a patient having multiple episodes of stool in a dayvsince 2-3 years
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Now I have comprehensive material. Let me compile a thorough clinical response.
Chronic Diarrhea - Clinical Approach
Definition
Chronic diarrhea = ≥3 loose/watery bowel movements per day lasting >30 days (or >4 weeks). This patient's 2-3 year history firmly qualifies. The first step is to exclude fecal incontinence masquerading as diarrhea (a common diagnostic trap).
Step 1 - Classify the Diarrhea
The most practical framework divides chronic diarrhea into three mechanistic categories:
| Type | Key Feature | Fecal Osmotic Gap |
|---|---|---|
| Watery - Secretory | Persists with fasting; large volume | < 50 mOsm/kg |
| Watery - Osmotic | Stops with fasting | > 100 mOsm/kg |
| Fatty (Steatorrhea) | Oily, malodorous, floats; multiple flushes needed | Elevated fecal fat |
| Inflammatory | Blood/pus in stool, fever | Fecal calprotectin elevated |
Fecal osmotic gap = 290 - 2 × (stool Na+ + stool K+)
Step 2 - Differential Diagnosis
Most common causes overall: IBS-D, lactose intolerance, chronic infections, IBD, celiac disease
(Symptom to Diagnosis, 4th Ed.)
By Category
Osmotic diarrhea:
- Lactose intolerance (very common)
- Fructose malabsorption
- Mg2+-containing laxatives or antacids
- Poorly absorbed carbohydrates (sorbitol, mannitol)
Fatty/Malabsorptive diarrhea:
- Celiac disease
- Crohn's disease (small bowel)
- Pancreatic exocrine insufficiency (chronic pancreatitis - clue: history of alcohol, postprandial pain, steatorrhea, weight loss)
- Short bowel syndrome
- Small intestinal bacterial overgrowth (SIBO)
Inflammatory diarrhea:
- Ulcerative colitis / Crohn's disease (IBD)
- Microscopic colitis (often indistinguishable from IBS - requires biopsy)
- Infectious: C. difficile, TB, CMV, HSV, amebiasis, giardiasis
- Ischemic colitis, radiation colitis
- Colorectal neoplasia
Secretory diarrhea (non-osmotic, watery):
- IBS-D (most common - diagnosis of exclusion)
- Microscopic/collagenous colitis
- Bile acid malabsorption (especially after ileal resection)
- Laxative abuse (found in 15-26% at tertiary referral centers)
- Motility disorders: diabetic neuropathy, hyperthyroidism
- Neuroendocrine tumors: VIPoma, carcinoid syndrome, gastrinoma, mastocytosis
Step 3 - History Red Flags ("Alarm Features")
These demand urgent investigation and argue against functional causes:
- Hematochezia / rectal bleeding
- Unintentional weight loss
- Nocturnal diarrhea (wakes patient from sleep - points to organic disease)
- Fever
- Age >50 years with new onset
- Family history of IBD, celiac disease, or colorectal cancer
- Anemia (low Hb, low MCV/MCH)
- Hypoalbuminemia
- Perianal fistulas or skin tags (Crohn's)
- Extraintestinal: oral ulcers, arthritis, skin rashes (erythema nodosum, dermatitis herpetiformis), uveitis
Step 4 - Focused History Questions
Ask about:
- Stool character - watery, oily, bloody, mucous? (Bristol Stool Scale)
- Relationship to food - worse after dairy? (lactose), after fatty meals? (pancreatic/biliary)
- Does diarrhea stop with fasting? (If yes - osmotic; if persists - secretory)
- Nocturnal episodes?
- Travel history, sick contacts
- Current medications (metformin, PPIs, antibiotics, NSAIDs, olmesartan, chemotherapy, colchicine - all cause diarrhea)
- Prior surgeries (cholecystectomy - bile acid diarrhea; ileal resection)
- Alcohol use
- Family history of IBD or celiac
Step 5 - Initial Investigations
Blood Tests
- CBC - anemia (IBD, celiac), eosinophilia (parasites, EGE)
- Comprehensive metabolic panel - hypokalemia (secretory diarrhea), hypoalbuminemia
- CRP / ESR - inflammation (sensitivity 49%, specificity 73% for inflammatory diarrhea)
- IgA tissue transglutaminase (TTG-IgA) + total IgA - celiac disease screening
- TSH - hyperthyroidism
- Iron, folate, B12 - malabsorption
Stool Tests
- Fecal calprotectin or lactoferrin - best stool inflammatory marker (calprotectin: sensitivity 92%, specificity 82%)
- Fecal occult blood
- Stool culture, ova & parasites, Giardia antigen, C. difficile PCR - or multiplex PCR panel
- Qualitative or quantitative fecal fat (Sudan stain: sensitivity 76%, specificity 99%)
Endoscopy
- Colonoscopy with biopsies - highest diagnostic yield, finds diagnosis in up to 30% of referred patients. Even with normal mucosa, biopsies detect microscopic colitis
- Upper endoscopy + duodenal biopsy - if celiac disease suspected
- Ileoscopy to evaluate terminal ileum for Crohn's
Imaging
- CT or MR enterography if IBD or small bowel pathology suspected
Diagnostic Algorithm
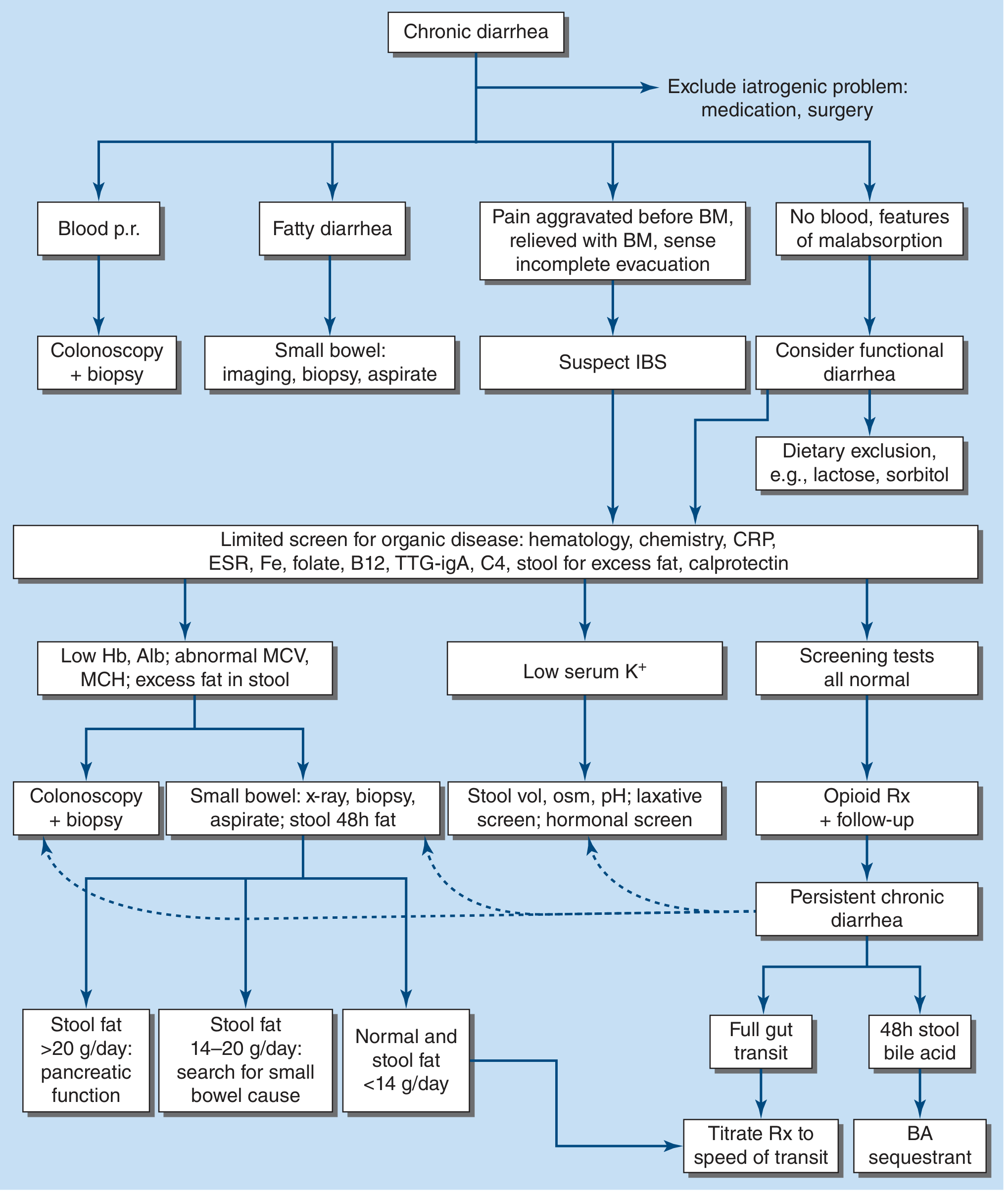
(Harrison's Principles of Internal Medicine, 22E, Fig. 49-4 - Algorithm for management of chronic diarrhea)
Step 6 - Management Principles
| Mechanism | Targeted Treatment |
|---|---|
| IBS-D (functional) | Antispasmodics, loperamide, low-FODMAP diet, tricyclic antidepressants, rifaximin |
| Lactose intolerance | Lactose-free diet, lactase supplements |
| Bile acid malabsorption | Cholestyramine, colestipol, colesevelam |
| Celiac disease | Strict gluten-free diet |
| IBD | 5-ASA, corticosteroids, immunomodulators, biologics |
| Microscopic colitis | Budesonide |
| SIBO | Rifaximin or rotating antibiotics |
| Pancreatic insufficiency | Pancreatic enzyme replacement |
| Giardiasis | Metronidazole or tinidazole |
| Secretory (neuroendocrine) | Somatostatin analogues (octreotide) |
Key Practical Points
- IBS-D is the most common diagnosis but is only made after excluding organic disease - never skip the workup.
- Microscopic colitis is clinically identical to IBS; it only shows up on biopsy - always biopsy a normal-looking colon in chronic diarrhea.
- Nocturnal diarrhea rules against IBS and strongly points to organic pathology.
- Laxative abuse accounts for 15-26% of cases at referral centers - ask tactfully.
- A therapeutic trial is appropriate in specific settings: e.g., lactose-free diet for suspected lactose intolerance, metronidazole for post-travel giardiasis, cholestyramine for post-cholecystectomy bile acid diarrhea.
Sources: Sleisenger & Fordtran's GI and Liver Disease; Harrison's Principles of Internal Medicine 22E; Symptom to Diagnosis, 4th Ed.
Celiac disease treatment
Reading File
Finding Sources
Searching PubMed
celiac disease treatment management
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent material gathered. Here is the comprehensive treatment guide:
Celiac Disease - Treatment
Overview
Celiac disease is a chronic, immune-mediated enteropathy triggered by dietary gluten (proteins from wheat, rye, and barley) in genetically predisposed individuals (HLA-DQ2/DQ8). Currently, the only proven treatment is a strict, lifelong gluten-free diet (GFD). There are no approved pharmacological alternatives as primary therapy.
1. Gluten-Free Diet (GFD) - The Foundation
What to Eliminate
| Avoid (Contain Gluten) | Safe Alternatives |
|---|---|
| Wheat, rye, barley | Rice, corn, maize |
| Most breads, pasta, cereals | Quinoa, buckwheat, millet |
| Most beers, lagers, ales, stout | Wines, ciders, most spirits (brandy, scotch), gluten-free beers |
| Many sauces, soups, dressings (hidden gluten) | Fresh unprocessed meats, fish, fruits, vegetables |
| Ice cream, sausages, fish sticks, cheese spreads (often contain wheat as filler) | Certified gluten-free labeled products |
Oats: Pure, uncontaminated oats are generally tolerated, but cross-contamination during milling is common - certified gluten-free oats only.
Hidden Gluten
Wheat flour is widely used as a thickener and filler in:
- Processed foods, precooked meals, convenience foods
- Medications and vitamin preparations
- Mixed seasonings and condiments
Food lists compiled in one country are not transferable to another - even same-brand foods may differ by region.
Response to GFD
- Symptom improvement: often within days to weeks
- Enterocyte height improvement: within 1 week
- Villus architecture normalization: may take months to 2 years or longer
- In ~50% of adults, biopsies show only partial improvement even on strict GFD; recovery is faster in children
Important notes:
- Some patients are so sensitive that trace amounts cause massive watery diarrhea within 1-2 hours ("gliadin shock" / celiac crisis)
- Accompanying lactase deficiency is common initially due to mucosal damage; dairy can be reintroduced once the mucosa heals
- A GFD often causes inadequate fiber intake, leading to constipation - replace with gluten-free fiber sources
- Weight gain is common after starting GFD as malabsorption resolves - avoid excess fat/calorie-rich GF processed snacks
2. Dietary Supplementation
Newly diagnosed patients require supplementation to correct malabsorption-related deficiencies:
| Deficiency | Supplement |
|---|---|
| Iron (most common) | Iron supplementation |
| Vitamin D | 400-2000 units/day (especially with steatorrhea) |
| Calcium | Total 1500 mg/day (dietary + supplemental 500-1500 mg/day) |
| Vitamin B12 | B12 supplementation |
| Folic acid | Folate supplementation |
| Vitamin K | If prolonged PT / evidence of bleeding |
| Zinc, niacin, magnesium | As needed |
| Daily GF multivitamin | Recommended for all patients |
Osteoporosis/Osteopenia: Risk is elevated in celiac disease. 1 year of GFD reverses osteopenia in most patients. Get bone mineral density (DEXA) scan at diagnosis. If secondary hyperparathyroidism present, calcium + vitamin D supplementation is essential.
Celiac crisis: Severe diarrhea + dehydration requires hospitalization with IV fluids and electrolyte replacement.
3. Glucocorticoids
Reserved for specific situations:
- Acute severe presentation / celiac crisis not responding to GFD alone
- Refractory celiac disease (RCD) - see below
4. Monitoring on Treatment
| What to Monitor | How | When |
|---|---|---|
| Dietary adherence | Consultation with expert dietitian | Regularly, especially in first year |
| Serologic response | Anti-tTG IgA levels (fall with adherence) | Every 6-12 months until normal |
| Mucosal healing | Follow-up duodenal biopsy | After ~2 years on GFD (or if symptoms persist) |
| Bone density | DEXA scan | At diagnosis, repeat at intervals |
| Nutritional labs | CBC, iron, B12, folate, vitamin D, calcium | Annually |
Key elements of management (NIH Consensus):
- Consultation with a skilled dietitian
- Education about the disease
- Lifelong adherence to GFD
- Identification and treatment of nutritional deficiencies
- Access to an advocacy group
- Long-term follow-up by a multidisciplinary team
5. Non-Responsive Celiac Disease (NRCD)
Defined as: persistent symptoms/signs despite strict GFD for >6-12 months (~10% of patients)
The most common cause is inadvertent gluten ingestion. A persistently elevated anti-tTG strongly suggests ongoing exposure.
Workup for NRCD:
- Re-review original diagnosis (confirm celiac, not mimicker)
- Expert dietitian assessment for hidden gluten, FODMAP intolerances
- Test for lactose/fructose intolerance
- Repeat duodenal biopsy + colonoscopy
- Rule out concurrent: IBS, microscopic colitis (6%), SIBO, pancreatic insufficiency, lactose intolerance
- If persistent villus atrophy - consider Refractory Celiac Disease (RCD)
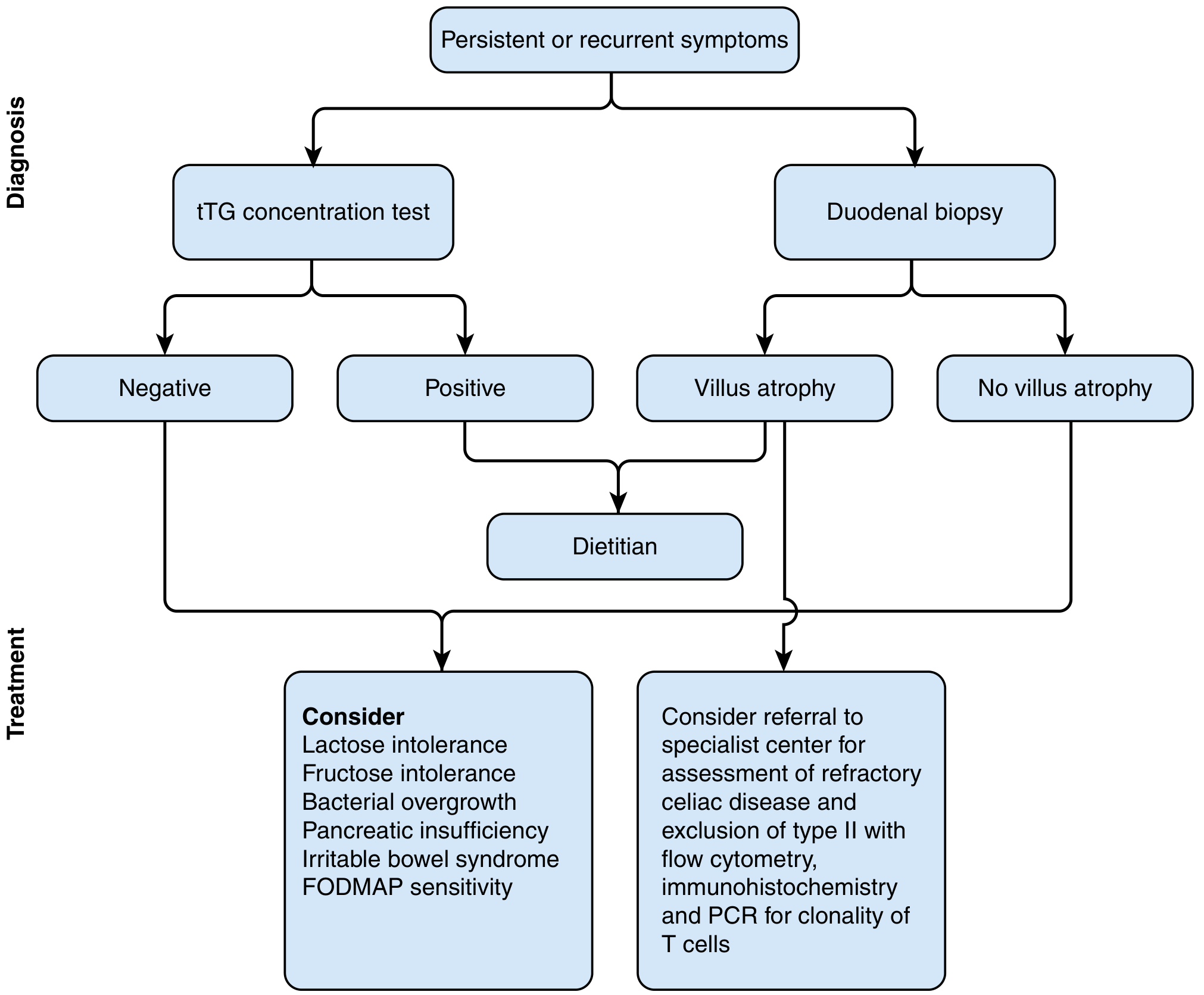
6. Refractory Celiac Disease (RCD)
Defined as: persistent malabsorption + villus atrophy despite strict GFD for >12 months, after excluding other causes.
| RCD Type I | RCD Type II | |
|---|---|---|
| IEL phenotype | Normal (CD8+) | Aberrant, undifferentiated, monoclonal (CD8-) |
| Risk | Lower | High - may progress to enteropathy-associated T-cell lymphoma (EATL) |
| Prognosis | Better | Markedly decreased 5-year survival |
Treatment of RCD:
- Enteric-coated budesonide (open-capsule technique for proximal small bowel delivery) - first-line for RCD, preferred over systemic steroids
- Small intestine-release mesalamine - good safety, useful for maintenance, less potent than budesonide
- Systemic prednisolone - if budesonide insufficient
- Azathioprine or 6-mercaptopurine - steroid-sparing if prednisolone ≥10 mg/day required
- Cyclosporine - improved histology in 61% in one pilot study; life-saving in occasional severe cases
- Infliximab (anti-TNF-α) - reported efficacy in some RCD cases
- Referral to specialist celiac center for flow cytometry, immunohistochemistry, and PCR for T-cell clonality
7. Complications to Screen For
| Complication | Notes |
|---|---|
| Lymphoma (EATL) | Rare but serious - risk in RCD type II; strictly GFD-adherent patients have near-normal risk |
| Small bowel adenocarcinoma | Rare but increased in celiac disease |
| Ulcerative jejunoileitis | Rare; strictures and ulceration; high overlap with lymphoma |
| Osteoporosis | Screen all patients with DEXA at diagnosis |
| Infertility / obstetric complications | GFD improves fertility outcomes |
| Hyposplenism | Increases risk of pneumococcal infections - vaccinate against pneumococcus |
8. Future / Investigational Therapies
Several non-dietary approaches are in clinical trials:
- Latiglutenase (IMGX003) - oral gluten-degrading enzyme
- ZED1227 - transglutaminase 2 inhibitor
- Larazotide acetate - tight junction regulator to reduce intestinal permeability
- AMG 714 (anti-IL-15) - for RCD type II
- HLA-DQ2-targeted peptide immunotherapy (tolerization approach)
None are currently approved as primary therapy.
Bottom line: The GFD remains the only effective treatment for celiac disease. About 70-80% of patients experience complete symptom resolution and mucosal healing on a strict GFD. The 10% who don't respond require systematic evaluation for inadvertent gluten exposure before labeling as refractory.
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Harrison's Principles of Internal Medicine, 22E; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.