DJ stenting
Reading File
Finding Sources
Finding Sources
Searching the Web
DJ stenting ureteral double J stent procedure indications complications
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Now I have comprehensive information to provide a thorough answer on DJ stenting.
DJ (Double-J) Ureteral Stenting
What Is a DJ Stent?
A Double-J (DJ) stent - also called a double pigtail stent or JJ stent - is an internal ureteral stent consisting of a hollow tube with two coiled (pigtail) ends that span the full length of the ureter. The proximal coil sits in the renal pelvis, and the distal coil curls in the bladder. These J-shaped coils anchor the stent and prevent migration in either direction.
The standard design has:
- Drainage holes in both pigtails and along the shaft
- Made of polymer material (polyurethane, silicone, or newer biocompatible polymers)
- Sizes typically 6-8 French in diameter, lengths 22-28 cm depending on patient height
Grainger & Allison's Diagnostic Radiology - the standard design is a hollow tube with a double pigtail (or double J) stent, which covers the full length of the ureter, with drainage holes in both pigtails and in some designs along the shaft.
Indications
| Category | Specific Indication |
|---|---|
| Obstruction relief | Ureteral calculi causing acute obstruction, ureteral strictures (benign or malignant), extrinsic compression (tumor, fibrosis) |
| Post-surgical splinting | After ureteroscopy, pyeloplasty, ureterolithotomy, ureteral repair, reimplantation |
| Perforation/trauma | Ureteral perforation during instrumentation (6-8 Fr stent for 2-6 weeks allows healing) |
| Pre-procedural | Passive ureteral dilation before ureteroscopy in a narrow ureter; prior to ESWL to prevent steinstrasse |
| Pregnancy | Symptomatic hydronephrosis or obstructing calculus not passing spontaneously |
| Renal transplant | Post-ureteral anastomosis to prevent stricture and urinary leak |
| Sepsis with obstruction | Retrograde stenting (or PCN) to achieve urgent decompression in infected obstructed system |
Smith & Tanagho's General Urology - Double-J catheters are used to facilitate internal drainage due to obstruction from ureteral angulation and internal or external ureteral compression; they also help decrease the likelihood of sepsis or obstruction in the presence of steinstrasse after ESWL.
Note: Antegrade primary stenting is contraindicated in infected obstructed systems - external nephrostomy drainage first.
Routes of Insertion
1. Retrograde (Endoscopic)
- Done via cystoscopy under fluoroscopic guidance
- Guidewire passed up the ureter, stent threaded over wire
- Most common approach for benign disease and uncomplicated stone disease
2. Antegrade (Percutaneous)
- Percutaneous renal access, nephrostogram to map obstruction
- Wire negotiated across stricture, stent advanced antegrade into bladder
- Technical success ~85% for primary antegrade; ~100% after prior nephrostomy drainage
- Preferred in pelvic malignancy or when retrograde approach fails
Stent Sizing
Diameter:
- 6 Fr - bypass ureteral calculi or inflammatory strictures
- 8 Fr - malignant, ischemic, or post-surgical strictures (higher flow required)
Length (based on patient height):
- Height < 175 cm → 22 cm stent
- Height 175-195 cm → 24 cm stent
- Height > 195 cm → 26 cm stent
- Transplant ureters → ~12 cm
- Urostomy patients → typically 22 cm or shorter
A lumen >5 Fr can accommodate a flow rate of up to 10 mL/min with minimal rise of intrapelvic pressure. - Grainger & Allison's Diagnostic Radiology
Consequences of wrong size:
- Too long: severe irritative voiding symptoms (distal coil irritates trigone)
- Too short: proximal migration beyond ureteral orifice, inadequate drainage
Mechanism of Drainage
Drainage occurs both through the internal lumen via side holes and around the catheter in the periureteral space. The stent disrupts normal ureteral peristalsis, so early drainage is largely passive, dependent on the renal-to-bladder pressure gradient. Peristalsis is rarely seen on imaging before 2 months post-insertion.
Pathophysiological Changes After Stenting
All stents cause:
- Reactive urothelial hyperplasia
- Thickened mucosa and periureteral inflammation
- Reduced/ineffective peristalsis
- Biofilm formation (leading eventually to encrustation)
- Rise in intrapelvic pressures
Benign strictures allow drainage around the stent as the ureter dilates (persistent drainage). Malignant tissue does not permit such dilatation.
Complications
Early Complications
| Complication | Notes |
|---|---|
| Hematuria | Common, usually self-limiting |
| Dysuria / frequency | Affects up to 50% of patients; due to bladder coil irritation |
| Flank/loin pain on voiding | Vesicoureteral reflux up the stent during bladder contraction |
| UTI / bacteriuria | Biofilm on stent surface |
| Stent malposition | Proximal migration (~0.9%) or distal migration (~0.7%) |
Late Complications
| Complication | Notes |
|---|---|
| Encrustation | Incidence 832/50,000 cases in one large series; risk increases after 4-6 weeks in pregnancy; needs regular exchange every ~6 months for plastic stents |
| Obstruction / blocked stent | ~925 cases/50,000 in one series; inefficient drainage |
| "Forgotten stent" | Missed removal leading to heavy encrustation; CT needed to assess extent; requires PCNL + ESWL + URS combination |
| Stent fragmentation | Rare (52/50,000 cases) |
| Retroperitoneal looping | During antegrade insertion; use peel-away sheath to prevent |
| False passage | During stricture cannulation; stop, start antibiotics, insert protective nephrostomy, retry after 3-7 days |
Plastic ureteric stents are easy to insert, efficient and economical but are associated with significant stent-related symptoms (especially dysuria). In many cases, they can encrust or become infected and can also lead to haematuria. They also need to be exchanged every 6 months or so. - Grainger & Allison's Diagnostic Radiology
DJ Stent vs. Percutaneous Nephrostomy (PCN)
| Feature | DJ Stent | PCN |
|---|---|---|
| Route | Retrograde (endoscopic) | Antegrade (percutaneous) |
| Anesthesia | General/spinal preferred | Local anesthesia possible |
| Bacteremia risk | Higher | Lower |
| Quality of life | Similar | Similar |
| Preference | Benign disease, coagulopathy | Pelvic malignancy, infected obstruction, retrograde failure |
| External drainage | No | Yes |
In uncontrolled UTI from obstructing stone: PCN is generally preferred as it can be done under local anesthesia and is less likely to cause bacteremia.
Management of Stent-Related Symptoms
- Alpha-blockers (e.g., tamsulosin 0.4 mg/day) - reduce stent-related symptoms including lower urinary tract symptoms and flank pain; supported by multiple RCTs and meta-analyses
- Antimuscarinics - may help bladder irritative symptoms
- Combination therapy (alpha-blocker + antimuscarinic) - may offer additional benefit
Stent Removal
- Removed cystoscopically using forceps via flexible or rigid cystoscope
- Alternatively, a string attached to the distal end (left exiting through the urethra) allows outpatient removal by pulling
- Timing is individualized - in post-transplant patients, typically at 3 weeks
- Prevention of "forgotten stent": stent cards, log books, smartphone app reminders, computerized tracking registries
Metal Stents (for Long-Term Use)
For malignant or recurrent strictures where plastic stents fail, metallic options include:
- Resonance stent - braided metal double pigtail; more rigid, used in malignant strictures
- Memokath stent - NiTiinol alloy; removable even years later with cold water flush
- Uventa / Allium stents - large caliber (20-30 Fr), self-expanding, PTFE-covered; inserted antegrade through 9-10 Fr sheaths
- Metal stents are more durable but can still encrust, dislodge, and cause the same range of symptoms as plastic stents
Sources: Smith & Tanagho's General Urology (19th Ed.) | Grainger & Allison's Diagnostic Radiology | Campbell-Walsh-Wein Urology | Comprehensive Clinical Nephrology (7th Ed.) | Hinman's Atlas of Urologic Surgery
Liposarcoma
Reading File
Finding Sources
Finding Sources
Searching the Web
liposarcoma subtypes pathology molecular features treatment 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a complete, well-organized answer on liposarcoma.
Liposarcoma
Overview
Liposarcoma is the most common soft tissue sarcoma (STS) in adults, accounting for approximately 15-20% of all STS. It represents 45% of all retroperitoneal sarcomas. These tumors typically arise in the deep soft tissues of the proximal extremities and retroperitoneum, predominantly in individuals in their 50s and 60s. There is no significant sex predilection.
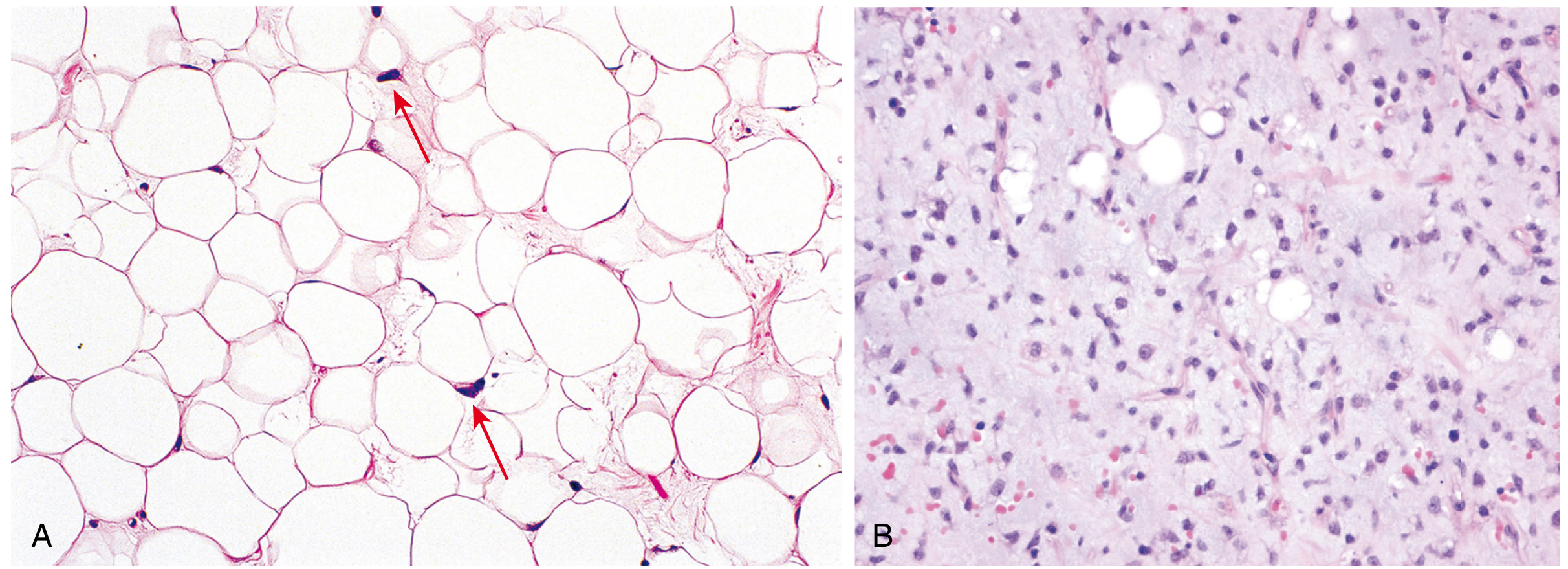
The hallmark diagnostic cell is the lipoblast - an immature fat cell with a hyperchromatic nucleus that is indented or scalloped by cytoplasmic lipid vacuoles.
WHO Classification - Subtypes
The 2020 WHO Classification of Soft Tissue and Bone Tumors recognizes five subtypes:
| Subtype | Frequency | Typical Location | Grade | Molecular Alteration |
|---|---|---|---|---|
| Well-differentiated (WDL) / Atypical Lipomatous Tumor (ALT) | Most common | Retroperitoneum (WDL), extremities/trunk (ALT) | Low | MDM2 + CDK4 amplification (12q13-15) |
| Dedifferentiated (DDLPS) | ~10% of WDL/ALT undergo this | Retroperitoneum | Variable (usually high) | MDM2 + CDK4 amplification + complex gains |
| Myxoid (MLPS) | 2nd most common; ~10% adult STS | Extremities (thigh) | Low-intermediate | t(12;16) → FUS::DDIT3 fusion |
| Pleomorphic (PLPS) | Least common | Extremities | High | Complex karyotype, no consistent mutation |
| Myxoid Pleomorphic | Rare, newly recognized | - | High | - |
Liposarcoma is a malignant tumor of adipose tissue, is the most common sarcoma of adulthood. - Robbins & Cotran Pathologic Basis of Disease
1. Well-Differentiated Liposarcoma (WDL) / Atypical Lipomatous Tumor (ALT)
The same tumor - different names based on location:
- ALT - extremities and superficial trunk (surgically resectable, hence better prognosis)
- WDL - retroperitoneum, mediastinum, pelvis, spermatic cord (harder to resect completely)
Histology:
- Mature adipocytes of varying sizes
- Scattered atypical spindle stromal cells with hyperchromatic nuclei
- Rare lipoblasts
- Fibrous bands (sclerosing variant) or dense inflammatory infiltrate (inflammatory variant)
Molecular: Amplification of chromosome 12q13-15 containing MDM2 and CDK4 genes. MDM2 promotes proteasomal degradation of p53; CDK4 inhibits Rb1. These appear as supernumerary ring chromosomes or giant marker chromosomes on cytogenetics.
Key IHC: MDM2 and CDK4 nuclear positivity - distinguishes WDL from benign lipomas, and distinguishes DDLPS from undifferentiated sarcoma.
Behavior:
- No metastatic potential in pure form
- Local recurrence in retroperitoneum is frequent (and causes morbidity)
- ~10% risk of dedifferentiation (time-dependent)
- Long-term survival is excellent for extremity tumors (ALT)
2. Dedifferentiated Liposarcoma (DDLPS)
Definition: Transition of ALT/WDL to a non-lipogenic sarcomatous component, either de novo (90%) or in recurrence (10%).
Histology:
- Abrupt or gradual transition from well-differentiated fatty areas to non-lipogenic sarcoma
- Dedifferentiated component is usually high-grade undifferentiated pleomorphic sarcoma
- Heterologous differentiation in ~10% (myogenic, osteosarcomatous, chondrosarcomatous)
Molecular: Same 12q13-15 amplification as WDL, but with additional coamplification involving 1p32 and 6q23 (JUN and ASK2 gene activation) and other complex gains.
Behavior: Higher risk of distant metastasis vs. WDL. Local recurrence common. Intermediate-grade behavior (grade 2 of malignancy overall).
Imaging clues to dedifferentiation:
- Tumor hypervascularity
- Areas of necrosis or cystic change
- Adjacent organ invasion
- Focal nodular or water-density areas within a fatty mass
3. Myxoid Liposarcoma (MLPS)
Epidemiology: Second most common subtype; accounts for ~10% of adult STS. Arises in young to middle-aged adults. Strong predilection for the thigh (deep soft tissues).
Histology:
- Abundant basophilic (myxoid) extracellular matrix
- Arborizing (chicken-wire) capillary network - characteristic
- Primitive mesenchymal cells and lipoblasts at various stages of adipocyte differentiation resembling fetal fat
- When >5% round cells are present: round cell liposarcoma (high-grade variant, worse prognosis)
Molecular:
- t(12;16)(q13;p11) → FUS::DDIT3 fusion gene (most common, ~90%)
- t(12;22)(q13;q12) → EWSR1::DDIT3 fusion (rare)
- These fusions arrest adipocyte differentiation
- Downstream activation of MET, RET, and PI3K/Akt pathways
Unique metastatic pattern: Tends to metastasize to the retroperitoneum and other unusual soft tissue sites (bone, contralateral extremity) - different from other STS which prefer lungs. Therefore, staging with CT chest/abdomen/pelvis is needed.
Behavior:
- Intermediate local recurrence and metastatic risk (~20% and ~50% respectively)
- Radiosensitive and chemosensitive - more responsive than other subtypes
- 10-year disease-specific survival: ~87%
- Round cell variant: worse, distant metastasis in up to 21%
- Trabectedin is particularly effective in this subtype
4. Pleomorphic Liposarcoma (PLPS)
Epidemiology: Rarest subtype. Predilection for extremities of adults. Can arise de novo or from a pre-existing lesion.
Histology:
- Sheets of anaplastic cells with bizarre pleomorphic nuclei
- Variable numbers of pleomorphic lipoblasts (sine qua non for diagnosis)
- High-grade sarcoma pattern
Molecular: Complex karyotypes with no consistent genetic abnormality - no known targetable mutations.
Behavior: Aggressive, frequently metastasizes. Poor prognosis.
Imaging Features
Differentiating liposarcoma from lipoma (CT/MRI):
| Feature | Lipoma | Liposarcoma (suspect) |
|---|---|---|
| Size | Usually < 10 cm | Often > 10 cm |
| Fat content | Homogeneous fat signal (>75%) | < 75% adipose tissue |
| Septa | Thin (< 2 mm), no enhancement | Thick (> 2 mm), nodular, enhancing septa |
| Non-adipose areas | None | Present (globular/nodular) |
| Fat suppression | Complete | Incomplete |
MRI specifics:
- WDL/ALT: predominantly fat signal with thin septa
- DDLPS: non-lipomatous discrete nodule within fatty mass; hypervascularity, necrosis
- Myxoid: fluid-like myxoid stroma + thin T1-hyperintense fatty septa ("lacy fat")
- Pleomorphic: little fat signal; appears as high-grade non-specific soft tissue mass
CT appearance of retroperitoneal liposarcoma is highly variable: from simple fatty tumors with thin septa (WDL) to complex masses with solid non-fat components (DDLPS). - Sabiston Textbook of Surgery
Staging and Diagnosis
- Biopsy: Image-guided core needle biopsy is standard. For deep retroperitoneal masses, percutaneous CT-guided biopsy is preferred.
- Imaging: MRI of primary site (best for soft tissue); CT chest/abdomen/pelvis for staging
- IHC: MDM2 and CDK4 nuclear positivity confirms WDL/DDLPS
- FISH/cytogenetics: MDM2 amplification (FISH) can distinguish WDL from atypical lipoma in difficult cases
Treatment
Surgery (Primary Treatment for All Subtypes)
Extremity liposarcoma:
- Limb-sparing resection with negative surgical margins is the goal
- ALT/WDL: more limited resection acceptable (low metastatic risk); local recurrence occurs on average 6-8 years after resection
- Higher-grade subtypes: wide local excision + adjuvant radiation
Retroperitoneal liposarcoma:
- Gross complete resection is the principal goal - incomplete resection increases mortality
- Compartmental resection (including potentially uninvolved adjacent organs) vs. standard resection - controversial
- Organs resected in >50% of compartmental resections: spleen, pancreas, diaphragm, adrenal gland, kidney
- Recurrence monitoring: if recurrent tumor growth < 0.9 cm/month - resect; if > 0.9 cm/month - poor outcome, consider systemic therapy
Radiation Therapy
- Neoadjuvant radiation preferred for extremity high-grade tumors (reduces local recurrence)
- Used perioperatively for WDL/ALT extremity tumors as well
- Myxoid liposarcoma is particularly radiosensitive
Chemotherapy
| Drug/Regimen | Indication |
|---|---|
| Doxorubicin (anthracycline) | First-line for high-grade, metastatic or unresectable; also adjuvant |
| Ifosfamide | Often combined with doxorubicin |
| Trabectedin (1.3 mg/m² IV over 24h q3w) | Approved for unresectable/metastatic liposarcoma or leiomyosarcoma after anthracycline failure; especially effective in myxoid subtype; pretreat with dexamethasone to reduce hepatotoxicity |
| Eribulin | FDA-approved; phase III showed improved OS vs. dacarbazine (15.6 vs. 8.4 months) - now standard in palliative setting for liposarcoma |
| Dacarbazine | Alternative palliative option |
Prognosis
| Subtype | 5-Year Survival | Key Points |
|---|---|---|
| ALT (extremity) | Excellent (near 100% DSS) | No metastatic potential |
| WDL (retroperitoneum) | Good, but frequent local recurrence | Significant morbidity from recurrence |
| DDLPS | Intermediate | Local recurrence + metastatic risk |
| Myxoid LPS (pure) | ~87% (10-year DSS) | Chemo/radiosensitive |
| Round cell LPS | Worse - 21% metastatic rate | High-grade variant of myxoid |
| Pleomorphic LPS | Poor | Aggressive, frequent mets |
| High-grade tumors overall | ~60% 5-year survival | - |
Poor prognostic indicators:
- High grade
- Large size (> 5 cm)
- Proximal or deep location
- Presence of metastases
- Positive surgical margins
Key Molecular Summary Table
| Subtype | Chromosomal Change | Genes Affected |
|---|---|---|
| WDL / DDLPS | Amplification 12q13-15 (ring/marker chromosomes) | MDM2, CDK4 (also HMGA2, CDK4, FRS2, YEATS4) |
| Myxoid / Round cell | t(12;16)(q13;p11) or t(12;22)(q13;q12) | FUS::DDIT3 or EWSR1::DDIT3 |
| Pleomorphic | Complex karyotype | No consistent mutation |
Sources: Robbins & Cotran Pathologic Basis of Disease | Sabiston Textbook of Surgery | Campbell's Operative Orthopaedics (15th Ed., 2026) | Grainger & Allison's Diagnostic Radiology | Fitzpatrick's Dermatology | Goodman & Gilman's Pharmacological Basis of Therapeutics | Quick Compendium of Clinical Pathology | Frontiers in Oncology (2024)
This is a shared conversation. Sign in to Orris to start your own chat.