Treatment for left ventricular hypertrophy
Reading File
Finding Sources
Searching PubMed
"left ventricular hypertrophy" AND treatment
Searching the Web
left ventricular hypertrophy treatment guidelines 2025
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have comprehensive textbook evidence. Let me synthesize a complete, structured answer.
Treatment of Left Ventricular Hypertrophy (LVH)
LVH is not a single disease — its treatment depends heavily on the underlying cause. The two major categories are:
- Hypertensive LVH (most common — pressure-overload concentric hypertrophy)
- Hypertrophic cardiomyopathy (HCM) (genetic sarcomere mutations)
I. LVH from Hypertension (Hypertensive Heart Disease)
Cornerstone: Blood Pressure Control
Effective antihypertensive treatment can delay and sometimes reverse LVH. Effective treatment reduces the risk of atrial fibrillation, heart failure, ventricular arrhythmias, sudden death, and stroke associated with LVH. — Goldman-Cecil Medicine, p. 757
Most antihypertensive classes reduce LVH to some degree when they lower blood pressure, but ARBs and ACE inhibitors are favored specifically for LVH regression. — Goldman-Cecil Medicine, p. 757
Drug Classes and LVH Regression (ranked by evidence)
| Drug Class | LVH Regression | Notes |
|---|---|---|
| ARBs (e.g., losartan) | ✅ Best evidence | LIFE trial: losartan superior to atenolol for LVH regression and stroke reduction in hypertensive patients with LVH |
| ACE inhibitors (e.g., enalapril, ramipril) | ✅ Excellent | Chronic treatment achieves sustained BP reduction + LVH regression + improved ventricular remodeling post-MI |
| Calcium channel blockers (dihydropyridines) | ✅ Good | Used in combination; added for angina or resistant BP |
| Thiazide/thiazide-like diuretics (chlorthalidone, indapamide) | ✅ Good | Often needed in combination; preferred in stroke prevention |
| β-blockers | ⚠️ Less effective for LVH regression | Still used for ischemic disease, heart failure with reduced EF, HCM |
| Aldosterone antagonists (spironolactone, eplerenone) | ✅ Useful | Particularly in HFrEF, resistant hypertension |
LIFE Trial evidence: In 9,193 hypertensive patients with LVH, losartan reduced stroke risk by 26% compared to atenolol and produced greater LVH regression, establishing ARB superiority over beta-blockade for this indication. — Brenner & Rector's The Kidney; Goodman & Gilman's
Non-pharmacological Measures
- Weight loss — reduces LV mass proportionally
- Sodium restriction — reduces volume load
- Aerobic exercise — physiologic hypertrophy (eccentric), not pathologic
- Alcohol reduction
- These lifestyle changes work synergistically with drug therapy
When EF is Reduced (Hypertensive Cardiomyopathy Progressing to HFrEF)
Guideline-directed medical therapy shifts to:
- β-blockers (carvedilol, metoprolol succinate, bisoprolol)
- Aldosterone antagonists (spironolactone, eplerenone)
- ARB/neprilysin inhibitors (sacubitril/valsartan — ARNI) — Goldman-Cecil Medicine, p. 757
II. Hypertrophic Cardiomyopathy (HCM)
HCM is genetic LVH (most commonly sarcomere mutations in MYH7, MYBPC3). Treatment targets symptom relief, obstruction reduction, and SCD prevention — not just BP.
Medical Management of LVOT Obstruction
First-line:
- β-blockers — slow heart rate, enhance diastolic filling, reduce contractility and gradient
- Verapamil (L-type CCB) — same mechanism; used if β-blockers not tolerated
- Disopyramide — negative inotrope; added for persistent exertional dyspnea/chest pain
Novel therapy:
- Mavacamten (FDA-approved cardiac myosin inhibitor) — highly effective for symptomatic obstructive HCM, including patients refractory to β-blockers; reduces sarcomere hypercontractility directly
- Aficamten — under investigation; same class — Harrison's Principles of Internal Medicine 22E, p. 2051
Diuretics: Used cautiously for fluid retention/venous congestion; avoid in obstruction due to hypovolemia risk.
Septal Reduction Therapy (Refractory Severe Symptoms ~5% of patients)
- Surgical septal myectomy — gold standard; removes obstructing septal myocardium; very low perioperative mortality at experienced centers; excellent long-term outcomes; resolves associated mitral regurgitation
- Alcohol septal ablation — percutaneous; controlled infarction of proximal septum; comparable gradient reduction; preferred in those who cannot tolerate surgery
Neither procedure has been shown to improve mortality — only symptoms. Both carry risk of complete heart block requiring permanent pacemaker.
Sudden Cardiac Death Prevention in HCM
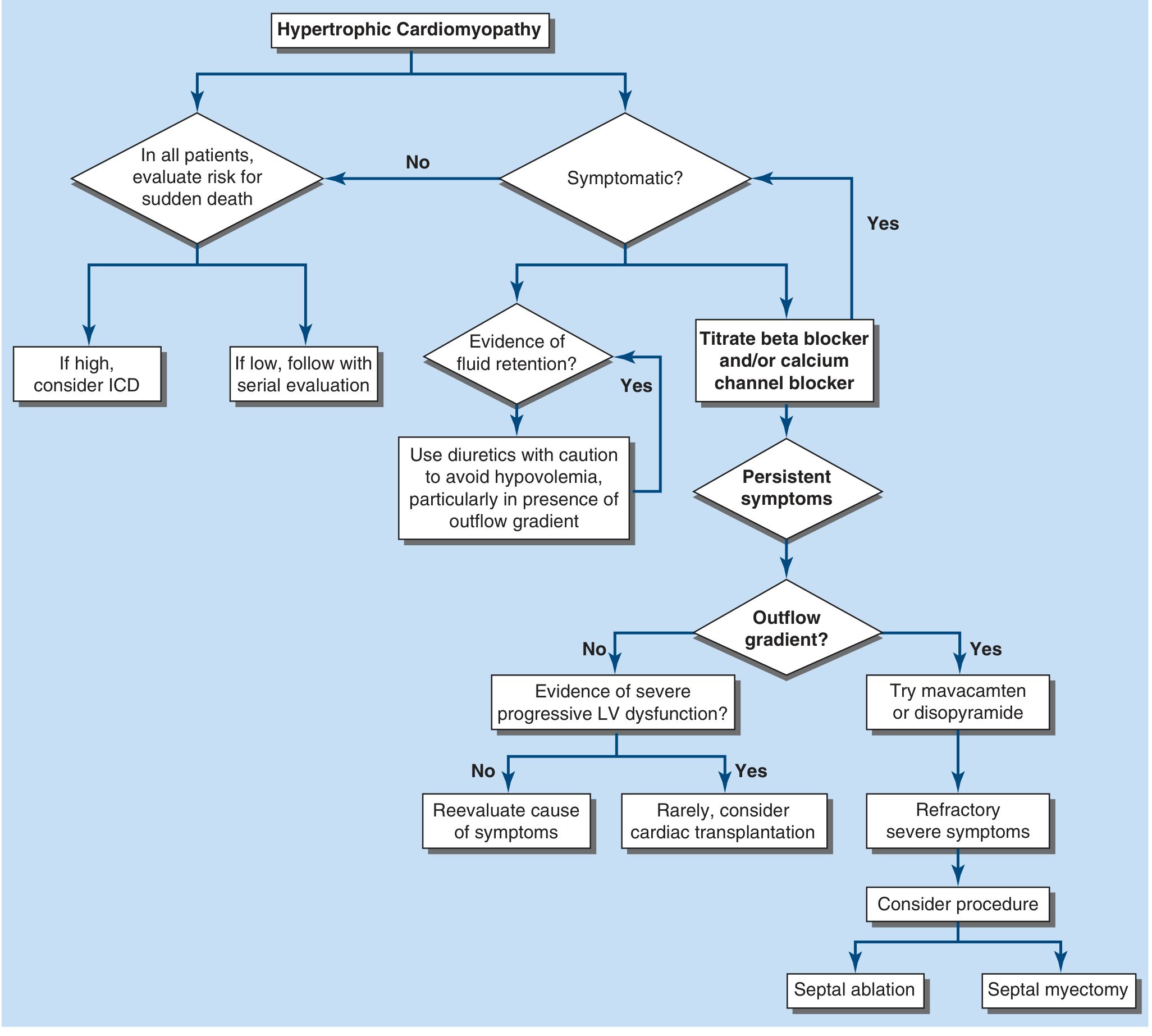
HCM management algorithm — Harrison's Principles of Internal Medicine 22E
ICD implantation is advised for patients with ≥1 major risk factor for SCD:
- Prior cardiac arrest or sustained VT
- Family history of SCD
- Massive LVH (wall thickness ≥30 mm)
- Unexplained syncope
- Abnormal BP response to exercise
- LV apical aneurysm
- Non-sustained VT on Holter
SCD risk is approximately 0.5%/year overall, but higher in young patients and those with multiple risk factors. — Harrison's 22E; Braunwald's Heart Disease
Atrial Fibrillation in HCM
- Rate control: β-blockers, verapamil
- Rhythm control: disopyramide, amiodarone
- Anticoagulation: indicated for AF regardless of CHA₂DS₂-VASc score in HCM
III. Other Causes of LVH
| Cause | Primary Treatment |
|---|---|
| Aortic stenosis | Aortic valve replacement (TAVR or SAVR) — LVH regresses post-procedure |
| Aortic/mitral regurgitation (eccentric LVH) | Valve repair/replacement when indicated |
| Acromegaly | Treat the underlying GH excess; LVH may persist post-cure |
| CKD/anemia | ESA therapy to correct anemia causes LVH regression; BP and volume control |
| Athlete's heart | No treatment needed — physiologic hypertrophy |
Summary of Drug Preference
For hypertensive LVH, the preferred agents for LVH regression:
- ARBs or ACE inhibitors — first-line, greatest evidence for LVH regression
- Thiazide-like diuretics (chlorthalidone, indapamide) — essential in combination
- Dihydropyridine CCBs — add-on, especially with angina or resistant BP
- Avoid: direct vasodilators (hydralazine, minoxidil) can worsen LVH via reflex sympathetic activation
For HCM-LVH: β-blockers → verapamil → disopyramide/mavacamten → septal reduction.
Sources: Goldman-Cecil Medicine, pp. 757–758 | Harrison's Principles of Internal Medicine 22E | Braunwald's Heart Disease | Lippincott Illustrated Reviews Pharmacology | Goodman & Gilman's Pharmacological Basis of Therapeutics | Morgan & Mikhail's Clinical Anesthesiology 7e | Brenner & Rector's The Kidney
Treatment for left ventricular hypertrophy
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Best antibiotic for cholecystitis
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.