Myopectineal orifice of fruchaud
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
I have comprehensive information from three major surgery textbooks. Here is a detailed answer:
Myopectineal Orifice of Fruchaud
Definition and Historical Background
The myopectineal orifice (MPO) is the medial aspect of the superior gap between the pelvis and the thigh - a large, anatomically weak oval opening in the lower abdominal wall. In 1956, the French anatomist and surgeon Henri René Fruchaud first described this concept, proposing that weakening of the MPO is the fundamental cause of all hernias in the inguinal region. This concept became the foundation for modern adult groin hernia repair.
- Sabiston Textbook of Surgery, p. 1681
- Schwartz's Principles of Surgery (11th ed.), p. 1630
Boundaries of the MPO
The MPO is bounded by:
| Border | Structure |
|---|---|
| Superior | Arch of the internal oblique and transversus abdominis muscles |
| Medial | Lateral edge of the rectus abdominis muscle |
| Inferior / Posterior | Pectineal line of the pubis (Cooper's ligament / pectineal ligament) |
| Lateral | Iliopsoas muscle |
The inguinal ligament (Poupart's ligament) divides the MPO horizontally into two zones:
- Above the inguinal ligament - the inguinal region (direct and indirect inguinal hernias pass here)
- Below the inguinal ligament - the femoral region (femoral hernias pass here)
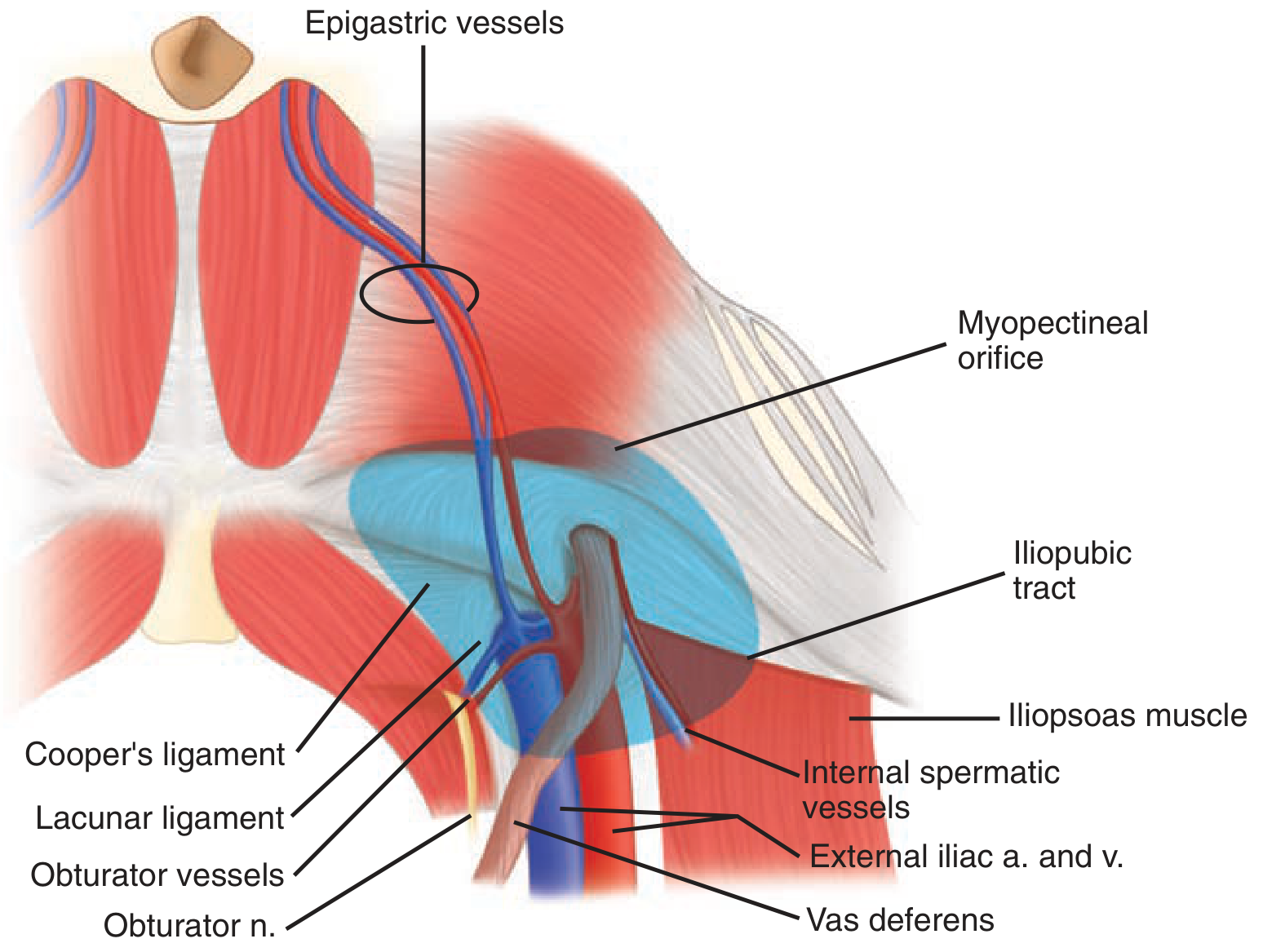
Posterior view of the myopectineal orifice of Fruchaud (from Schwartz's Principles of Surgery)
Why All Groin Hernias Pass Through the MPO
Every type of groin hernia - direct inguinal, indirect inguinal, and femoral - protrudes through some part of the MPO:
- Indirect inguinal hernia - passes lateral to the inferior epigastric vessels through the deep inguinal ring (upper lateral MPO)
- Direct inguinal hernia - passes medial to the inferior epigastric vessels within Hesselbach's triangle (upper medial MPO)
- Femoral hernia - passes through the femoral ring below the inguinal ligament (lower medial MPO)
Key Anatomical Relations Within and Around the MPO
From the posterior (preperitoneal) perspective, the following structures are visible:
- Epigastric vessels - divide direct from indirect hernias
- Iliopubic tract - aponeurotic band from ASIS to Cooper's ligament; forms inferior margin of internal inguinal ring
- Cooper's ligament (pectineal ligament) - formed by the periosteum fused with the tendon of pectineus; key anchoring point in hernia repair
- Lacunar ligament (Gimbernat's ligament) - triangular medial border of the femoral canal
- Corona mortis - anastomosis between the obturator and inferior epigastric vessels crossing the pubic rim; injury causes dangerous bleeding
Surgical Zones of the MPO (Fischer's Classification)
Fischer's Mastery of Surgery describes three operative zones when approaching the MPO preperitoneally (TAPP/TEP):
| Zone | Location | Contents / Significance |
|---|---|---|
| Zone 1 | Lateral to internal inguinal ring and spermatic vessels | Bordered laterally by ASIS, posteriorly by psoas; contains "triangle of pain" (lateral femoral cutaneous, genitofemoral, and femoral nerves) |
| Zone 2 | Medial to inferior epigastric vessels | Site of direct hernias |
| Zone 3 | Central zone (inferior epigastric vessels, internal ring, spermatic cord, external iliac vessels) | Contains "triangle of doom" (external iliac a. and v.) - the most dangerous zone |
- Fischer's Mastery of Surgery (8th ed.), p. 6098-6099
Danger Zones During Preperitoneal Repair
| Triangle | Boundaries | Contains |
|---|---|---|
| Triangle of Doom | Vas deferens (medial), testicular vessels (lateral), peritoneal fold (inferior) | External iliac artery and vein - injury is catastrophic |
| Triangle of Pain | Iliopubic tract (superior), testicular vessels (medial), peritoneal fold (inferior) | Lateral femoral cutaneous, genitofemoral, and femoral nerves - injury causes neuropathy |
Clinical Significance
The concept of the MPO underpins all posterior/preperitoneal inguinal hernia repairs:
- TAPP (Transabdominal preperitoneal repair)
- TEP (Totally extraperitoneal repair)
- Stoppa repair (Giant prosthetic reinforcement of the visceral sac)
In all these techniques, the mesh is placed to cover the entire MPO, protecting against all three hernia types simultaneously. This is superior to anterior repairs that only address one defect at a time.
The "critical view of the myopectineal orifice" is the mandatory dissection endpoint in laparoscopic inguinal hernia repair, analogous to the "critical view of safety" in laparoscopic cholecystectomy.
This is a shared conversation. Sign in to Orris to start your own chat.