, Marfan's)?
- Recent procedure or trauma (secondary/iatrogenic)?
For Pleural Effusion / Empyema:
- Recent respiratory infection, cough with purulent sputum
- Gradual increasing breathlessness
- Night sweats, weight loss, fever (TB, malignancy, empyema)
- Haemoptysis - raises concern for malignancy or TB
For Haemothorax:
- History of chest trauma, recent surgery, or coagulopathy
- Anticoagulant use
Symptom Progression:
- How rapidly did symptoms develop?
- Acute (minutes-hours) = pneumothorax, tension pneumothorax
- Subacute/chronic (days-weeks) = effusion, empyema
3. Past Medical History (PMH)
- Respiratory disease: COPD, asthma, TB, previous pneumothorax, lung cancer, cystic fibrosis, ILD
- Cardiac disease: heart failure (transudative effusion), pericarditis
- Connective tissue disease: SLE, rheumatoid arthritis, scleroderma (associated pleural and ILD)
- Malignancy (primary lung or metastatic - cause of effusion)
- Renal / liver disease (hypoalbuminaemia - transudative effusion)
- HIV/immunocompromise (opportunistic infections)
- Previous thoracic surgery or procedures
- History of DVT/PE (pleuritic pain, pleural effusion)
4. Drug History (DH)
Many drugs can cause pulmonary/pleural pathology:
| Drug Class | Examples |
|---|---|
| Antiarrhythmics | Amiodarone |
| Antibiotics | Nitrofurantoin, Minocycline |
| Anti-inflammatory | Methotrexate, NSAIDs, Gold salts |
| Chemotherapy | Bleomycin, Cyclophosphamide, Gemcitabine |
| Immunotherapy | Nivolumab, Ipilimumab |
| Anticoagulants | Warfarin, NOACs (risk of haemothorax) |
Also note: drugs of abuse (cocaine, heroin, talc)
- Ask about allergies (especially to local anaesthetics - lignocaine used for ICD)
5. Occupational & Environmental History
This is essential for respiratory patients:
- Asbestos exposure - electricians, plumbers, ship builders, construction workers (pleural plaques, mesothelioma - causes effusion)
- Silica - miners, stone cutters, sand blasters
- Hard metals/Beryllium - metal workers, electronics, nuclear industry
- Organic dusts - farmers, bird keepers (hypersensitivity pneumonitis)
- Current occupation - relevant for return to work planning post-ICD
6. Social History (SH)
- Smoking: pack-year history (COPD, lung cancer, respiratory bronchiolitis)
- Alcohol: liver cirrhosis → transudative pleural effusion
- Recreational drugs - IV drug use (septic emboli, empyema)
- Travel history - TB, hydatid cyst (Echinococcus), parasitic causes
- Pet ownership - bird/pigeon fancier (hypersensitivity pneumonitis)
- Living conditions - overcrowding (TB risk)
- Functional status - baseline exercise tolerance before this illness
- Occupation / hobbies (overlaps with occupational history)
7. Family History (FH)
- TB contacts
- Lung cancer
- Familial ILD (2-20% of idiopathic interstitial pneumonias are familial)
- Connective tissue disease
- Genetic conditions: Marfan's syndrome (tall, thin build - pneumothorax risk), cystic fibrosis
8. Systems Review
| System | Key Questions |
|---|---|
| Respiratory | Wheeze, stridor, sputum colour/amount, haemoptysis |
| Cardiovascular | Ankle oedema, orthopnoea, palpitations, syncope |
| GI | Dysphagia, reflux/aspiration (cause of ILD), weight loss |
| MSK | Joint swelling, morning stiffness, Raynaud's (connective tissue disease) |
| Skin | Rash, skin thickening, telangiectasia (scleroderma, SLE, dermatomyositis) |
| Eyes | Dry eyes (Sjögren), uveitis (sarcoidosis, SLE) |
| Neuro | Weakness (neuromuscular causing aspiration) |
| Constitutional | Fever, night sweats, weight loss (TB, lymphoma, malignancy) |
Summary: Key "Red Flags" Requiring Urgent ICD
| Feature | Likely Cause |
|---|---|
| Sudden severe breathlessness + tracheal deviation + hypotension | Tension pneumothorax - emergency ICD |
| Chest trauma + reduced air entry + haemodynamic compromise | Haemothorax |
| Fever + purulent pleural fluid + sepsis | Empyema |
| Rapidly accumulating effusion + weight loss + haemoptysis | Malignant effusion |
Sources: Fishman's Pulmonary Diseases and Disorders, 2-Volume Set; Bailey and Love's Short Practice of Surgery, 28th Ed.; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.