How to do a general anesthesia for a emergency c section
Reading File
Finding Sources
Finding Sources
Searching the Web
general anesthesia emergency cesarean section RSI protocol 2024 guidelines
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, authoritative content. Here is the complete answer:
General Anesthesia for Emergency Cesarean Section
General anesthesia (GA) is indicated when neuraxial anesthesia is contraindicated or time does not permit it - for example, profound fetal bradycardia, ruptured uterus, severe hemorrhage, cord prolapse, or abruptio placentae. Because pregnant women are at higher aspiration risk, Rapid Sequence Induction (RSI) is mandatory.
Why GA is High-Risk in Obstetrics
- Failed intubation rate in obstetric patients is at least 8x higher than in non-pregnant females
- Reduced lower esophageal sphincter competency + altered esophagogastric anatomy = high aspiration risk
- Airway edema worsens during labor (especially with preeclampsia, prolonged pushing, or tocolytic use)
- Awareness under anesthesia risk is elevated (RSI, deliberate dose limitation, NMBD use)
- Lower neonatal Apgar scores at 1 min vs. neuraxial - have a neonatologist/resuscitation team present
Step-by-Step Protocol
1. Pre-Induction Preparation
- Airway assessment (Mallampati, mouth opening, neck mobility) - do this even in a crash scenario
- If difficult airway anticipated: consider awake intubation or switch to neuraxial
- Left uterine displacement (wedge under right hip) - prevents aortocaval compression
- Standard monitoring: SpO2, NIBP (q2-3 min), ECG, capnography, temperature
- IV access (large bore, working)
- Equipment ready: video laryngoscope or direct laryngoscope, ETT (6.5-7.0 mm cuffed), bougie, supraglottic airway (LMA) as rescue, surgical cricothyrotomy kit
- Trained assistant for cricoid pressure
- Antacid prophylaxis: sodium citrate 30 mL oral, +/- ranitidine/omeprazole and metoclopramide if time allows
2. Pre-Oxygenation (Denitrogenation)
- Tight-fitting mask, 100% O2 for 3-5 minutes (standard)
- In true emergency: 4 maximal vital capacity breaths with 100% O2
- Apply apneic oxygenation via nasal cannula (15 L/min) during laryngoscopy to extend safe apnea time
- Head-up position (20-30 degrees) extends safe apnea window
3. Rapid Sequence Induction (RSI)
Administer induction agent + neuromuscular blocker in rapid succession, minimize/avoid bag-mask ventilation (or gentle mask ventilation at Pmax ≤20 cmH2O if desaturation risk is high):
| Agent | Dose | Notes |
|---|---|---|
| Propofol | 2 mg/kg | Most commonly used; caution in hemorrhage/hypotension |
| Ketamine | 1-1.5 mg/kg | Preferred if hemodynamically unstable; also bronchodilator |
| Etomidate | 0.2-0.3 mg/kg | Best for hemodynamic instability; single dose acceptable |
| Thiopental | 4-5 mg/kg | Historically used; less available now |
| Succinylcholine | 1-1.5 mg/kg | Classic choice - fastest onset, short duration; use if no contraindications |
| Rocuronium | 1.0-1.2 mg/kg | Equally effective alternative; sugammadex 16 mg/kg reverses it immediately if CICO |
- Succinylcholine remains the prototypic NMBD for RSI due to rapid onset and short duration
- Rocuronium 1.0-1.2 mg/kg is a safe alternative (intubating conditions within 60 seconds); if failed intubation occurs, sugammadex 16 mg/kg reverses it immediately even at that dose
- Apply cricoid pressure (Sellick's maneuver) via trained assistant - maintain until cuffed ETT placement confirmed
4. Intubation
- Use a cuffed ETT (size 6.5-7.0 mm)
- Maximum 2 laryngoscopy attempts by the primary operator; a 3rd only by an experienced colleague
- Confirm placement: capnography (gold standard) + bilateral auscultation
- Once confirmed: release cricoid pressure, surgeon may proceed with incision
5. Maintenance
- Volatile agent (isoflurane, sevoflurane, desflurane) at 0.5-0.75 MAC + 50% O2/N2O or 100% O2
- Keep volatile agent ≤1 MAC until delivery to minimize fetal depression and uterine relaxation
- TIVA (propofol infusion) is an option but increases awareness risk if dosing is insufficient
- After delivery of the baby:
- Increase volatile to full maintenance depth
- Add opioid (fentanyl, morphine) for analgesia
- Administer oxytocin IV (5-10 units slowly or infusion) to prevent uterine atony - avoid rapid bolus (causes hypotension)
- Nitrous oxide (N2O) can be used, but avoid or limit if bowel distension is a concern
6. Awareness Prevention
- Keep end-tidal volatile agent ≥ 0.7-1.0 MAC after delivery
- Consider BIS/depth-of-anesthesia monitoring - especially high-risk: young female, emergency, RSI, intraoperative TIVA
- Pre-induction midazolam can be used if time allows and fetal status is not critical
7. Emergence and Extubation
- At end of surgery, reverse neuromuscular blockade:
- Succinylcholine: spontaneous recovery
- Rocuronium: sugammadex 2-4 mg/kg (200 mg for 70 kg) at train-of-four 2 twitches
- Or neostigmine + glycopyrrolate if rocuronium at standard dose
- Extubate only when patient is:
- Fully awake and responsive to commands
- Adequate tidal volumes and airway reflexes restored
- SpO2 maintained on room air
- Consider sitting up / head-up before extubation to reduce aspiration risk
Failed Intubation Algorithm (OAA/DAS)
The master algorithm from the Obstetric Anaesthetists' Association and Difficult Airway Society:
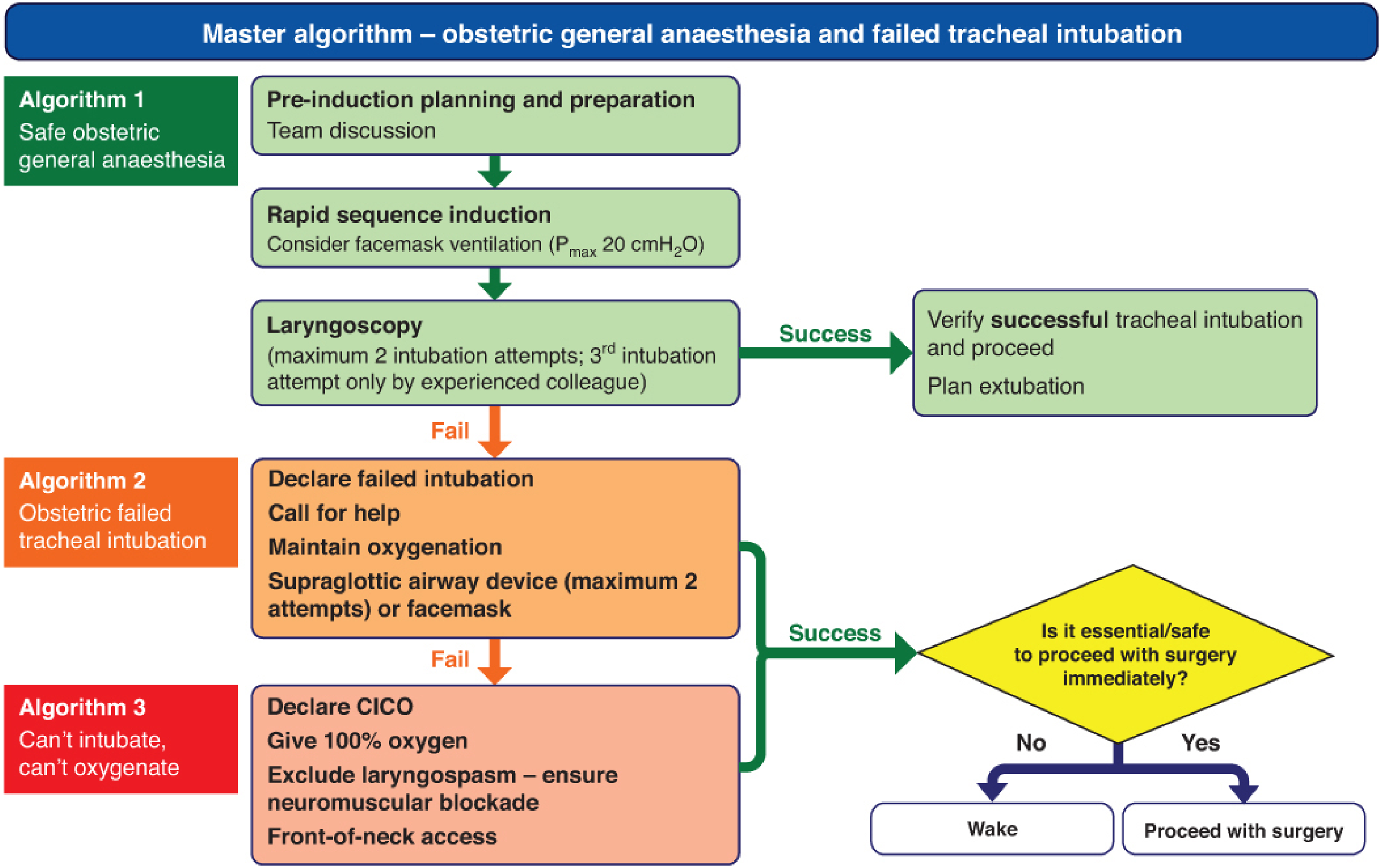
Key points:
- Algorithm 1 (Safe GA): Pre-induction planning -> RSI -> laryngoscopy (max 2 attempts, 3rd by senior) -> successful intubation -> proceed
- Algorithm 2 (Failed intubation): Declare failure, call for help, maintain oxygenation with supraglottic airway (max 2 attempts) or facemask -> if oxygenation maintained, decide: is it essential/safe to proceed? If yes, proceed with surgery; if no, wake patient
- Algorithm 3 (CICO - Can't Intubate, Can't Oxygenate): Declare CICO, 100% O2, exclude laryngospasm, ensure full NMB, front-of-neck access (surgical cricothyrotomy)
Special Considerations
| Situation | Modification |
|---|---|
| Preeclampsia | Attenuate hypertensive response to laryngoscopy (esmolol, labetalol, remifentanil, lidocaine); beware edematous airway; magnesium may cause uterine atony and prolong NMB |
| Hemorrhage/instability | Ketamine for induction; avoid propofol; have vasopressors ready (ephedrine, phenylephrine, noradrenaline) |
| Difficult airway predicted | Consider awake fibreoptic intubation or have video laryngoscope immediately available |
| Obese patient | Ramped position (ear-to-sternal notch), shorter safe apnea time, higher aspiration risk |
Postoperative Analgesia (after GA C-section)
Because neuraxial opioids weren't given, use multimodal analgesia:
- IV paracetamol (1g q6h) + NSAIDs (ketorolac, ibuprofen) if not contraindicated
- TAP block (transversus abdominis plane) or QL block - effective when neuraxial morphine not given
- PCA morphine/hydromorphone if severe pain
- Avoid codeine, tramadol, and meperidine in breastfeeding mothers
Sources: Barash Clinical Anesthesia 9e, p. 3499-3502; Miller's Anesthesia 10e (NMB in C-section); ASA Practice Guidelines for Obstetric Anesthesia; OAA/DAS Master Algorithm (Fig. 41-2)
What Are the Phases of anesthesia according to geudel and when is take right time to extubate?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
I have all the core content needed. Here is the complete, authoritative answer:
Guedel's Stages of Anesthesia + When to Extubate
Arthur Guedel (1920) originally described these stages from observations of diethyl ether anesthesia. They remain the classical framework for understanding depth of anesthesia, even though modern agents behave somewhat differently.
The Four Stages (Guedel's Classification)
Stage I - Analgesia
- Patient is awake but sedated, responds to verbal commands
- Pain is reduced; no amnesia early in this stage
- Late in Stage I: both analgesia and amnesia are present
- Reflexes: intact, respiration normal and regular
- Clinically: the "pre-induction" or "induction" zone; patient may feel dizzy or hear sounds but tolerate minor procedures
Stage II - Excitement (Delirium)
- Patient appears delirious, may shout, laugh, or vocalize
- Completely amnesic - no memory of this phase
- Respiration is irregular, rapid, and unpredictable; may hold breath or vomit
- Heart rate and blood pressure increase
- Reflexes are exaggerated - risk of laryngospasm, vomiting, breath-holding
- This stage is dangerous - the goal is to pass through it as quickly as possible by rapidly increasing the anesthetic concentration
- Key clinical point: Never extubate during Stage II - highest risk of laryngospasm, breath-holding, airway obstruction, and aspiration
Stage III - Surgical Anesthesia
This is the target for all surgical procedures. Guedel divided it into 4 planes based on ocular movements, eye reflexes, and pupil size:
| Plane | Eye Movements | Pupils | Respiration | Reflexes | Clinical Use |
|---|---|---|---|---|---|
| Plane 1 | Roving/conjugate eye movements present | Normal, miosis | Regular, thoraco-abdominal | Eyelid reflex lost; swallowing reflex still present | Light surgical plane |
| Plane 2 | Eye movements cease, eyes fixed and central | Mildly dilated | Regular, purely thoracic (diaphragmatic begins) | Laryngeal reflex lost - safer for intubation | Most general surgery |
| Plane 3 | Fixed, dull eyes | Dilated, loss of light reflex beginning | Intercostal muscles begin to fail; diaphragm predominates | Corneal and peritoneal reflexes lost | Deep surgery (abdominal) |
| Plane 4 | Fixed | Maximally dilated, no light reflex | Intercostal paralysis complete; only diaphragmatic breathing (then apnea) | All reflexes lost | Overdose territory - avoid |
- Planes 1-2: Light surgical anesthesia (minor/surface procedures)
- Plane 2-3: Standard surgical anesthesia (most operations)
- Approaching Plane 4: Danger zone
Stage IV - Medullary Depression (Overdose)
- Severe CNS depression including the vasomotor center and respiratory center in the medulla
- Circulatory collapse, complete apnea
- Death will rapidly follow without circulatory and ventilatory support
- Represents anesthetic overdose
Summary Diagram
Stage I Stage II Stage III Stage IV
(Analgesia) → (Excitement) → [Plane 1 | Plane 2 | Plane 3 | Plane 4] → (Medullary Depression)
↑
SURGICAL TARGET
(Planes 1-3)
When is the Right Time to Extubate?
Extubation can be performed either awake (most common and safest) or deep (selected cases). The key rule is:
Never extubate in Stage II. The patient must either be in deep Stage III (deep extubation) or fully awake with returned reflexes (awake extubation).
Awake Extubation (Standard/Preferred)
Performed when the patient has returned protective airway reflexes. Criteria:
Consciousness/Neurological:
- Responds to verbal commands ("open your eyes," "squeeze my hand")
- Eyes open spontaneously
- Purposeful movement
Respiratory:
- Adequate spontaneous tidal volume (>5 mL/kg) and respiratory rate
- SpO2 maintained on FiO2 ≤ 0.4
- EtCO2 < 55 mmHg
- Able to sustain head lift for 5 seconds (classic test of NMB reversal)
Neuromuscular:
- Train-of-Four (TOF) ratio ≥ 0.9 before extubation
- Full reversal confirmed with sugammadex or neostigmine if NMB given
Airway:
- Cuff leak present (especially after prolonged intubation or head/neck surgery)
- Secretions suctioned from oropharynx
- No active bleeding in airway
Deep Extubation (Selected Cases)
Used to avoid coughing, bucking, hypertension spikes - e.g., in eye surgery, neurosurgery, ENT.
Requirements:
- Patient is in deep plane of Stage III anesthesia (no response to deep suction or jaw thrust)
- Adequate spontaneous ventilation on minimal ventilator settings
- SpO2 maintained
Absolute contraindications to deep extubation:
- Difficult airway (cannot re-intubate safely)
- High aspiration risk (full stomach, GERD, obesity, obstetric patients)
- OSA (obstructive sleep apnea)
- Copious secretions or oral bleeding
- Inadequately trained PACU staff
The Stage II Trap - Why It's Dangerous
As the patient emerges from anesthesia, they pass back through Stage III → Stage II → Stage I → awake. If the endotracheal tube is removed during Stage II:
- Laryngospasm (glottic closure reflex exaggerated)
- Breath-holding / apnea
- Vomiting and aspiration
- Upper airway obstruction
- Hypertension / tachycardia from sympathetic surge
So the rule is: extubate either deep in Stage III (before reaching Stage II on the way out) or fully awake in Stage I (after passing through Stage II). Never in between.
Quick Reference: Extubation Readiness Checklist
| Parameter | Target |
|---|---|
| Consciousness | Follows commands, eye opening |
| Respiration | Spontaneous, TV > 5 mL/kg, RR 8-20 |
| Oxygenation | SpO2 > 95% on FiO2 ≤ 0.4 |
| Capnography | EtCO2 < 50-55 mmHg |
| NMB reversal | TOF ratio ≥ 0.9 |
| Airway reflexes | Cough, swallow present |
| Temperature | Normothermic (hypothermia prolongs NMB) |
| Hemodynamics | Stable HR and BP |
| Secretions | Oropharynx suctioned clear |
Sources:
- Guedel's stages: Katzung's Basic and Clinical Pharmacology 16e, p. 701 - "Traditionally, anesthetic effects on the brain produce four stages... (Guedel's signs, derived from observations of inhaled diethyl ether)"
- Extubation criteria and deep vs. awake extubation: Barash Clinical Anesthesia 9e, p. 3767-3769
This is a shared conversation. Sign in to Orris to start your own chat.