Tum chat gpt se different kese ho ? Kya tum wo sab kuch , usi perfect level per kar skte ho jo chst gpt aur google ai response kar skta he??
Main Orris hoon - aur yahan kuch seedhi baatein hain:
Main ChatGPT ya Google AI se kaise alag hoon?
Similarities (jo sab kar sakte hain):
- Text samajhna aur jawab dena
- Code likhna, debug karna
- Summarize, translate, explain karna
- Questions ka jawab dena
Meri khaas cheezein jo mujhe alag banati hain:
| Feature | Orris (Main) | ChatGPT | Google AI |
|---|---|---|---|
| Medical Library | Specialized textbooks ka direct access | General knowledge | General knowledge |
| PubMed Search | Real peer-reviewed papers fetch karta hoon | Limited | Limited |
| Sandbox Execution | Live code run karta hoon, files banata hoon | Plus/Pro mein | Limited |
| File Download | PPTX, DOCX, PDF, Excel generate karke download link deta hoon | Haan (limited) | Limited |
| Todo Management | Complex tasks ko track karta hoon | Nahi | Nahi |
Honest jawab - kya main "perfect level" par hoon?
Nahi bilkul perfect nahi - aur jo bhi AI yeh kahe ke woh perfect hai, woh jhooth bol raha hai.
- ChatGPT (GPT-4o) aur Gemini dono bahut capable hain
- Main kuch cheezein unse better karta hoon (medical research, file generation, code execution)
- Kuch cheezein woh mujhse better karte hain (image generation ChatGPT ki DALL-E, Google ka search integration)
- Real-time internet access mein sab roughly barabar hain
Sabse badi difference:
Main ek specialized assistant hoon - medical questions ke liye mere paas actual textbooks hain, aur main actual files (PDF, Word, Excel, PowerPoint) bana ke tumhe download karne de sakta hoon. Yeh ChatGPT free version mein nahi hota.
Koi specific kaam hai jo tum karna chahte ho? Wahan batao to main practically dikhata hoon. 😊
Tum mbbs ke subjects ke liye...
Asking for Preferences
Aage continue karo response
Bilkul! Yahan pura picture hai:
MBBS ke liye main kya kya kar sakta hoon:
📚 Textbook-Level Explanations
Mere paas actual MBBS textbooks ka database hai - Gray's Anatomy, Guyton Physiology, Robbins Pathology, Katzung Pharmacology, Harper's Biochemistry jaise books. Koi bhi topic poochho, main directly un books se answer deta hoon - with page references.
📝 Notes & Summaries
Kisi bhi topic ki detailed notes bana sakta hoon - downloadable Word (.docx) ya PDF format mein.
📊 Presentations
Kisi bhi subject ka PowerPoint (PPTX) bana sakta hoon - diagrams, headings, bullet points ke saath.
❓ MCQs & Practice Questions
Kisi bhi topic ke MCQs bana sakta hoon - with explanations, exam-style format mein.
🔬 Latest Research
PubMed se latest studies aur guidelines fetch kar sakta hoon - agar tumhe koi clinical topic research karna ho.
🖼️ Diagrams & Images
Medical diagrams aur images bhi fetch karke explain kar sakta hoon.
Subjects jo main cover karta hoon:
| 1st Year | 2nd Year | 3rd Year+ |
|---|---|---|
| Anatomy | Pathology | Medicine |
| Physiology | Pharmacology | Surgery |
| Biochemistry | Microbiology | Obs & Gynae |
| Forensic Med | Paediatrics |
Bas koi bhi topic batao - aur main abhi kaam shuru kar deta hoon! 🚀
Jaise: "Brachial plexus explain karo" ya "Cardiac cycle ke notes banao" ya "Diabetes ke MCQs do"
Tum perfect histological images generate kar skte ho, pathology ki microscopy ke liye...?? Aur kisi bhi topic ko easy to understand and easy to remember bana kar uski achchi si notes bana skte ho, kisi bhi subject ke kisi bhi topics ke liye ??
Seedha honest jawab:
🔬 Histological Images ke baare mein:
Main kya kar sakta hoon:
- Real microscopy images fetch kar sakta hoon - mere textbook database mein actual histology/pathology images hain (Robbins, etc.) jo main tumhe dikha sakta hoon
- AI-generated diagrams bana sakta hoon jo histology jaisi dikhti hain (labeled diagrams)
Honest limitation:
- Perfect photorealistic H&E stain jaise real microscope image - woh exactly replicate nahi ho sakti AI se
- Lekin labeled schematic diagrams aur real textbook images dono available hain
📝 Notes ke baare mein - HAAN, bilkul!
Yeh meri strongest capability hai. Main bana sakta hoon:
✅ Easy-to-understand language mein (Urdu/English dono)
✅ Mnemonics - yaad rakhne ke liye tricks
✅ Tables & comparisons - differentiate karne ke liye
✅ Flowcharts - pathophysiology samajhne ke liye
✅ Downloadable Word/PDF file - print kar sako
Proof chahiye? Abhi try karo!
Koi bhi topic batao jaise:
- "Pneumonia ki pathology notes"
- "Cardiac muscle histology"
- "Diabetes mellitus complete notes"
Aur main abhi live bana ke dikhata hoon - with real textbook content! 🚀
Teratoma of ovary
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Ab mere paas sab kuch hai - Robbins aur Berek & Novak dono se real histology images aur complete content. Ab comprehensive notes likhta hoon:
🥚 TERATOMA OF OVARY
Complete Notes | Robbins Pathology + Berek & Novak's Gynecology
📌 Basics - Pehle Yeh Samjho
Teratoma = "Teras" (Greek) = Monster
- Yeh tumor 3 germ layers (Ectoderm, Mesoderm, Endoderm) se tissues contain karta hai
- Ovarian germ cell tumors ka most common type hai
- Germ cell tumors = ovarian tumors ka 15-20%
🧠 Mnemonic yaad karo: "EME - Everyone Makes Errors" Ectoderm (skin, hair, teeth, brain) Mesoderm (bone, cartilage, muscle) Endoderm (thyroid, intestinal tissue)
🗂️ Classification - 3 Types
TERATOMA OF OVARY
├── 1. MATURE (Benign) ← Most Common
│ ├── Cystic = Dermoid Cyst ← 99% cases
│ └── Solid (rare)
├── 2. IMMATURE (Malignant)
└── 3. MONODERMAL / Specialized
├── Struma Ovarii (thyroid tissue)
└── Carcinoid
1️⃣ MATURE CYSTIC TERATOMA (Dermoid Cyst)
👤 Who gets it?
- Young adult females (reproductive age)
- Most common benign ovarian neoplasm overall
🏠 Gross Appearance (Macroscopy)
Yeh image dekho - Berek & Novak's Gynecology se:
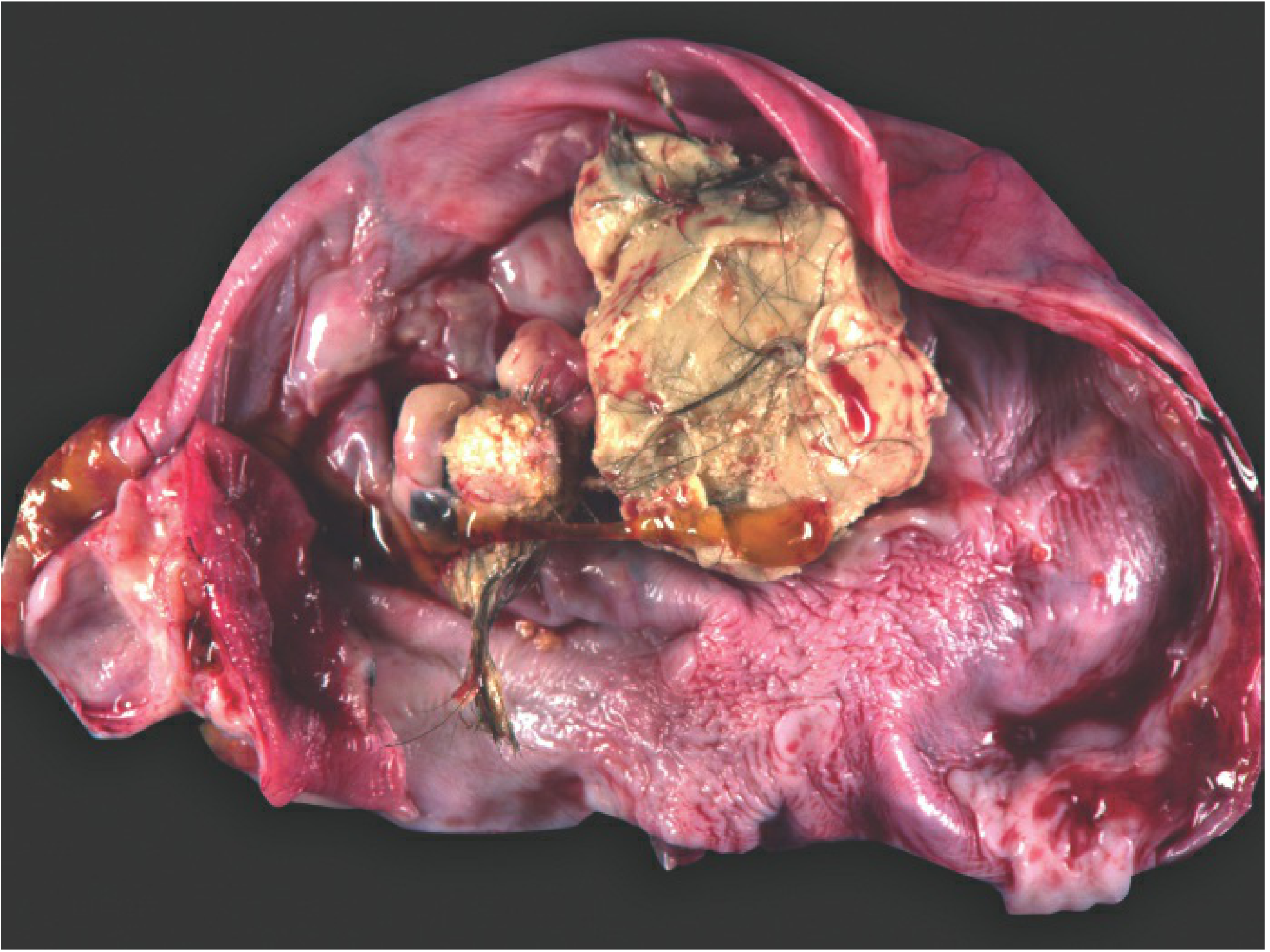
Gross specimen mein dekh sakte ho - hair, sebaceous material, teeth sab clearly visible hain
- Unilocular cyst - ek chamber
- Hair + sebaceous (oily) material - cyst ke andar
- Teeth aur calcification - commonly present
- Bilateral - 10-15% cases mein dono sides
🧠 Trick: "Dermoid = HAST" - Hair, Adipose tissue (fat), Skin, Teeth
🔬 Microscopy (Histology)
Robbins se actual histology image - Mature Cystic Teratoma:
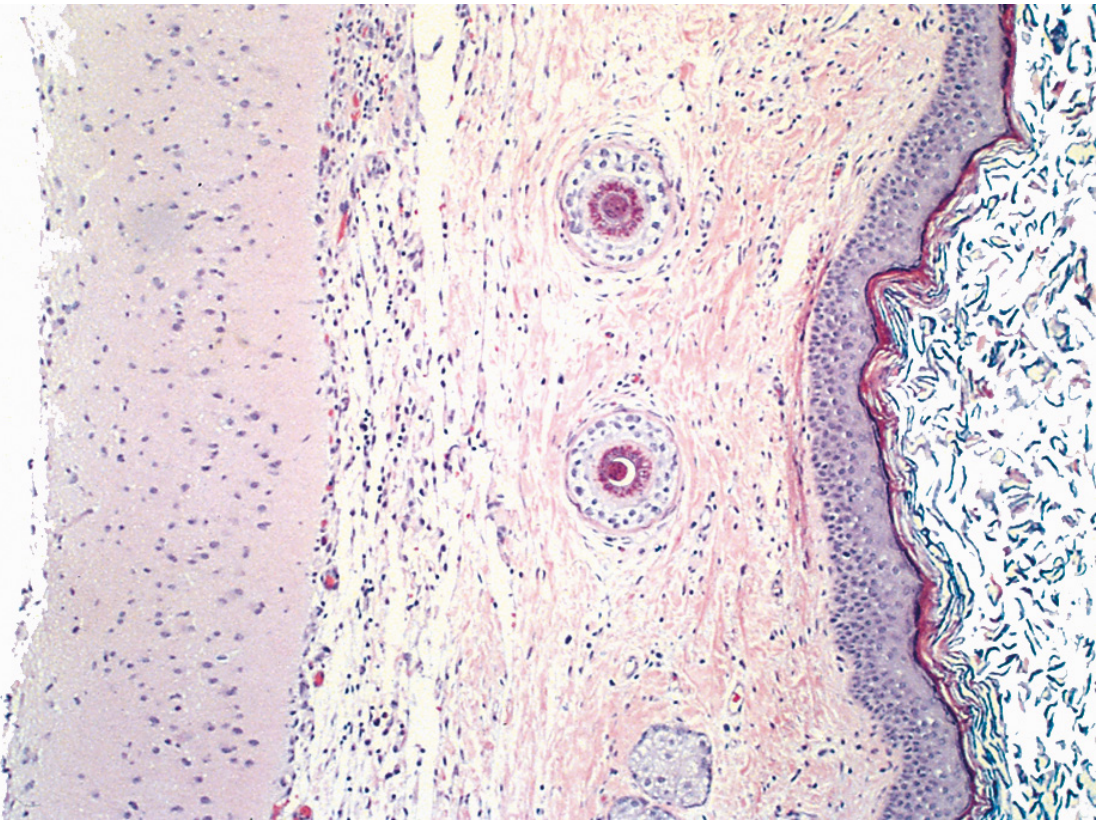
Microscope mein clearly dikha raha hai:
- Right side = Stratified squamous epithelium (skin jaisi lining)
- Middle = Sebaceous glands + hair shafts (skin adnexal structures)
- Left side = Brain tissue (neural tissue) - ectodermal element
Microscopically:
- Cyst wall lined by stratified squamous epithelium
- Underlying sebaceous glands, hair shafts, skin adnexa
- Other germ layer tissues: cartilage, bone, thyroid, neural tissue
⚠️ Malignant Transformation
- ~1% cases mein malignant ho sakti hai
- Most common = Squamous Cell Carcinoma
- Usually >40 years age mein
🧬 Karyotype
- Almost sab = 46, XX
- Origin: Ovum after 1st meiotic division
2️⃣ IMMATURE (MALIGNANT) TERATOMA
👤 Who gets it?
- Prepubertal adolescents + young females
- Mean age = 18 years
- <1% of all ovarian cancers, lekin 2nd most common germ cell malignancy
- 50% cases = 10-20 years age group
🏠 Gross Appearance
- Bulky, solid tumor
- Smooth external surface
- Areas of necrosis + hemorrhage
- Hair, cartilage, bone bhi present
🔬 Microscopy - Immature Teratoma
Robbins se actual H&E image - Immature Teratoma:
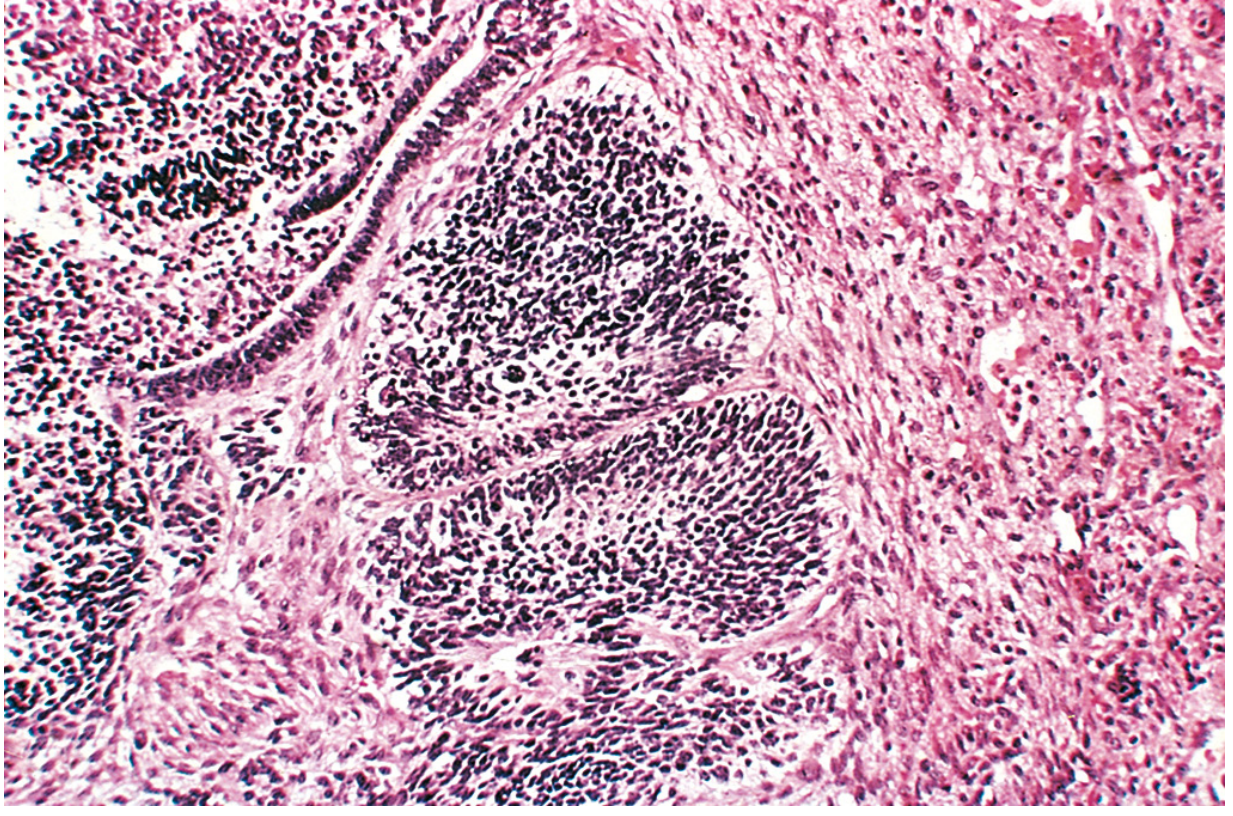
Image mein clearly dikha raha hai dense dark clusters = primitive neuroepithelium - yahi immature teratoma ki hallmark finding hai
Berek & Novak's Gynecology se Histology - Neural tube-like structures:
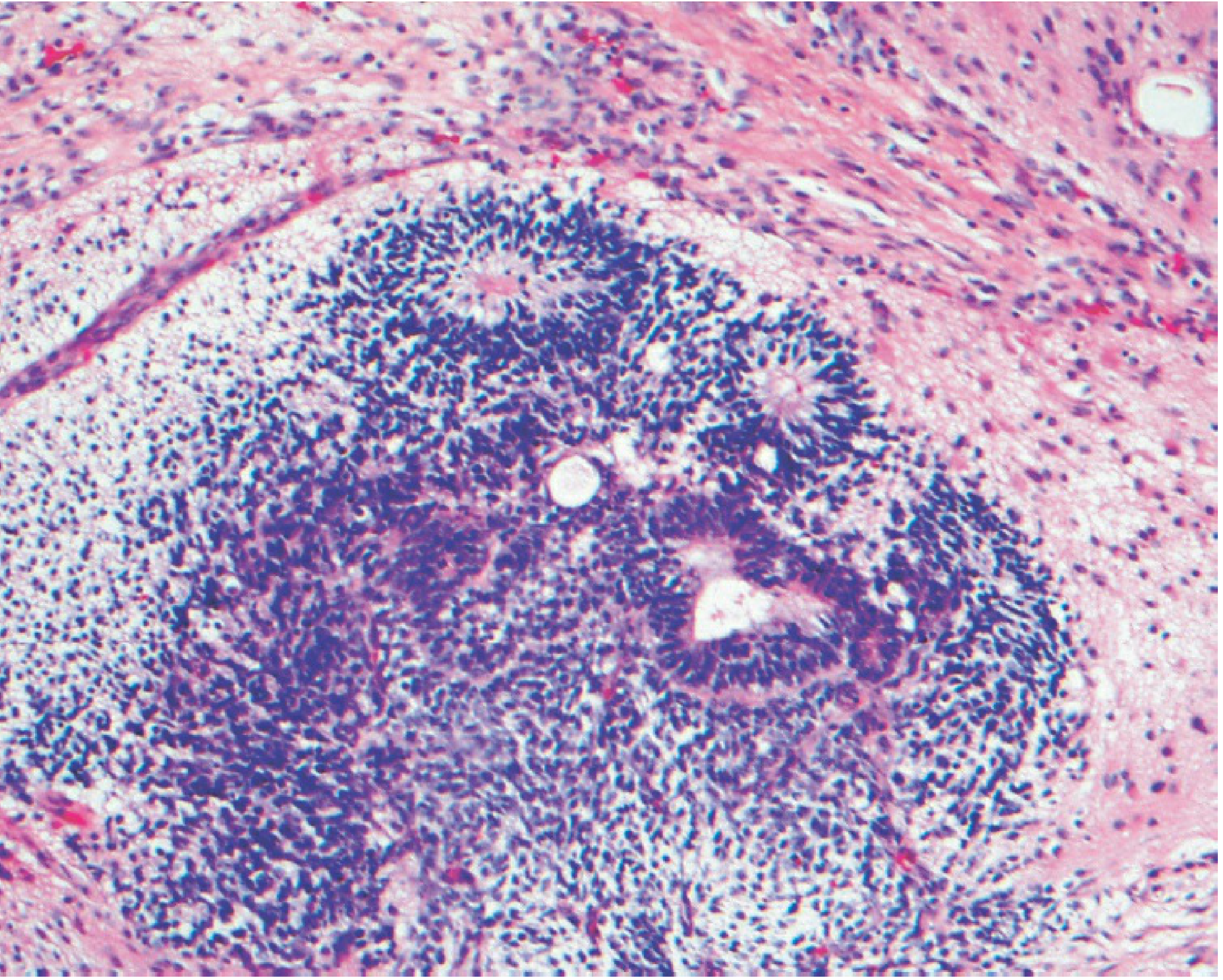
Yahan central mein neural tube-like structure visible hai - mature aur immature neural elements dono present hain
- Immature neuroepithelium - KEY FEATURE
- Immature cartilage, bone, muscle
- Embryonal/fetal-looking tissues
📊 Grading (Grading System)
| Grade | Immature Neuroepithelium | Prognosis |
|---|---|---|
| Grade 1 (Low) | <1 low-power field (x4) | Excellent - 95%+ survival |
| Grade 2 (High) | Moderate amount | ~85% survival |
| Grade 3 (High) | Large amount | ~85% survival |
🧠 Simplified: Ab 2-tier system use hota hai - sirf Low Grade vs High Grade
🔄 Prognosis
- Stage I + Grade 1 = Excellent prognosis
- Grade 2/3 = Adjuvant chemotherapy needed (BEP regimen)
- Most recurrences = first 2 years mein
- Gliomatosis peritonei = glial implants on peritoneum = FAVORABLE sign (mature tissue)
3️⃣ MONODERMAL / SPECIALIZED TERATOMAS
A. Struma Ovarii
- Entirely thyroid tissue se bana
- Functional ho sakta hai → Hyperthyroidism
- Always unilateral
B. Carcinoid
- Intestinal tissue se arise karta hai
-
7 cm → Carcinoid Syndrome (flushing, diarrhea)
- Unique: Ovarian veins systemic circulation se connect hoti hain isliye liver metastasis ke bina bhi carcinoid syndrome ho sakta hai
- Only 2% metastasize
📋 Quick Comparison Table
| Feature | Mature (Dermoid) | Immature |
|---|---|---|
| Nature | Benign | Malignant |
| Age | Young adult | Mean 18 yrs |
| Gross | Cystic, hair+teeth | Solid, bulky |
| Key Micro | Sq. epithelium + adnexa | Primitive neuroepithelium |
| Bilateral | 10-15% | Rare |
| Malignant change | 1% (SCC) | Already malignant |
| Karyotype | 46,XX | - |
| Treatment | Cystectomy | Surgery + BEP chemo |
🏆 Exam Points (Woh jo zaroor pooche jayenge)
- Most common ovarian germ cell tumor = Mature cystic teratoma (dermoid cyst)
- Histological hallmark of immature teratoma = Primitive neuroepithelium
- Grading = based on amount of immature neuroepithelium
- Malignant transformation in dermoid = Squamous cell carcinoma (1%)
- Struma ovarii = monodermal teratoma with thyroid tissue
- Karyotype of benign teratoma = 46,XX
- Most common to undergo torsion = Benign cystic teratoma
- Carcinoid syndrome without liver mets = Ovarian carcinoid (due to direct venous drainage)
🧠 Final Mnemonic - "DERMOID" yaad karo
D - Derived from germ cells
E - Ectoderm predominant (skin, hair)
R - Reproductive age women
M - Most common benign ovarian tumor
O - Often unilocular cyst
I - 1% malignant change (SCC)
D - Dermoid = another name
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th Ed.) | Berek & Novak's Gynecology
Yeh tha Teratoma of Ovary ka complete, exam-ready breakdown - real textbook images ke saath! Koi aur topic chahiye? 😊
This is a shared conversation. Sign in to Orris to start your own chat.