In general examination explain each and every point and tell me what to in patients according to bailey and love and s das
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have rich content from both sources. Let me compile the comprehensive answer.
General Examination - Bailey & Love and S Das
General examination is the systematic assessment of the patient as a whole before proceeding to local/regional examination. Both texts emphasize that focusing only on a local lesion without a thorough general survey leads to "innumerable misdiagnoses" (S Das).
How to Set Up the Examination
- Perform in natural daylight (artificial light may miss faint jaundice)
- Patient should remove all clothing and be covered with a gown
- Female patients must have a nurse attendant
- Patient lies flat, hips and knees extended (a pillow allowed for comfort)
- For palpation, flex the hips and knees to relax abdominal muscles
- Proceed in a systematic sequence: inspection → palpation → percussion → auscultation
(S Das, Ch. 1 & 3; Bailey & Love, Ch. 63)
Components of General Examination
1. General Assessment of Illness
What to do: Observe the patient from the moment they enter the room.
- In a severely ill patient, prioritize - proceed rapidly to local examination and begin treatment rather than spending time on less important findings.
- Note whether the patient looks well, ill, or moribund.
- A cachectic patient with abdominal discomfort and a lump strongly suggests GI malignancy.
(S Das)
2. Mental State and Level of Consciousness
What to do: Assess orientation and responsiveness, especially in head injury or critically ill patients.
S Das defines 5 levels of consciousness:
| Level | Description |
|---|---|
| a | Fully conscious, correctly oriented to time, space, and person |
| b | Fully conscious but disoriented to time/space |
| c | Semi-conscious (drowsy) - can be awakened |
| d | Unconscious (stupor) - responds to painful stimuli only |
| e | Unconscious (coma) - no response to painful stimuli |
Always document level of consciousness and note any confusion, agitation, or delirium.
(S Das)
3. Build and State of Nutrition
What to do: Look at body habitus and estimate nutritional status.
- Obesity may point to hypothyroidism, Cushing's syndrome, or metabolic syndrome.
- Cachectic/wasted appearance with abdominal complaint suggests malignancy.
- Endocrine abnormalities (acromegaly, myxoedema, Marfan's) are recognizable from build alone.
- Record weight and BMI in elective settings (Bailey & Love).
(S Das; Bailey & Love)
4. Attitude (Posture/Decubitus)
What to do: Observe how the patient is lying or sitting - this gives immediate diagnostic clues.
| Attitude | Suggests |
|---|---|
| Lying completely still | Peritonitis (movement aggravates pain) |
| Restless, tossing in bed | Renal/biliary colic |
| Neck retraction and rigidity | Meningitis |
| Knees drawn up to abdomen | Peritonitis or severe abdominal pain |
| Unable to lie flat | Diffuse peritonitis (thin patient) |
(S Das; Bailey & Love)
5. Skin Color - Pallor, Cyanosis, Jaundice
Pallor (Anaemia)
Where to look: Lower palpebral conjunctiva, mucous membranes of lips and cheeks, nail beds, palmar creases.
- Causes: Massive haemorrhage, shock, intense emotion, anaemia (from any cause).
- Look for koilonychia (spoon-shaped nails) in iron deficiency anaemia.
- Chronic inflammatory/malignant swellings cause anaemia (low Hb%).
Cyanosis
Where to look:
- Peripheral cyanosis: Nail beds, tip of nose, skin of palms and toes.
- Central cyanosis: Tongue (key differentiator - tongue is spared in peripheral cyanosis), plus above sites.
Mechanism: Requires a minimum of 5 g/dL of reduced haemoglobin - therefore cyanosis is NOT detectable in severe anaemia.
| Type | Cause | Site affected |
|---|---|---|
| Peripheral | Reduced cardiac output, cold-induced vasoconstriction | Nail beds, nose tip, toes |
| Central | Pulmonary disease, cardiac R→L shunt | Tongue + all peripheral sites |
| Special | Methaemoglobinaemia, sulphaemoglobinaemia (e.g. phenacetin) | Generalized; normal arterial pO2 |
| CO poisoning | Carbon monoxide | Cherry-red discoloration |
Jaundice
Where to look: Sclera (patient looks down at feet while examiner opens eyelid), nail bed, lobule of ear, tip of nose, undersurface of tongue.
- Colour ranges from faint yellow (viral hepatitis) to dark olive-green (obstructive jaundice - due to biliverdin accumulation).
- Scratch marks on skin = obstructive jaundice (bile acid retention → pruritus).
- Distinguish from hypercarotinaemia (carotene staining): sclera is NOT icteric in hypercarotinaemia; it mainly affects the face, palms, and soles.
- In deep/longstanding jaundice, a greenish tint appears in sclerae and skin.
(S Das, pp. 9-11)
6. Oedema
What to do: Press the dorsum of the foot, medial aspect of the leg/ankle, and sacral region (in bedridden patients) with your thumb for 5 seconds, then release.
- Pitting oedema: Pit remains after pressure release - cardiac failure, hypoalbuminaemia (liver disease, nephrotic syndrome), venous obstruction.
- Non-pitting (brawny) oedema: No pit - lymphoedema (filariasis), myxoedema.
- Note: oedema is better seen in the ankles and feet in ambulant patients; in bedridden patients, check the sacral region.
- Also note periorbital oedema (nephrotic syndrome, angioedema).
(S Das; Bailey & Love)
7. Lymphadenopathy
What to do: Systematically examine all lymph node groups:
- Cervical (anterior and posterior chains), submandibular, submental, pre/post-auricular
- Axillary (central, anterior, posterior, medial, apical)
- Inguinal
- Virchow's node (left supraclavicular lymphadenopathy) - suggests intra-abdominal malignancy (Bailey & Love)
S Das stresses: in any lymph node enlargement, always examine all other groups to determine the cause (generalized vs. regional).
Note: hard, non-tender, irregular nodes suggest malignancy; soft, tender nodes suggest infection.
8. Hands
What to do: Examine both hands carefully for signs of systemic disease.
| Sign | Disease |
|---|---|
| Pallor of nail beds/palmar creases | Anaemia |
| Clubbing (loss of angle at nail base) | Lung cancer, bronchiectasis, cirrhosis, IBD, cyanotic heart disease |
| Koilonychia (spoon nails) | Iron deficiency anaemia |
| Leukonychia (white nails) | Hypoalbuminaemia (liver disease) |
| Palmar erythema | Chronic liver disease |
| Dupuytren's contracture | Liver cirrhosis, alcoholism |
| Asterixis (liver flap) | Hepatic encephalopathy |
| Finger clubbing + cyanosis | Cyanotic congenital heart disease |
(Bailey & Love, Ch. 63)
9. Head and Neck
What to do: Examine eyes, face, neck systematically.
- Eyes: Jaundice (sclerae), pallor (conjunctivae), exophthalmos (hyperthyroidism), Kayser-Fleischer rings (Wilson's disease), Horner's syndrome (apical lung/neck pathology)
- Face: Cushingoid facies, myxoedematous face, acromegalic features, malar flush (mitral stenosis)
- Neck: Thyroid enlargement, jugular venous pressure (JVP) for cardiac status, cervical lymphadenopathy, carotid pulsations
- Left supraclavicular node (Troisier's sign / Virchow's node) = intra-abdominal malignancy
(Bailey & Love)
10. Vital Signs
What to do: Always record all four vital signs. Bailey & Love calls this mandatory in every patient.
Pulse
- Rate (normal: 60-100/min), rhythm (regular/irregular), volume (full/thready), character (bounding/collapsing)
- Tachycardia: shock, infection, pain, anaemia, hyperthyroidism
- Bradycardia: hypothyroidism, raised ICP, heart block
Blood Pressure
- Both arms (differ by >10 mmHg = vascular pathology)
- Hypertension: renal disease, endocrine causes
- Hypotension + tachycardia = shock; note pulse pressure
Respiratory Rate
- Normal: 12-18 breaths/min
- Tachypnoea: pulmonary pathology, metabolic acidosis, pain, sepsis
- Cheyne-Stokes respiration: uraemia, raised ICP, cardiac failure
Temperature
- Normal: 37°C (98.6°F)
- Fever patterns help diagnosis: hectic fever = abscess; low-grade evening fever = tuberculosis
- Hypothermia: severe shock, hypothyroidism
(S Das; Bailey & Love)
11. Specific Examination in Suspected Malignancy (S Das)
When a swelling is suspected to be malignant, the general examination must include:
- Pulmonary metastasis: Enquire about cough, haemoptysis, chest pain; examine for consolidation and pleural effusion
- Hepatic metastasis: Examine liver for enlargement and nodularity
- Peritoneal metastasis: General abdominal examination
- Bony metastasis: Examine spine, pelvis, trochanters of femora, skull for tenderness
(S Das, p. 57)
12. Lymph Node Examination for Cause
When lymphadenopathy is present (S Das):
- Always examine ALL lymph node groups
- Generalized lymphadenopathy = systemic disease (lymphoma, leukaemia, HIV, TB)
- Regional lymphadenopathy = local cause in drainage area
Summary Checklist: General Examination Sequence
1. General assessment of illness (well/unwell/moribund)
2. Mental state and level of consciousness
3. Build, nutrition, body habitus, weight/BMI
4. Attitude and posture in bed
5. Skin: pallor, cyanosis (peripheral vs. central), jaundice
6. Oedema: ankles/feet, sacrum
7. Hands: clubbing, koilonychia, palmar erythema, flap
8. Head and neck: eyes, face, thyroid, JVP, lymph nodes
9. Vital signs: pulse, BP, RR, temperature
10. Lymph node groups: cervical, axillary, inguinal
11. If malignancy: lung, liver, abdomen, bones
12. Specific system examination based on chief complaint
Sources:
- S Das - A Manual on Clinical Surgery, 13th Edition, Chapter 1 (History & Physical Examination) and Chapter 3 (General Examination)
- Bailey & Love's Short Practice of Surgery, 28th Edition, Chapter 63 (Abdominal Examination and General Examination)
I have to examine from head to toe in sequence and can't return to area I already passed so tell me body area with related examination so I don't miss a point
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have the full head-to-toe structure from S Das and Bailey & Love. Now let me compile this into the definitive sequential guide.
Head-to-Toe Examination: Complete Sequential Guide
Based on S Das (Manual on Clinical Surgery) & Bailey and Love
Key rule: The patient lies flat, adequately exposed, in natural light. Examine each region completely before moving on - you cannot come back.
BEFORE YOU START (Patient Positioning & Setup)
- Natural daylight (artificial light misses faint jaundice)
- Patient fully undressed, covered by gown
- Lying flat, hips/knees extended (pillow allowed)
- Female patient: nurse attendant mandatory
- Start the moment the patient walks in (gait, posture, distress)
1. GENERAL FIRST IMPRESSION (Standing/Entering)
| What to assess | What to look for |
|---|---|
| General appearance | Well / ill / acutely distressed / moribund |
| Build | Obese, normal, thin, cachectic (wasted = suspect malignancy) |
| Nutrition | Well-nourished vs. malnourished |
| Gait | Antalgic, shuffling, ataxic, hemiparetic |
| Posture | Stooped, rigid, protective guarding |
| Mental state | Alert and oriented / confused / drowsy / stuporous / comatose |
| Decubitus (position in bed) | Lying still (peritonitis) vs. restless/tossing (colic) vs. knees drawn up |
(S Das: 5 levels of consciousness - fully conscious oriented → fully conscious disoriented → drowsy → stupor → coma)
2. HEAD
Eyes
- Conjunctiva (lower lid): Pallor = anaemia - pull down lower lid and look at palpebral conjunctiva
- Sclera: Jaundice (ask patient to look down at feet, open eyelid wide) - yellow = early; greenish-yellow = late/obstructive
- Pupils: Size, equality, reaction to light, accommodation reflex (PERLA)
- Eye movements: 3rd, 4th, 6th cranial nerves
- Exophthalmos: Hyperthyroidism
- Periorbital oedema: Nephrotic syndrome, angioedema
- Visual fields: Confrontation test
- Fundoscopy: Optic disc, papilloedema, hypertensive/diabetic changes
Ears
- Lobule of ear: Look for jaundice here (a sensitive site)
- Discharge, tophi (gout)
Nose
- Tip of nose: Pallor, cyanosis, jaundice (all visible here)
- Nasal flaring: Respiratory distress
Face/Skin
- Facies: Cushingoid (moon face, plethora), myxoedematous (puffy, dull), acromegalic (jaw protrusion), malar flush (mitral stenosis)
- Pigmentation: Addison's (buccal), Peutz-Jeghers (perioral)
- Skin colour: Pallor, cyanosis, jaundice, cherry-red (CO poisoning), scratch marks (obstructive jaundice = bile acid retention)
3. MOUTH AND THROAT
- Lips: Colour (cyanosis/pallor), pigmentation (Peutz-Jeghers syndrome), angular stomatitis (B12/iron deficiency), herpes labialis
- Teeth and gums: Dental hygiene, bleeding gums (scurvy), spongy gums
- Tongue:
- Colour: Pallor (anaemia), central cyanosis (blue tongue = TRUE central cyanosis - key differentiator from peripheral)
- Moisture: Dry tongue = dehydrated
- Papillae: Smooth bald tongue = B12 deficiency/iron deficiency/GI disorders
- Leukoplakia: White opaque patches on dorsum
- Undersurface and sides: Ulcers (especially at tongue margins - carcinoma)
- Furring: Infection, heavy smoking
- Midline rhomboid area: Median rhomboid glossitis
- Undersurface of tongue: Jaundice visible here
- Soft palate: Movement (9th/10th cranial nerve)
- Tonsils: Enlargement, exudate
- Buccal mucosa: Pallor, pigmentation
S Das: The tongue is key - central cyanosis makes the tongue blue; peripheral cyanosis does NOT affect the tongue.
4. NECK
Lymph Nodes
Palpate all cervical groups systematically:
- Submental → submandibular → anterior cervical chain → posterior cervical chain → pre-auricular → post-auricular → occipital
- Left supraclavicular (Virchow's/Troisier's node): If enlarged = intra-abdominal malignancy (Bailey & Love)
- Note: hard, irregular, non-tender = malignancy; soft, tender = infection
Neck Veins (JVP)
- Jugular venous pressure: Raised in cardiac failure, SVC obstruction
- Normal: <4 cm above sternal angle at 45°
Thyroid
- Inspect for swelling (ask patient to swallow - thyroid moves up)
- Palpate: Size, consistency, nodularity, tenderness
- Percuss for retrosternal extension
- Auscultate for bruit (hyperthyroidism)
Carotid Pulses
- Palpate each side separately (never both simultaneously)
- Bruit on auscultation
Trachea
- Position: Central or deviated? (Note - will reassess tracheal position at thorax too)
Neck Movements
- Restriction: Cervical spine pathology, meningism (Kernig's/Brudzinski's)
- Neck stiffness: Meningitis
Cranial Nerves (relevant to neck)
- 7th (facial): Smile, raise eyebrows, close eyes tight, show teeth
- 11th (accessory): Trapezius and sternomastoid power
- 12th (hypoglossal): Tongue protrusion - deviates to side of lesion
5. HANDS AND UPPER LIMBS
Do this BEFORE moving to the chest. The hands contain a wealth of systemic signs.
Nails (examine both hands together)
| Nail sign | Disease |
|---|---|
| Clubbing - loss of angle at nail base, fluctuant nail bed, beaking | Lung cancer, bronchiectasis, empyema, cyanotic heart disease, cirrhosis, IBD |
| Koilonychia (spoon-shaped, concave) | Iron deficiency anaemia, Plummer-Vinson syndrome |
| Leukonychia / Terry's nails (white nail bed) | Hypoalbuminaemia (liver disease) |
| Splinter haemorrhages (longitudinal under nail) | Infective endocarditis, vasculitis |
| Pitting | Psoriasis |
| Transverse grooves (Beau's lines) | Past systemic illness |
| Bitten nails | Anxiety neurosis |
| Pallor of nail beds | Anaemia |
| Cyanosis of nail beds | Peripheral cyanosis |
(S Das: "Splinter haemorrhages under the nails are manifestations of systemic vasculitis... Multiple splinter haemorrhages suggest infective endocarditis")
Palms and Hands
| Sign | Disease |
|---|---|
| Pallor of palmar creases | Anaemia |
| Palmar erythema (red palms) | Chronic liver disease, pregnancy |
| Dupuytren's contracture (palmar fibrosis, ring/little finger) | Liver cirrhosis, alcoholism, idiopathic |
| Tremor - fine resting tremor | Parkinsonism |
| Flapping tremor/asterixis (hold hands outstretched, dorsiflex wrists) | Hepatic encephalopathy, uraemia, CO2 retention |
| Thenar/hypothenar wasting | Median/ulnar nerve lesion |
| Sclerodactyly | Scleroderma |
Pulse (Radial)
- Rate: Count for 1 full minute (normal 60-100/min)
- Rhythm: Regular / irregularly irregular (AF) / regularly irregular
- Volume: Full and bounding (sepsis, hyperthyroidism) / thready (shock)
- Character: Collapsing/water-hammer (aortic regurgitation) - feel with forearm elevated
- Radio-radial delay: Aortic coarctation / subclavian artery stenosis
- Radio-femoral delay: Aortic coarctation
Arms
- Power, tone, reflexes: Biceps (C5/6), triceps (C7), supinator (C5/6)
- Sensation: Test in dermatomal pattern
- Axillae: Lymph nodes - central, anterior, posterior groups; skin rash/hidradenitis
- Joints: Elbows, wrists - swelling, tenderness, range of motion
- Blood pressure: Both arms (difference >10 mmHg = vascular/structural cause)
6. THORAX (CHEST)
Inspection
- Type of chest: Barrel (COPD), pigeon (rickets), funnel (pectus excavatum), kyphoscoliosis
- Respiratory rate: Normal 12-18/min - count for 1 minute without patient knowing
- Breathing pattern: Cheyne-Stokes (uraemia, cardiac failure, raised ICP), Kussmaul (metabolic acidosis), abdominal vs. thoracic breathing
- Symmetry of chest movement: Reduced on side of pathology
- Intercostal recession: Severe respiratory distress
- Dilated veins: SVC obstruction (flow upward), IVC obstruction (flow downward)
- Visible pulsations: Apex beat, aortic aneurysm
- Breasts (both sexes): Shape, skin changes, nipple retraction/discharge, asymmetry, scars
- Spine: Kyphosis, scoliosis, gibbus
Palpation
- Tracheal position: Central vs. deviated (to same side = collapse/fibrosis; to opposite = large effusion/pneumothorax)
- Apex beat: Normally 5th intercostal space, mid-clavicular line; displaced outward = cardiomegaly
- Chest expansion: Hands around chest - thumbs meet at midline, should move symmetrically 2-3 cm
- Vocal fremitus: "99" - increased = consolidation; absent/reduced = effusion/pneumothorax
- Tenderness: Rib fractures, Tietze's
Percussion
- Lungs: Resonant (normal) / dull (consolidation, effusion, collapse) / stony dull (effusion) / hyperresonant (pneumothorax)
- Cardiac border: Left border (3rd/4th/5th ICS)
- Liver dullness: Lower right chest (reduced = pneumoperitoneum!)
- Retrosternal thyroid: Dullness over manubrium
Auscultation - Lungs
- Breath sounds: Vesicular (normal) / bronchial (consolidation) / absent (effusion, pneumothorax)
- Added sounds: Crackles (fine = pulmonary oedema/fibrosis; coarse = bronchiectasis), wheeze (obstruction), pleural rub
- Vocal resonance: "99" - increased (consolidation), absent (effusion)
Auscultation - Heart
- Aortic area (2nd right ICS): Aortic stenosis murmur (ejection systolic, radiates to neck)
- Pulmonary area (2nd left ICS): Pulmonary stenosis; splitting of S2
- Tricuspid (lower left sternal border): Tricuspid murmurs
- Mitral (apex - 5th ICS MCL): Mitral stenosis (mid-diastolic, low-pitched rumble), mitral regurgitation (pan-systolic, radiates to axilla)
- Heart sounds: S1, S2; S3 (gallop = cardiac failure); S4 (stiff LV)
- Pericardial rub: Both systolic and diastolic, scratchy, positional
Temperature is recorded here - 37°C normal; >38°C fever; <36°C hypothermia. Record on chart.
7. ABDOMEN
Inspection (patient lying flat, knees/hips can be flexed for palpation)
- Contour: Flat, scaphoid (hollow = starvation), distended (fat/fluid/flatus/foetus/faeces/full bladder)
- Umbilicus: Central/displaced; everted (ascites, large mass); inverted (normal); Sister Mary Joseph's nodule (peritoneal mets)
- Skin: Scars (note location - gives clue to past surgery), striae, dilated veins (caput medusae = portal hypertension; flow away from umbilicus), hernias (ask patient to cough/strain)
- Grey Turner's sign: Bruising of flanks = retroperitoneal haemorrhage (severe pancreatitis, leaking AAA)
- Cullen's sign: Bruising around umbilicus = severe pancreatitis, ruptured ectopic, liver trauma (blood tracks along ligamentum teres)
- Visible peristalsis: Gastric outlet obstruction (left to right), intestinal obstruction (ladder pattern)
- Visible pulsation: Aortic aneurysm (midline pulsation)
- Movement with respiration: Absent chest movement with breathing = peritonitis
Palpation
- Light palpation first: Tenderness, guarding (voluntary vs. involuntary), rigidity (board-like = peritonitis)
- Deep palpation: Organomegaly, masses
- Liver: Start from RIF, move up; measure in cm below costal margin; note edge (smooth/irregular/nodular), surface, tenderness
- Spleen: Start from RIF, palpate toward left costal margin; cannot get above it; moves with respiration; notch on medial border
- Kidneys: Bimanual ballottement (loin to loin); can get above (unlike spleen); moves on respiration
- Bladder: Midline suprapubic mass, dull to percussion
- Aorta: Pulsatile midline mass (expansile = aneurysm)
- Abdominal reflexes: Stroke each quadrant toward umbilicus - absent in UMN lesions
- Rebound tenderness: Press slowly, release quickly; wince = peritoneal irritation (Blumberg's sign)
- Murphy's sign: Arrest of inspiration on palpation RUQ = acute cholecystitis
Percussion
- Liver dullness: Right side, upper and lower borders
- Spleen dullness: Left side
- Shifting dullness: Ascites - dull flanks, tympanic centre; shift when patient turns
- Fluid thrill: Large ascites
- Resonance over bowel
Auscultation
- Bowel sounds: Present/absent (absent = ileus/peritonitis; high-pitched tinkling = obstruction)
- Vascular bruits: Renal artery (laterally, above umbilicus), aortic bruit
Hernial Orifices
- Inguinal (deep and superficial ring): Ask patient to cough - impulse?
- Femoral ring
- Umbilicus
- Previous scars: Incisional hernia
Inguinal Lymph Nodes
- Horizontal group: Drains perineum, anus, external genitalia, lower limb
- Vertical group: Drains lower limb
Genitalia
- Males: Testes (size, consistency, tenderness, transillumination of scrotal swelling), epididymis, spermatic cord, phimosis
- Females: Gynaecological examination if indicated (with chaperone)
Rectal Examination (PR)
- Tone of sphincter, masses, tenderness (boggy = pelvic abscess), prostate (males - size/consistency), cervix/uterus (females), blood on glove
- Never omit in: rectal bleeding, change in bowel habit, pelvic pain, retention of urine
8. LOWER LIMBS
General
- Skin: Colour (pallor, cyanosis, gangrene), hair distribution (absent = arterial disease), varicose veins (tortuous dilated superficial veins), lipodermatosclerosis, venous eczema, pigmentation (haemosiderin)
- Muscle wasting: Thigh and calf comparison (measure circumference)
- Varicose veins: Distribution (long/short saphenous system), Trendelenburg test, cough impulse at saphenofemoral junction
Oedema
- Press firmly over dorsum of foot, medial malleolus, lower shin, then sacrum (if bedridden) for 5 seconds
- Pitting oedema: Pit remains = cardiac failure, hypoalbuminaemia, venous obstruction
- Non-pitting (brawny) oedema: No pit = lymphoedema (filariasis), myxoedema
Pulses - Vascular Assessment
- Femoral pulse: Femoral triangle, below inguinal ligament
- Popliteal pulse: Knee flexed, palpate deep in popliteal fossa with both thumbs
- Posterior tibial: Behind medial malleolus
- Dorsalis pedis: Lateral to extensor hallucis longus tendon on dorsum of foot
- Note: absent pulses → Buerger's test, ankle-brachial pressure index (ABPI)
Neurological
- Power: Hip flexion/extension, knee flexion/extension, ankle dorsi/plantarflexion (L2-S2)
- Tone: Spasticity (UMN) vs. flaccidity (LMN)
- Reflexes: Knee jerk (L3/4), ankle jerk (S1/2), plantar response (Babinski - extensor = UMN)
- Sensation: Light touch, pin-prick, vibration (128 Hz tuning fork on medial malleolus), proprioception (big toe)
- Coordination: Heel-shin test
Joints
- Hips, knees, ankles: Swelling, tenderness, range of movement, crepitus
- Gout: First MTP joint (podagra), tophi
9. BACK AND SPINE (Before asking patient to sit up)
- Spinal curvature: Kyphosis, lordosis, scoliosis
- Vertebral tenderness: Percuss each vertebra with fist - TB spine (gibbus at T12/L1), metastasis
- Paravertebral muscle spasm
- Sacroiliac joints: Press over each SIJ - ankylosing spondylitis
- Costovertebral angle tenderness: Renal disease (punch tenderness)
- Sacral oedema: Check sacral pad for pitting oedema (bedridden patients)
10. COMPLETION
Always end with:
- Temperature: If not already done
- Urinalysis: Naked eye and dipstick (colour, sugar, protein, blood, ketones)
- Specific examination if malignancy suspected (S Das):
- Chest: Pulmonary metastasis (consolidation, effusion)
- Liver: Hepatomegaly, nodular
- Abdomen: Peritoneal metastasis
- Spine/skull/pelvis/trochanters: Bony tenderness
QUICK REFERENCE CARD
HEAD → EYES → EARS → NOSE → MOUTH/TONGUE/THROAT
↓
NECK → Lymph nodes → JVP → Thyroid → Trachea → Cranial nerves
↓
HANDS → Nails → Palms → Pulse → BP → Arms → Axillae
↓
CHEST → Inspect → Palpate (apex, expansion, tactile fremitus)
→ Percuss → Auscultate (lungs + heart)
→ Breasts + Temperature
↓
ABDOMEN → Inspect → Palpate (light→deep, organs)
→ Percuss → Auscultate
→ Hernial orifices → Inguinal LN → Genitalia → PR
↓
LOWER LIMBS → Skin → Oedema → Pulses → Neuro → Joints
↓
BACK/SPINE → Curvature → Vertebral tenderness → SIJ → Renal angle
↓
COMPLETE → Urinalysis → Document vitals → Provisional diagnosis
S Das - A Manual on Clinical Surgery, 13th Ed., Ch. 1 & Ch. 3 | Bailey & Love's Short Practice of Surgery, 28th Ed., Ch. 63
Generate a detailed picture of human with site of examination reference to it
Generating Image
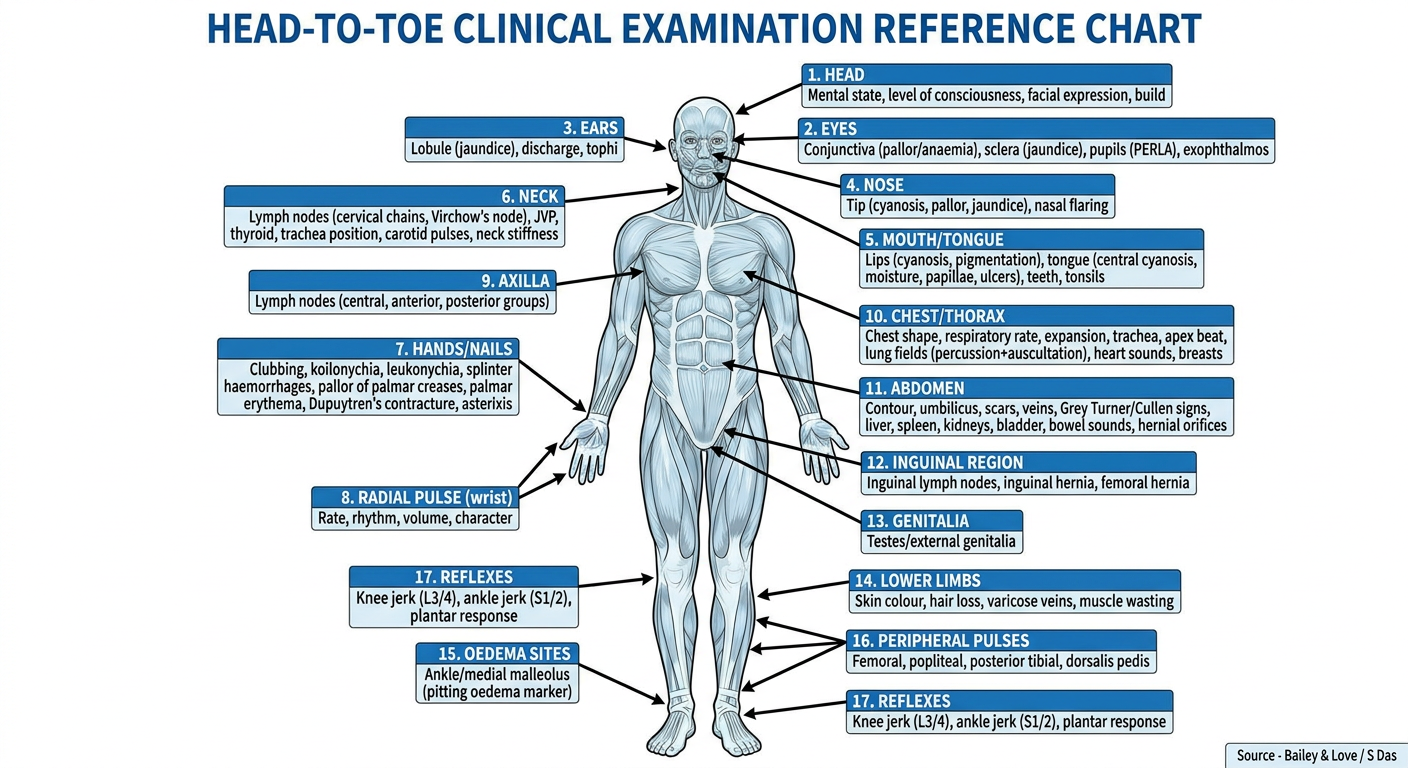
Here is your head-to-toe clinical examination reference chart. It maps every key examination point to its anatomical location on the body, following the sequence from Bailey & Love and S Das.
A few highlights to note on the chart:
- Eyes - lower palpebral conjunctiva for pallor, sclera for jaundice
- Mouth/tongue - the tongue is the single site that distinguishes central from peripheral cyanosis (tongue turns blue only in central)
- Neck - left supraclavicular node (Virchow's/Troisier's) is marked separately as it signals intra-abdominal malignancy
- Wrist - radial pulse site with rate, rhythm, volume and character assessment
- Chest - apex beat, lung fields, heart sound areas all mapped
- Abdomen - Grey Turner's (flanks) and Cullen's (umbilicus) signs are marked at their precise sites
- Ankle/medial malleolus - primary site for pitting oedema in ambulant patients
- Foot - dorsalis pedis and posterior tibial pulses for peripheral vascular assessment
Would you like a separate close-up diagram for any specific region - for example, the hand signs, the abdominal regions, or the lymph node groups?
This is a shared conversation. Sign in to Orris to start your own chat.