Enteric fever
Reading File
Finding Sources
Searching PubMed
"enteric fever" OR "typhoid fever" management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive review of enteric fever drawn primarily from Harrison's Principles of Internal Medicine 22E (2025) and Goldman-Cecil Medicine, supplemented by the Red Book 2021.
Enteric Fever
Definition
Enteric fever is a systemic illness caused by Salmonella enterica serovar Typhi (typhoid fever) or serovars Paratyphi A, B, and C (paratyphoid fever). The term "enteric fever" was proposed in 1869 to distinguish the illness from typhus, based on its pathological association with enlarged Peyer's patches and mesenteric lymph nodes. The two names - typhoid fever and enteric fever - are used interchangeably today. - Harrison's Principles of Internal Medicine 22E, p. 1359
Epidemiology
- An estimated 9.2-21 million cases of typhoid fever and 5 million cases of paratyphoid fever occur annually, with 110,000-280,000 deaths per year.
- Highest incidence: Indian subcontinent (Pakistan, Bangladesh, Nepal, India), Eastern Mediterranean, and sub-Saharan Africa. Some urban areas in these regions exceed 1,000 cases per 100,000 children.
- S. Typhi and S. Paratyphi have no animal reservoir - humans are the only host. Transmission is fecal-oral, via contaminated food or water, or from asymptomatic chronic carriers.
- Risk factors: contaminated drinking water or ice, street food, raw produce fertilized with sewage, ill household contacts, lack of hand hygiene, and prior H. pylori infection (linked to reduced gastric acidity).
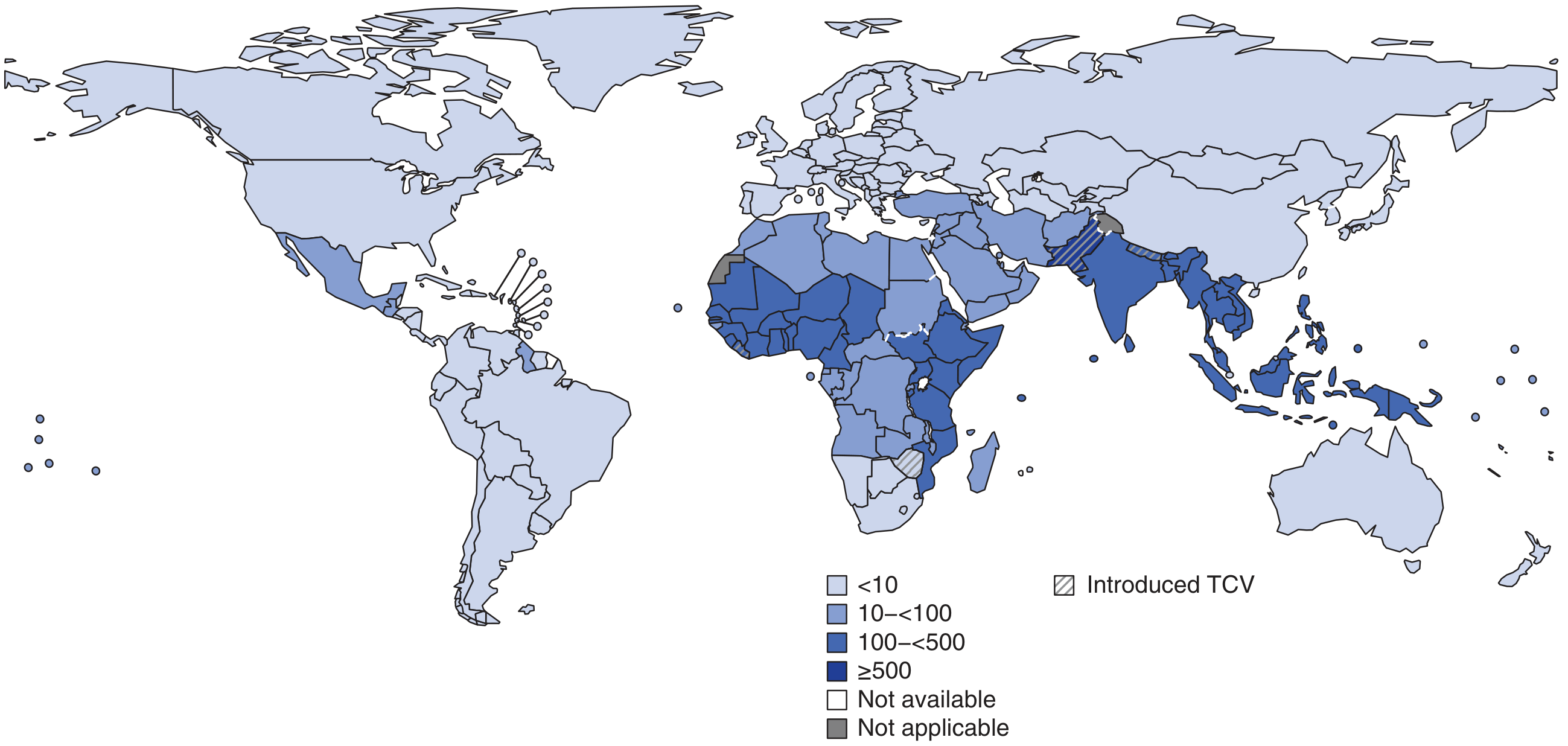
South Asia and sub-Saharan Africa carry the highest burden (≥500 cases per 100,000), with typhoid conjugate vaccines (TCV) being introduced in some of the highest-burden countries.
Pathogenesis
After ingestion of a sufficient inoculum (~10³-10⁹ organisms), S. Typhi invades the small intestinal mucosa via M cells overlying Peyer's patches. It is then phagocytosed by macrophages and transported via lymphatics into the bloodstream - a primary bacteremia. The bacteria seed reticuloendothelial organs (liver, spleen, bone marrow, lymph nodes) where they multiply within macrophages. A secondary bacteremia follows, coinciding with clinical onset of fever. The organism then re-enters the gut via biliary secretion, causing necrosis of Peyer's patches - the pathological basis for intestinal hemorrhage and perforation. - Harrison's 22E
Clinical Course
Week 1
- Incubation period: 5-21 days (mean 10-14 days), depending on inoculum size and host immunity.
- Fever: Prolonged, rising in a stepwise fashion to 38.8°-40.5°C (101.8°-104.9°F). Present in >75% at initial evaluation.
- Symptoms: Headache (80%), anorexia (55%), chills (35-45%), cough (30%), abdominal pain (30-40%), nausea (18-24%), vomiting (18%), diarrhea (22-28%) or constipation (13-16%).
- Signs: Coated tongue (51-56%), relative bradycardia (pulse-temperature dissociation, up to 50% of cases), mild hepatosplenomegaly.
Week 2
- Rose spots: Faint, salmon-colored, 1-4 mm blanching maculopapules on the lower chest and abdomen. Appear in ~30% of light-skinned patients, rarely visible in dark-skinned patients. Salmonella can be cultured from biopsy of these lesions.
- Hepatosplenomegaly in ~50% of patients.
- Abdominal distension and tenderness become more pronounced.
- Neuropsychiatric manifestations: apathy, confusion, delirium ("typhoid state"), even psychosis.
- Leukopenia and neutropenia in ~20%; abnormal liver function tests are common.
Week 3-4
- Risk of major complications (intestinal perforation/hemorrhage) due to Peyer's patch necrosis: ~5% of untreated patients.
- Illness resolves by end of week 4 in untreated cases.
- Relapse occurs in up to 17% within 4 weeks, especially in immunocompromised patients; relapse is milder than the initial episode. - Goldman-Cecil Medicine
Complications
| System | Complication |
|---|---|
| Gastrointestinal | Intestinal perforation, hemorrhage (2nd-3rd week) |
| Hepatobiliary | Hepatitis, cholecystitis, hepatic abscess |
| Neurological | Encephalopathy, meningitis (rare), Guillain-Barré |
| Cardiac | Infective endocarditis, myocarditis |
| Pulmonary | Pneumonia |
| Other | Pancreatitis, orchitis, splenic abscess |
Rarely, patients may develop pancreatitis, cholecystitis, endocarditis, meningitis, or focal infection at virtually any site. - Goldman-Cecil Medicine
Diagnosis
Gold Standard: Culture
- Blood culture: Positive in 60-80% in the first week (bacteria are in the bloodstream during primary bacteremia). Sensitivity falls with antibiotic use.
- Bone marrow culture: Most sensitive (~90%), especially after antibiotic use; remains positive longer.
- Stool culture: Positive from 2nd week onward as bacteria re-enter the gut via bile.
- Rose spot culture: Positive from biopsies of rose spot lesions.
Serology
- Widal test: Detects agglutinating antibodies against O (somatic) and H (flagellar) antigens. High false-positive and false-negative rates limit its usefulness, especially in endemic areas. Not recommended as a standalone diagnostic.
Molecular
- PCR-based methods are increasingly used but not yet standardized for routine clinical use.
Other labs
- Leukopenia/neutropenia (~20%), mild thrombocytopenia, elevated transaminases are common.
Antibiotic Treatment
The choice of antibiotic is dominated by resistance patterns, which have evolved dramatically.
Resistance landscape
- MDR strains (resistant to chloramphenicol, ampicillin, TMP-SMX): emerged in the 1980s-1990s.
- Decreased susceptibility to ciprofloxacin (DSC) / fluoroquinolone resistance: emerged from the Indian subcontinent in the 1990s-2000s; clone H58 is the dominant strain. In the US in 2015, 66% of isolates were DSC.
- XDR (extensively drug-resistant) S. Typhi: Emerged in Pakistan in 2016. Resistant to chloramphenicol, ampicillin, TMP-SMX, fluoroquinolones, AND third-generation cephalosporins (ESBL-mediated). Only susceptible to azithromycin and carbapenems. Over 5,000 XDR cases reported from Pakistan; imported cases documented in the US and UK. - Red Book 2021, p. 1023; Harrison's 22E
- Azithromycin resistance has now emerged in multiple countries where it is used as first-line treatment.
Treatment recommendations
| Susceptibility | Drug of Choice | Alternative |
|---|---|---|
| Fully susceptible | Ciprofloxacin 500 mg PO BID × 5-7 d OR amoxicillin/chloramphenicol | - |
| MDR (resistant to chloramphenicol, ampicillin, TMP-SMX) | Azithromycin OR ceftriaxone 2g IV OD × 7-14 d | - |
| DSC / fluoroquinolone-resistant | Azithromycin 1g PO OD × 5-7 d OR ceftriaxone 2g IV × 7-14 d | High-dose ciprofloxacin (unreliable) |
| XDR (Pakistan-associated) | Azithromycin (oral, mild disease) OR meropenem (IV, severe disease) | Tigecycline (limited data) |
Key principle: Most typhoid fever diagnosed in the US is fluoroquinolone-nonsusceptible, so empiric fluoroquinolones should be avoided, especially in travelers returning from South Asia. Empiric therapy should use parenteral ceftriaxone or azithromycin while awaiting susceptibility results. - Red Book 2021
Duration: At least 7-10 days for uncomplicated disease. If amoxicillin or TMP-SMX is used based on susceptibility, a 14-day course is preferred.
Severe disease (encephalopathy, shock)
- High-dose dexamethasone: 3 mg/kg IV initially, then 1 mg/kg IV every 6 hours for 48 hours. Shown to reduce mortality in severely ill (delirious, comatose, or shocked) patients. - Red Book 2021, p. 1024
Chronic carrier state
- Defined as stool shedding >1 year (often associated with cholelithiasis/cholecystitis).
- Treat with ciprofloxacin or norfloxacin for 4 weeks (concentrates in bile).
- Cholecystectomy + antibiotics may be needed if medical therapy fails.
Prevention
Vaccines
Two licensed vaccines are available:
| Vaccine | Type | Route | Age | Efficacy | Duration |
|---|---|---|---|---|---|
| Ty21a (Vivotif) | Live attenuated oral | Oral (4 capsules every other day) | ≥6 years | ~67% | 5 years |
| Vi-CPS (Typhim Vi) | Polysaccharide | IM, single dose | ≥2 years | ~64% | 2 years |
| Vi-TT (Typbar-TCV) | Conjugate (TCV) | IM, single dose | ≥6 months | ~82% | Longer (ongoing) |
The typhoid conjugate vaccine (TCV) has now been introduced in many high-burden countries (shown with hatched areas on the map above) and is recommended by WHO for children as young as 6 months in endemic settings. A 2025 meta-analysis (PMID 41125003) confirmed real-world effectiveness of TCV in children and adolescents.
- Neither vaccine protects against S. Paratyphi - this remains an important gap.
- Vaccination is recommended for travelers to endemic regions, especially those visiting friends/family or staying for prolonged periods.
General measures
- Safe water and food handling
- Hand hygiene
- Proper sewage treatment
- Identification and treatment of chronic carriers (especially food handlers)
Special Notes
- Weil-Felix reaction: Negative (distinguishes from typhus).
- Faget's sign (sphygmothermal dissociation / relative bradycardia): Pulse rate lower than expected for the degree of fever - a classic but non-specific sign.
- "Typhoid state": Second-week delirium, apathy, and high fever.
- In sickle cell disease: Salmonella is the most common cause of osteomyelitis.
- Pregnancy: Associated with miscarriage, preterm delivery, and vertical transmission; use ceftriaxone (fluoroquinolones contraindicated).
Sources:
- Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill), Ch. 171
- Goldman-Cecil Medicine (International Edition), Salmonella chapter
- Red Book 2021: Report of the Committee on Infectious Diseases, AAP
This is a shared conversation. Sign in to Orris to start your own chat.