Potts TB for 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full 10-mark answer.
Pott's Disease (Tuberculous Spondylitis)
1. Definition and Historical Background
Pott's disease is tuberculous osteomyelitis of the spine, first described by Percival Pott in 1779 in a patient presenting with paraplegia secondary to spinal tuberculosis. It is one of the oldest documented human infections - evidence has been found in Egyptian and Peruvian mummies over 5,000 years old. It represents the most severe form of infective spondylitis and the most common form of skeletal tuberculosis, accounting for 50% of all skeletal TB cases.
- Rheumatology, 2-Volume Set (Elsevier 2022)
- Miller's Review of Orthopaedics 9th Edition
2. Etiopathogenesis
- Caused by Mycobacterium tuberculosis (occasionally M. bovis)
- Reaches the spine via haematogenous spread from a primary pulmonary focus, establishing a latent focus in the richly vascularised metaphysis of the vertebral body
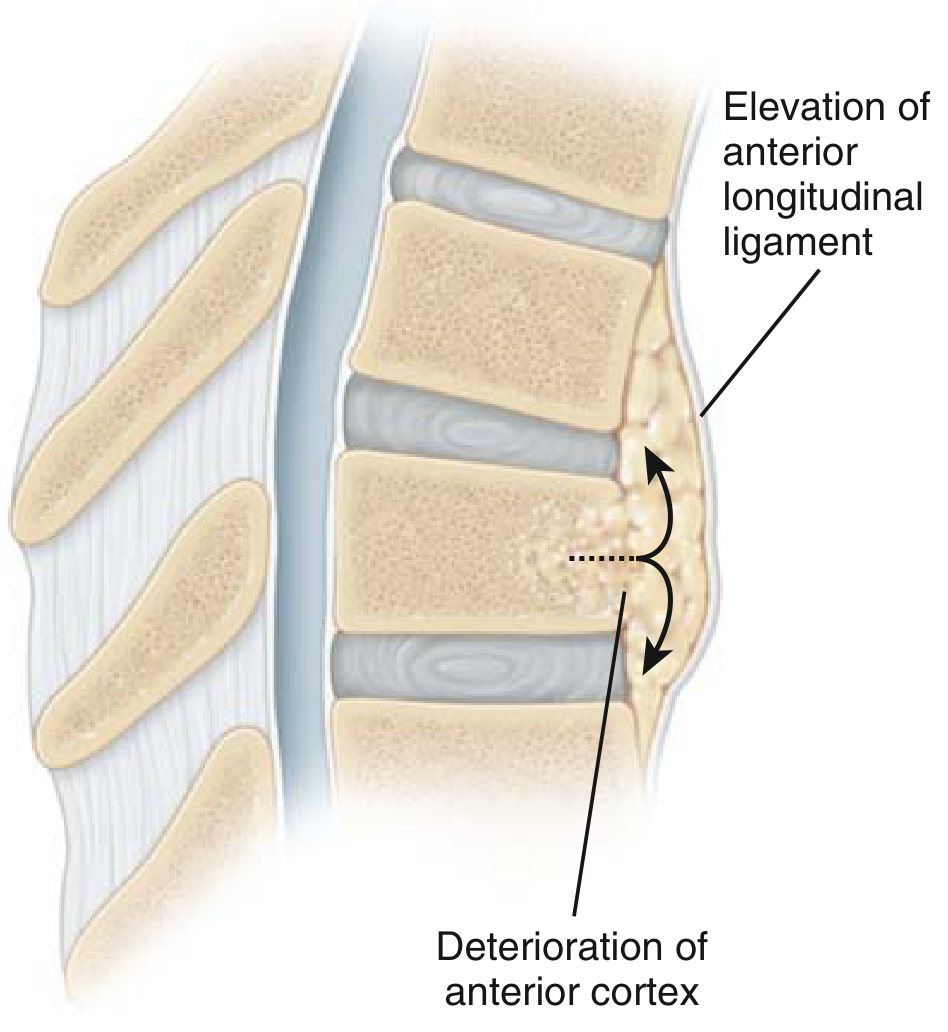
- The infection originates in the anterior aspect of the vertebral body and spreads under the anterior longitudinal ligament (ALL) to involve adjacent vertebrae - a hallmark feature distinguishing it from pyogenic infection
- An infectious endarteritis causes progressive bone necrosis and collapse
- The intervertebral disc is initially spared (avascular, resistant to TB), unlike pyogenic osteomyelitis where disc destruction is early
Pathogenesis diagram (spread under the anterior longitudinal ligament with deterioration of the anterior cortex):
3. Sites of Involvement
| Region | Frequency |
|---|---|
| Thoracic spine (T4-T8) | Most common (~50%) |
| Thoracolumbar junction | Second most common |
| Lumbar spine | Common |
| Cervical spine | Least common |
The thoracic and lumbar regions are predominantly affected. Contiguous multi-level involvement is typical; skip lesions occur in ~15% of cases.
4. Pathology
- Caseous necrosis with central caseating lesion surrounded by necrotic tissue and multinucleated giant cells (caseating granulomas)
- Progressive anterior column destruction leads to:
- Vertebral body collapse and wedging
- Gibbus deformity - sharp angular kyphosis (kyphosis + scoliosis)
- Cold abscess formation in 50% - pus tracks along fascial planes without signs of acute inflammation
- Abscess can track to present as:
- Psoas abscess (lumbar TB - track along psoas sheath to iliac fossa/groin/thigh)
- Paravertebral abscess (thoracic TB - may be seen on CXR as a 'fusiform' shadow)
- Retropharyngeal abscess (cervical TB)
5. Clinical Features
Onset is insidious, with symptoms often present for months before diagnosis.
Constitutional symptoms:
- Low-grade fever, night sweats, weight loss, malaise
- ESR and CRP are elevated (often more so than in pyogenic infection)
Local symptoms:
- Back pain (thoracic or lumbar) - most common presenting symptom
- Localized tenderness over the affected vertebrae
- Kyphosis / gibbus - late finding
Neurological complications (Pott's Paraplegia):
- Occurs in 4-30% of cases
- Spinal cord compression results from:
- Epidural abscess / caseous granulation tissue (most common cause - "early onset" paraplegia)
- Bony sequestra or vertebral collapse pressing on the cord
- Mechanical angulation due to gibbus deformity ("late onset" paraplegia)
- Rarely: tuberculous meningomyelitis (worst prognosis)
- Sensory deficits from cord/root compression often appear before spinal deformity is evident
6. Investigations
Laboratory:
- Elevated ESR and CRP
- Normal or mildly elevated WBC (unlike pyogenic infection)
- Possible normochromic normocytic anaemia
- TST (Mantoux) / IGRA - may be negative in ~20% (anergy)
Imaging:
Plain X-ray (late findings):
- Anterior vertebral body destruction with preservation of disc space - key distinguishing feature from pyogenic infection
- Subligamentous spread to multiple contiguous levels
- Vertebral collapse and kyphosis
- Paravertebral soft tissue shadow (abscess)
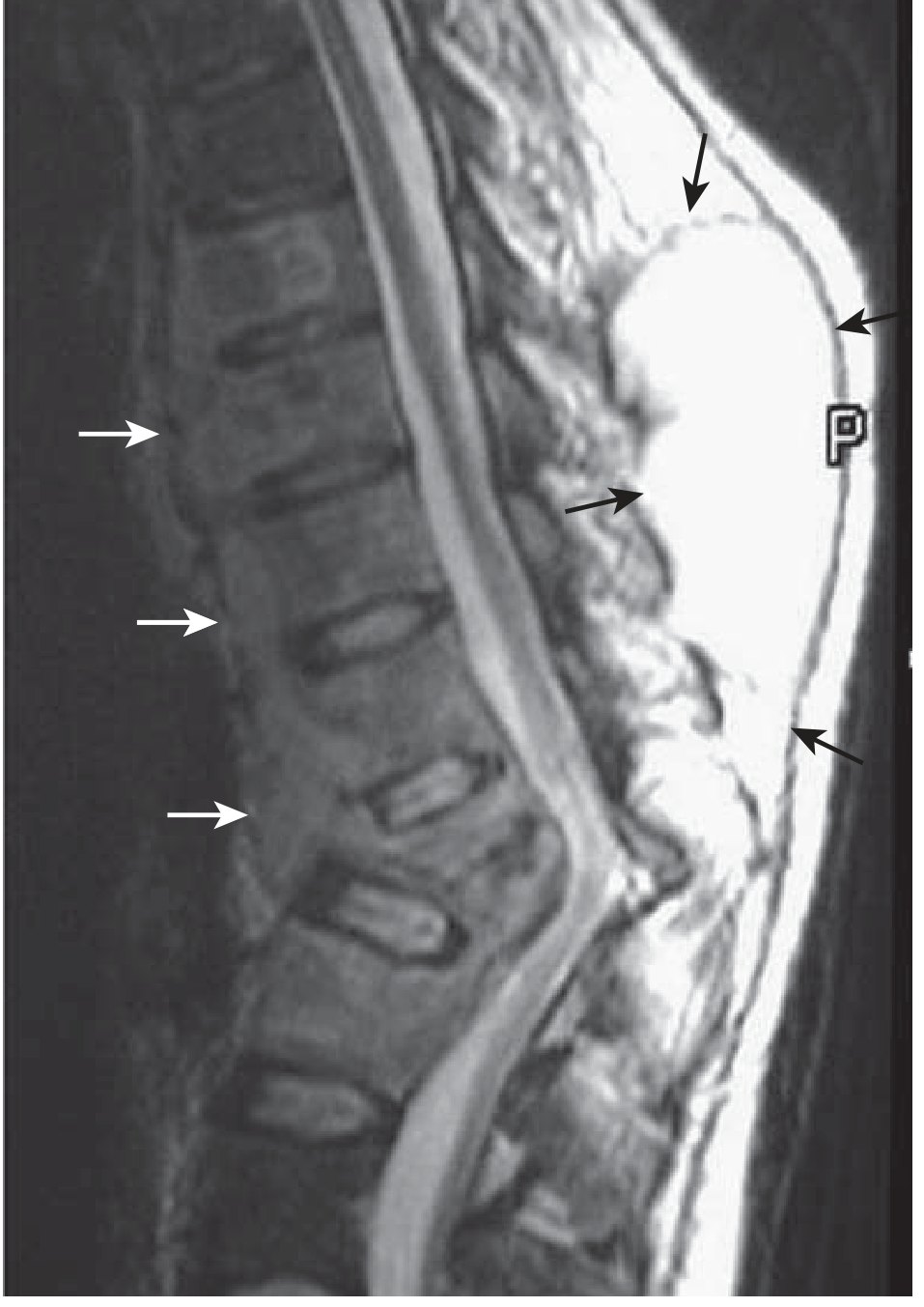
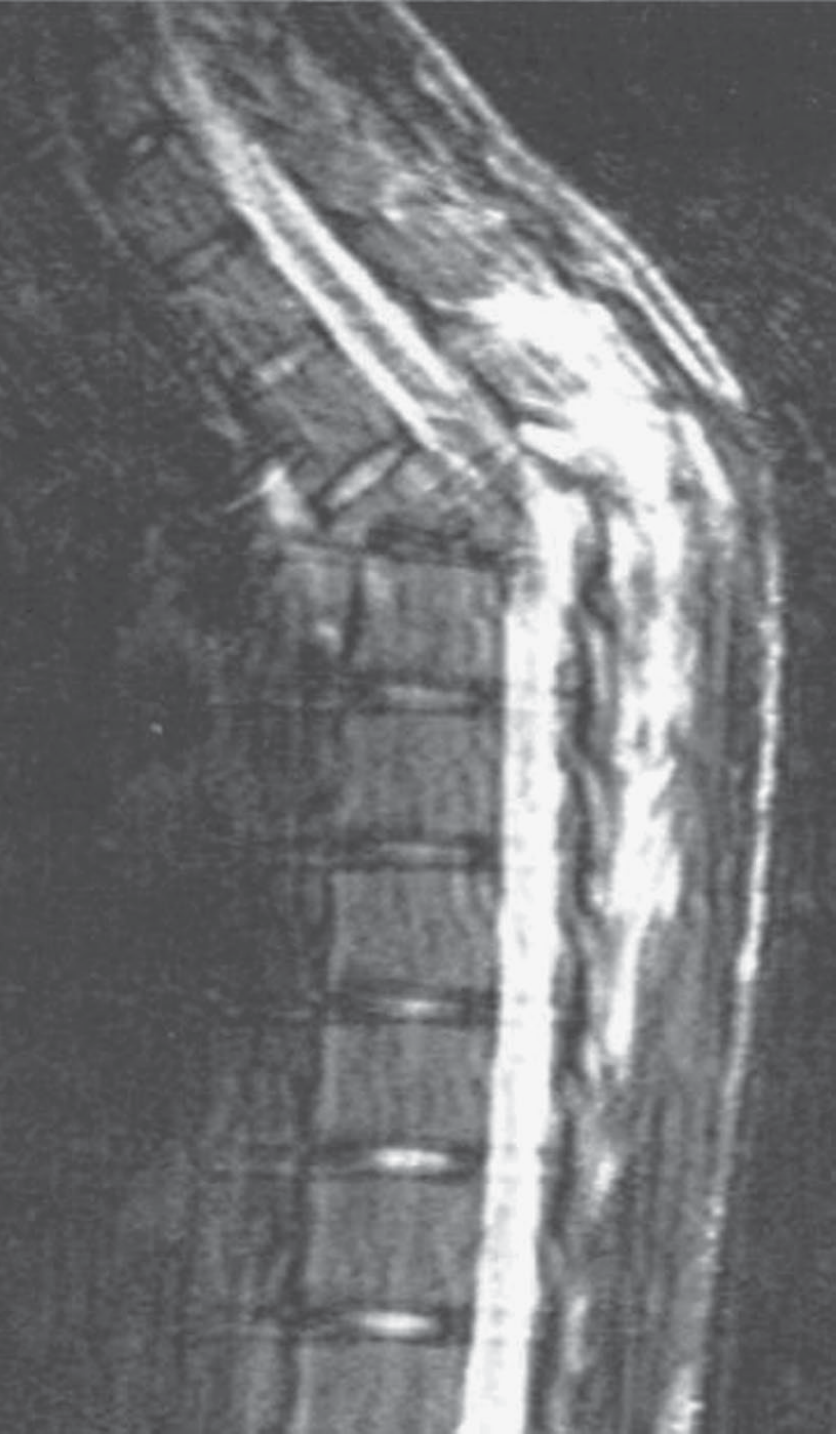
MRI - modality of choice:
- Shows vertebral body destruction, extent of cord compression, abscess
- T2: high signal in abscess and epidural collection
- Gadolinium (T1): enhances pus but not CSF - differentiates epidural abscess from CSF
- Relative sparing of disc on MRI is characteristic
Biopsy (CT-guided or open):
- Histology: caseating granulomas with Langhans giant cells
- Culture for M. tuberculosis (gold standard but takes weeks)
- About two-thirds of patients have abnormal chest radiographs
7. Treatment
A. Non-operative (Mainstay)
- Anti-tubercular therapy (ATT) is the cornerstone of management
- Standard regimen: HRZE (Isoniazid, Rifampicin, Pyrazinamide, Ethambutol) for 2 months intensive phase, then HR for 10 months continuation phase (total 12 months for spinal TB, longer than pulmonary TB)
- Triple or even quadruple therapy may be required
- External stabilisation (orthosis/brace) to protect the spine
- Results can be excellent with ATT alone + immobilisation in early disease
B. Surgical Indications
- Neurological deficit (cord compression, paraplegia)
- Spinal instability
- Progressive kyphosis
- Failure of medical management
- Advanced disease with caseation, fibrosis, and avascularity limiting antibiotic penetration
- Diagnostic uncertainty requiring biopsy
C. Surgical Procedure
- Hong Kong procedure (Hodgson & Stock, 1956): radical anterior debridement of infection followed by uninstrumented autogenous strut grafting - the classical/accepted surgical treatment
- Later evidence supports use of instrumented fixation when needed - advantages include less progressive kyphosis, earlier healing, and reduced sinus formation
- Adjuvant ATT starting 10 days before surgery is recommended (controversial but widely practiced)
- ATT after surgery is mandatory
8. Complications
| Complication | Notes |
|---|---|
| Pott's paraplegia | 4-30%; early (active disease) vs. late (healed, deformity-driven) |
| Gibbus deformity | Severe kyphosis; cosmetic + neurological risk |
| Sinus formation | Chronic discharging sinus from cold abscess |
| Psoas abscess | May point in groin or thigh |
| Meningomyelitis | Rare; poor prognosis |
| Aortic/visceral erosion | Very rare, from large paraspinal abscess |
Summary Table
| Feature | Pott's Disease (TB Spondylitis) |
|---|---|
| Organism | M. tuberculosis |
| Most common site | Thoracic > thoracolumbar > lumbar |
| Disc involvement | Spared early (key feature) |
| Spread | Subligamentous (under ALL) |
| Abscess type | Cold abscess |
| Deformity | Gibbus (kyphosis) |
| Neurological complication | Pott's paraplegia (4-30%) |
| Imaging of choice | MRI |
| Treatment | ATT (12 months) ± surgery |
| Classic surgery | Hong Kong procedure |
Sources: Rheumatology 2-Volume Set (Elsevier 2022), p. 1017 | Miller's Review of Orthopaedics 9th Ed., p. 787 | Campbell's Operative Orthopaedics 15th Ed. 2026 | Adams and Victor's Principles of Neurology 12th Ed., p. 1253
This is a shared conversation. Sign in to Orris to start your own chat.