Thalamus, Limbic System & Hypothalamus Add a note on diseases and possible treatment add diagrams and make flowcharts
Thalamus, Limbic System & Hypothalamus
Complete Study Guide with Diagrams, Flowcharts & Clinical Notes
PART 1 — THE THALAMUS
1.1 Overview & Location
"The thalamus processes almost all sensory information going to the cerebral cortex and almost all motor information coming from the cerebral cortex to the brain stem and spinal cord." - Costanzo Physiology 7th Ed., p.77
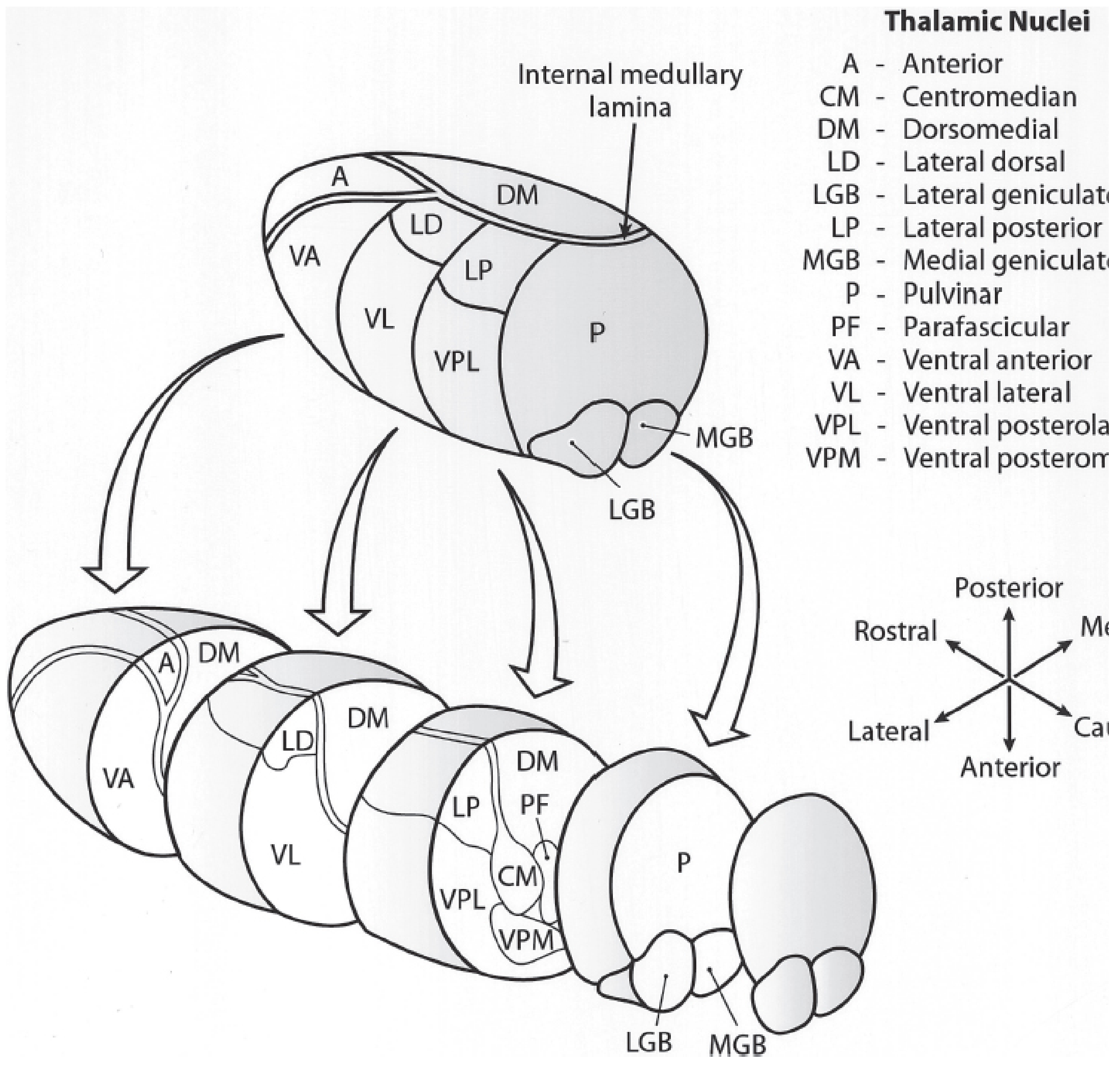
1.2 Structural Organization of Thalamic Nuclei
┌─────────────────────────────────────────────────────────────┐
│ THALAMIC NUCLEI ORGANIZATION │
├─────────────────┬───────────────────────────────────────────┤
│ GROUP │ NUCLEI INCLUDED │
├─────────────────┼───────────────────────────────────────────┤
│ Anterior │ Anterior nucleus (single large nucleus) │
│ Medial │ Medial dorsal (MD) nucleus │
│ Lateral - │ Lateral dorsal (LD), Lateral posterior │
│ Dorsal tier │ (LP), Pulvinar (P) │
│ Lateral - │ Ventral anterior (VA), Ventral lateral │
│ Ventral tier │ (VL), VPL (posterolateral), VPM │
│ │ (posteromedial) │
│ Reticular │ Thin shell; inhibitory neurons │
│ Intralaminar │ Central median (CM), Parafascicular (PF) │
│ Midline │ Cover medial surface; may fuse → │
│ │ interthalamic adhesion │
│ Geniculate │ Lateral geniculate (LGB) - vision │
│ │ Medial geniculate (MGB) - hearing │
└─────────────────┴───────────────────────────────────────────┘
1.3 Functional Classification of Thalamic Nuclei
THALAMIC NUCLEI - FUNCTIONAL TYPES
│
┌────┴──────────────────────┐
│ │
Specific Relay Nuclei Diffuse-Projection Nuclei
(topographic projections (regulate cortical
to defined cortex) excitability/arousal)
│
├── First-Order Relays
│ (drivers from ascending pathways)
│ e.g., LGB (visual), MGB (auditory)
│
└── Higher-Order Relays
(drivers from layer 5 cortical pyramidal neurons)
(>50% of primate thalamic circuits!)
Association Relay Nuclei (e.g., Medial Dorsal)
→ receive multi-source input
→ project to association cortex
| Nucleus | Input From | Projects To | Function |
|---|---|---|---|
| Anterior | Mammillary body (via fornix) | Cingulate cortex | Memory, Papez circuit |
| Medial Dorsal (MD) | Hypothalamus, Amygdala | Prefrontal cortex | Emotion, cognition |
| VPL | Medial lemniscus, spinothalamic tract | Somatosensory cortex | Body sensation |
| VPM | Trigeminal lemniscus | Somatosensory cortex (face area) | Facial sensation |
| VL | Cerebellum, basal ganglia | Motor cortex | Motor coordination |
| VA | Basal ganglia | Premotor cortex | Motor planning |
| LGB | Optic tract | Primary visual cortex (V1) | Vision |
| MGB | Inferior colliculus | Primary auditory cortex (A1) | Hearing |
| Pulvinar | Multiple cortical areas | Parietal/temporal association cortex | Multimodal integration |
| CM (intralaminar) | Brainstem reticular formation | Widespread cortex | Arousal, attention |
| Reticular nucleus | Cortex + other thalamic nuclei (collaterals) | Other thalamic nuclei (inhibitory) | Gating/modulation |
1.4 Thalamocortical Circuit Types
THREE THALAMOCORTICAL CIRCUIT SYSTEMS
1. SENSORY SYSTEM
Peripheral receptors
↓ (ascending pathways)
First-order thalamic relay (LGB, MGB, VPL, VPM)
↓
Primary sensory cortex
↓ (layer 6 feedback)
Modulates thalamic relay (via reticular nucleus)
2. MOTOR SYSTEM
Basal ganglia / Cerebellum
↓
VA / VL thalamic nuclei
↓
Frontal motor cortex (layer 5 output)
↓ (layer 5 → thalamus)
Higher-order relay loops
3. ASSOCIATION SYSTEM
Hypothalamus + Amygdala + Limbic structures
↓
Medial dorsal nucleus
↓
Prefrontal / premotor / temporal cortex
↓ (feedback)
Modulates MD nucleus again
1.5 Thalamic Diseases & Treatment
A. Thalamic (Dejerine-Roussy) Syndrome
THALAMIC INFARCTION
↓
DEJERINE-ROUSSY SYNDROME
│
┌────┴──────────────────────┐
│ │
ACUTE PHASE CHRONIC PHASE
- Contralateral - Thalamic pain (central
hemisensory loss poststroke pain)
- Transient hemiparesis - Dysesthesias + allodynia
- Hemiataxia - Hyperalgesia
- Choreoathetoid - "Thalamic hand" (athetoid
movements posture)
- "Thalamic astasia"
(disequilibrium)
- First-line: Amitriptyline (tricyclic antidepressant), Lamotrigine
- Second-line: Gabapentin, Pregabalin, Opioids
- Refractory: Deep Brain Stimulation (DBS) of thalamic pain centers
B. Thalamic Amnesia
- Caused by infarction of the anterior thalamic territory (paramedian artery territory)
- Disrupts the Papez circuit (anterior nucleus - mammillary body - fornix - hippocampus)
- Features: Anterograde amnesia, personality change, apathy
- Treatment: Cognitive rehabilitation
C. Thalamic Hemorrhage
- Hypertensive hemorrhage most common
- Features: Sensorimotor deficits, "wrong-way" eyes (conjugate gaze deviation toward the hemiplegia), consciousness disturbance
- Treatment: BP control, surgical evacuation if large
D. Fatal Familial Insomnia (FFI)
- Prion disease affecting the thalamus (dorsomedial and anterior nuclei specifically)
- Progressive untreatable insomnia → autonomic dysfunction → coma → death
- No effective treatment currently
E. Wernicke Encephalopathy
- Thiamine deficiency causes bilateral thalamic (especially medial dorsal and anterior nuclei) injury
- Features: Ophthalmoplegia, ataxia, confusion (triad)
- Treatment: IV/IM Thiamine (B1) - urgent
PART 2 — THE LIMBIC SYSTEM
2.1 Definition & Historical Background
- 1878 - Paul Broca: Named the "limbic lobe" (cingulate + parahippocampal gyri)
- 1937 - James Papez: Proposed the Papez circuit as the neural substrate for emotional behavior
- 1939 - Klüver & Bucy: Temporal lobe lesions alter affective responses (Klüver-Bucy syndrome)
- 1952 - Paul MacLean: Coined "limbic system" to describe the full emotional network
"Despite limitations, the concept of a limbic system may still be a useful way to describe the circuitry that relates certain telencephalic structures and their cognitive processes with the hypothalamus and its output pathways that control autonomic, somatic, and endocrine functions." - Kaplan & Sadock's Comprehensive Textbook of Psychiatry
2.2 Components of the Limbic System
LIMBIC SYSTEM COMPONENTS
│
┌────┴──────────────────────────────┐
│ │
LIMBIC CORTEX SUBCORTICAL STRUCTURES
│ │
┌──┴───────┐ ┌────────────┼────────────┐
│ │ │ │ │
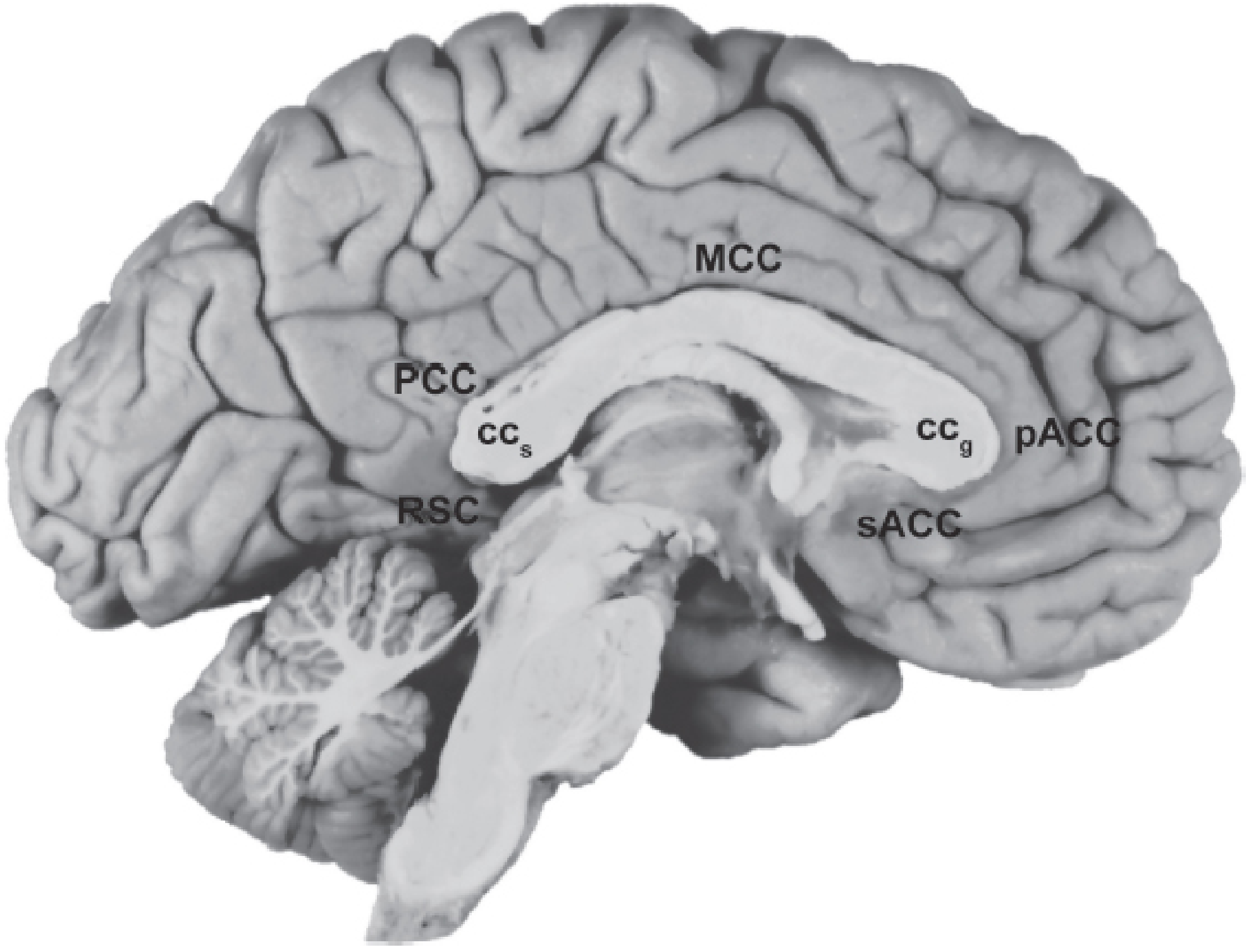
Cingulate Para- Hippocampal Amygdala Septal Area
Gyrus hippocampal Formation + related
Gyrus │ thalamic
│ │ ┌───┴──────┐ nuclei
sACC Entorhinal │Dentate │
pACC Cortex │Gyrus │
MCC │Hippocampus│
PCC │(CA1-CA3) │
RSC │Subicular │
│Complex │
└──────────┘
Also included: Hypothalamus, Mammillary bodies,
Anterior thalamic nuclei, Habenula
2.3 The Papez Circuit
PAPEZ CIRCUIT (Emotion & Memory)
Cingulate Cortex
↑ ↓
┌────────────────────────┐
│ │
Anterior Thalamic (via cingulum
Nucleus bundle)
↑ ↓
Mammillary Body ←─── Hippocampal Formation
(via mammillothalamic ↓
tract) (via fornix)
↓
Mammillary Body
2.4 Functional Summary
LIMBIC STRUCTURE → PRIMARY FUNCTION(S)
──────────────────────────────────────────────────────
Hippocampus → Declarative memory formation
(especially new episodic memory)
Amygdala → Fear conditioning, threat detection,
emotional tone of memory
Cingulate gyrus → Attention, conflict monitoring,
pain affect, emotion regulation
sACC (area 25) → Depression circuitry
pACC → Cognitive-emotional integration
PCC/RSC → Spatial navigation, autobiographical memory
Entorhinal cortex → Gateway to hippocampus (memory)
Septal area → Reward, pleasure, anxiety modulation
Habenula → Negative reward signaling;
(lateral) links limbic → serotonin/dopamine
Mammillary bodies → Memory recall (Papez circuit node)
2.5 Limbic System Diseases & Treatment
A. Depression
DEPRESSION - LIMBIC PATHOPHYSIOLOGY
│
Overactivity of sACC (Brodmann area 25)
+ Amygdala hyperreactivity
+ Reduced hippocampal volume
│
┌──────────┴──────────────────┐
│ │
TREATMENT OPTIONS MECHANISM
│
├── SSRIs / SNRIs → Normalize sACC & amygdala activity
├── Antidepressants (TCAs) → Monoaminergic modulation
├── ECT → Decreases sACC overactivity
├── rTMS → Non-invasive neuromodulation
└── DBS (area 25 / white → For treatment-resistant depression;
matter bundle) activates connected areas:
amygdala, hypothalamus, hippocampus
B. Post-Traumatic Stress Disorder (PTSD)
- Overactivation of amygdala + underactivation of prefrontal cortex (impaired fear extinction)
- Treatment: Trauma-focused CBT, SSRIs (first-line), Prazosin (nightmares), EMDR
C. Alzheimer Disease
- Earliest lesions in entorhinal cortex → hippocampus (CA1) → progressive amygdala and cingulate involvement
- Features: Anterograde amnesia first, then retrograde amnesia, behavioral changes
- Treatment: Cholinesterase inhibitors (donepezil, rivastigmine, galantamine); Memantine (NMDA antagonist); Lecanemab/Donanemab (anti-amyloid - newer)
D. Klüver-Bucy Syndrome
- Bilateral amygdala/temporal lobe destruction
- Features: Hyperorality, hypersexuality, placidity, visual agnosia, distractibility
- Causes: Herpes simplex encephalitis, Alzheimer disease, bilateral temporal lobectomy
- Treatment: Address underlying cause; behavioral management
E. Temporal Lobe (Limbic) Epilepsy
- Most common focal epilepsy; originates in hippocampus/amygdala
- Features: Aura, automatisms (lip smacking, fumbling), altered awareness
- Treatment:
TEMPORAL LOBE EPILEPSY - MANAGEMENT FLOWCHART New onset seizure ↓ MRI + EEG (confirm temporal focus) ↓ Antiseizure medications (1st line): - Carbamazepine / Oxcarbazepine - Lamotrigine / Levetiracetam ↓ If 2 drugs fail → Drug-resistant epilepsy ↓ Presurgical evaluation (video-EEG, fMRI, PET) ↓ Anterior temporal lobectomy / Amygdalohippocampectomy (60-70% seizure-free rate) ↓ If not surgical candidate: - VNS (Vagus Nerve Stimulation) - RNS (Responsive Neurostimulation) - DBS (anterior thalamus)
F. Wernicke-Korsakoff Syndrome
- Thiamine deficiency damages mammillary bodies (limbic circuit node) + medial thalamus
- Korsakoff amnesia: Severe anterograde amnesia + confabulation due to mammillary body destruction
- Treatment: Thiamine IV/IM urgently
PART 3 — THE HYPOTHALAMUS
3.1 Location & Overview
- Autonomic nervous system
- Neuroendocrine regulation (via pituitary)
- Homeostasis (temperature, hunger, thirst, sleep-wake cycles)
- Emotional/behavioral expression (via limbic connections)
3.2 Hypothalamic Regions & Nuclei
HYPOTHALAMUS - REGIONAL ORGANIZATION
(Anterior → Posterior / Medial → Lateral)
ANTERIOR POSTERIOR
REGION REGION
┌──────────────────────────────────────┐
│ Preoptic area │
│ ┌────────────────────────────────┐ │
│ │ Supraoptic nucleus (SON) │ │
│ │ → ADH + Oxytocin production │ │
│ ├────────────────────────────────┤ │
│ │ Paraventricular nucleus (PVN) │ │
│ │ → TRH, CRH, oxytocin, ADH │ │
│ ├────────────────────────────────┤ │
│ │ Suprachiasmatic nucleus (SCN) │ │
│ │ → Circadian rhythm master clock │ │
│ └────────────────────────────────┘ │
│ │
│ TUBERAL / MEDIOBASAL REGION │
│ ┌────────────────────────────────┐ │
│ │ Arcuate nucleus (ARC) │ │
│ │ → Leptin/ghrelin sensing │ │
│ │ αMSH neurons (anorexigenic) │ │
│ │ NPY/AgRP neurons (orexigenic) │ │
│ ├────────────────────────────────┤ │
│ │ Ventromedial nucleus (VMH) │ │
│ │ → Satiety center ("stop eating")│ │
│ ├────────────────────────────────┤ │
│ │ Dorsomedial nucleus (DMH) │ │
│ │ → GI function, stress responses │ │
│ └────────────────────────────────┘ │
│ │
│ LATERAL HYPOTHALAMIC AREA (LHA) │
│ → "Feeding center" (start eating) │
│ Orexin/hypocretin neurons │
│ (arousal + appetite) │
│ │
│ POSTERIOR REGION │
│ Mammillary bodies → Memory (Papez) │
│ Posterior nucleus → Sympathetic control│
└──────────────────────────────────────┘
3.3 Hypothalamic Functions Summary
| Function | Hypothalamic Region | Hormone/Pathway |
|---|---|---|
| Body temperature (heat loss) | Anterior/preoptic | Parasympathetic; sweating |
| Body temperature (heat conservation) | Posterior | Sympathetic; shivering |
| Hunger/feeding stimulation | LHA, ARC (AgRP/NPY) | NPY, AgRP, Orexin |
| Satiety/feeding inhibition | VMH, ARC (αMSH) | αMSH, CRF, Oxytocin |
| Thirst/water balance | Supraoptic, PVN | ADH (vasopressin) |
| Circadian rhythms | Suprachiasmatic nucleus | Melatonin cues from retina |
| Anterior pituitary control | Arcuate, periventricular | CRH, TRH, GnRH, GHRH, somatostatin, dopamine |
| Posterior pituitary hormones | SON, PVN (axon terminals) | ADH, Oxytocin |
| Autonomic regulation | Multiple | Sympathetic + parasympathetic balance |
| Emotional/stress responses | PVN, LHA | CRH → HPA axis |
3.4 Hypothalamic-Pituitary Control (Neuroendocrine Axis)
HYPOTHALAMIC-PITUITARY AXIS
Hypothalamus (releasing/inhibiting hormones into portal blood)
│
├── CRH ──────────────→ ACTH (anterior pituitary) → Cortisol (adrenal)
├── TRH ──────────────→ TSH → Thyroid hormones
├── GnRH ─────────────→ LH + FSH → Sex hormones
├── GHRH ────────────→ GH → IGF-1
├── Somatostatin ─────→ Inhibits GH + TSH
├── Dopamine ─────────→ Inhibits Prolactin
│
└── Direct axon projections to POSTERIOR PITUITARY:
ADH (vasopressin) → water reabsorption in kidneys
Oxytocin → uterine contraction; milk ejection; social bonding
3.5 Appetite Regulation Flowchart
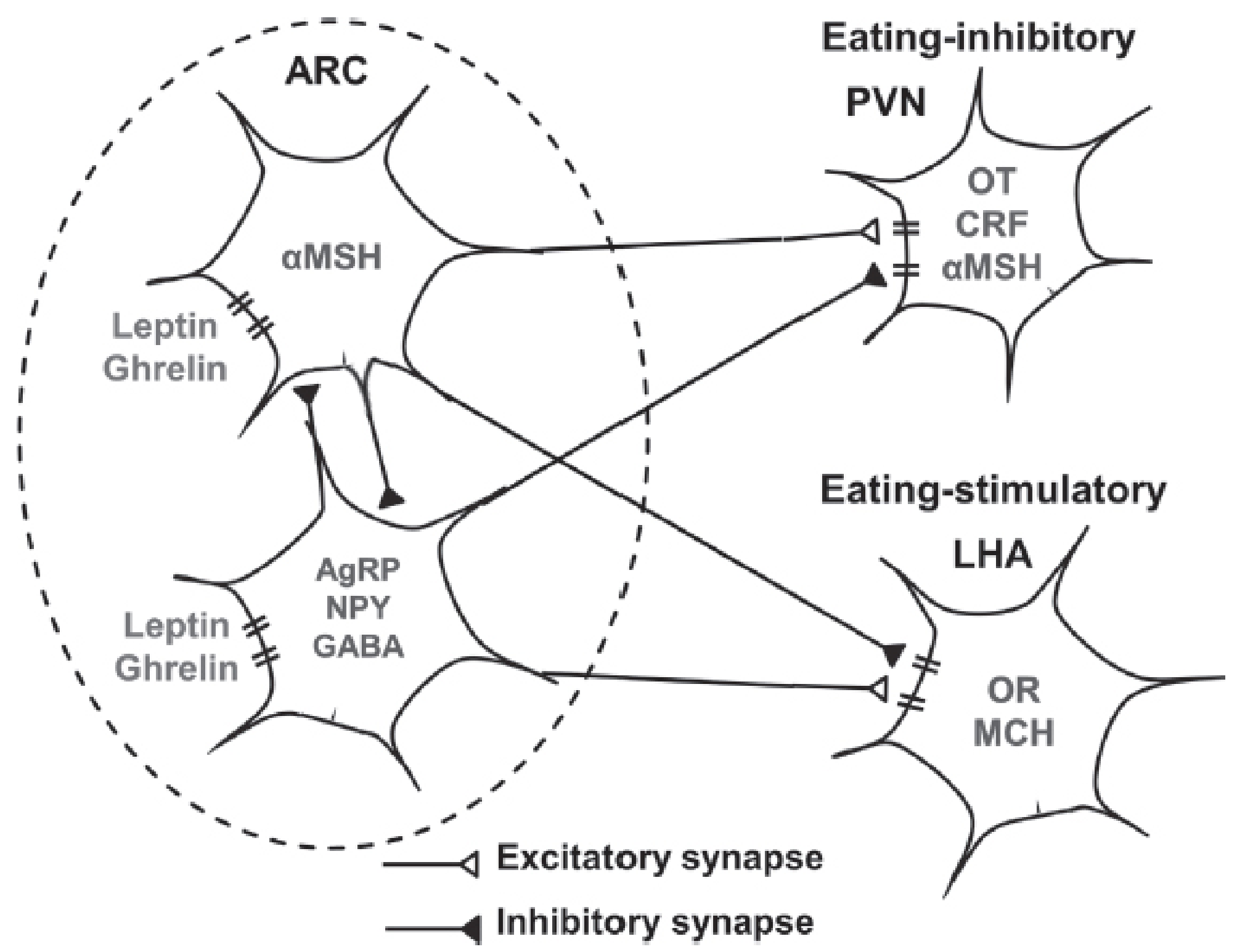
APPETITE REGULATION FLOWCHART
Low food intake → Low leptin → Low blood glucose
↓
ARC: AgRP/NPY/GABA neurons ACTIVATED
↓
├── Inhibit PVN → reduce anorexigenic peptides (CRF, OT, αMSH)
└── Stimulate LHA → increase orexigenic peptides (Orexin, MCH)
↓
HUNGER → EATING BEHAVIOUR
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Food intake → High leptin → High blood glucose
↓
ARC: αMSH neurons ACTIVATED
↓
├── Stimulate PVN → increase CRF, OT, αMSH (anorexigenic)
└── Inhibit LHA → decrease Orexin, MCH
↓
SATIETY → STOP EATING
3.6 Hypothalamic Diseases & Treatment
Flowchart: Approach to Hypothalamic Disease
HYPOTHALAMIC DYSFUNCTION - DIAGNOSTIC APPROACH
Suspected hypothalamic disease
↓
History: obesity/weight change, polyuria/polydipsia,
temperature dysregulation, amenorrhea,
sleep disturbance, personality change
↓
Investigations:
- MRI brain (gadolinium-enhanced)
- Hormone panel: TSH, ACTH/cortisol, GH, LH/FSH, prolactin
- Serum/urine osmolality (DI workup)
- Serum ACE, chest X-ray (sarcoid)
- Tumor markers (alpha-FP, beta-hCG for germ cell)
↓
┌────┴────────────────────────────────────────┐
│ │
GLOBAL DYSFUNCTION PARTIAL/SELECTIVE
(all functions impaired) DYSFUNCTION
│ │
├── Sarcoidosis ├── Diabetes Insipidus
├── Histiocytosis X ├── Hypothalamic amenorrhea
│ (Hand-Schüller-Christian, ├── Obesity/Hyperphagia
│ Letterer-Siwe, eosinophilic ├── Narcolepsy (orexin deficiency)
│ granuloma) └── SIADH
├── Craniopharyngioma
├── Germ cell tumors
├── Lymphoma / Metastases
├── Irradiation damage
└── Immune checkpoint inhibitor
therapy (iatrogenic)
A. Diabetes Insipidus (Central)
Hypothalamic lesion (tumor, trauma, granuloma, surgery)
↓
Loss of ADH secretion from SON/PVN → posterior pituitary
↓
Failure of renal tubule water reabsorption
↓
HYPOTONIC POLYURIA (urine osmolality < serum osmolality)
+ POLYDIPSIA
- Severe DI lasting days
- Paradoxical hyponatremia (release of stored ADH as neurohypophysis degenerates)
- Persistent DI (usually lifelong)
- Desmopressin (DDAVP) - synthetic ADH analog (intranasal, oral, parenteral)
- Treat underlying cause
B. SIADH (Syndrome of Inappropriate ADH)
- Excessive ADH → excess water retention → dilutional hyponatremia
- Causes: CNS lesions (including hypothalamic), pulmonary disease, certain drugs
- Treatment: Fluid restriction; if severe: hypertonic saline; Tolvaptan (V2 receptor antagonist)
C. Hypothalamic Obesity
- Lesions of VMH or other satiety centers → hyperphagia and severe obesity
- Seen after craniopharyngioma surgery, hypothalamic tumors
- Treatment: Dietary management; Octreotide (reduces insulin hypersecretion); Metreleptin (leptin replacement if leptin-deficient); Bariatric surgery in selected cases
D. Narcolepsy
OREXIN (HYPOCRETIN) DEFICIENCY
↓
Loss of lateral hypothalamic orexin neurons
(autoimmune destruction - HLA-DQB1*06:02 associated)
↓
NARCOLEPSY TYPE 1:
- Excessive daytime sleepiness (EDS)
- Cataplexy (sudden bilateral muscle weakness triggered by emotion)
- Sleep paralysis
- Hypnagogic hallucinations
- Low/absent CSF orexin-1 (<110 pg/mL)
TREATMENT:
EDS: Modafinil / Armodafinil (1st line)
Sodium oxybate (also treats cataplexy)
Pitolisant (H3 receptor inverse agonist)
Cataplexy: Sodium oxybate; SSRIs/SNRIs; TCAs (venlafaxine)
E. Hypothalamic Amenorrhea
- Functional suppression of GnRH pulsatile secretion (stress, excessive exercise, low body weight/anorexia nervosa)
- Treatment: Treat underlying cause; weight restoration; pulsatile GnRH therapy; Kisspeptin analog (investigational)
F. Temperature Dysregulation
| Lesion Location | Effect |
|---|---|
| Anterior/preoptic hypothalamus | Loss of heat dissipation → hyperthermia |
| Posterior hypothalamus | Loss of heat conservation → hypothermia |
| Diffuse hypothalamic damage | Poikilothermia (body temp tracks environment) |
PART 4 — INTEGRATED OVERVIEW
4.1 Diencephalon at a Glance
DIENCEPHALON
│
┌──┴──────────────┐
│ │
THALAMUS HYPOTHALAMUS
(relay station) (master homeostasis)
│ │
EPITHALAMUS SUBTHALAMUS
(Habenula, (Subthalamic nucleus -
Pineal gland) motor circuits)
4.2 Cross-System Disease Connections
KEY INTER-SYSTEM DISEASE LINKS
WERNICKE-KORSAKOFF SYNDROME
Thiamine deficiency
↓
Bilateral THALAMUS (MD nuclei) damage
+ MAMMILLARY BODIES (limbic) damage
↓
Wernicke (acute): ophthalmoplegia + ataxia + confusion
↓ (if untreated or incomplete treatment)
Korsakoff (chronic): amnesia + confabulation
TREATMENT: IV Thiamine URGENTLY
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
DEPRESSION CIRCUIT
sACC (Brodmann area 25) OVERACTIVITY
← Connected to amygdala + hypothalamus
↓
Thalamus (MD nucleus) also abnormal
TREATMENT: Antidepressants / DBS of sACC white matter
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
ALZHEIMER DISEASE
Entorhinal cortex → Hippocampus (CA1) → Amygdala
→ Anterior thalamic nuclei → Cingulate gyrus
Progressive memory failure → behavioral change
TREATMENT: Cholinesterase inhibitors; Memantine;
Anti-amyloid mAbs (Lecanemab)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STROKE AFFECTING THALAMUS + LIMBIC
Paramedian thalamic infarction
→ Anterior nucleus damage (Papez circuit disrupted)
+ Medial dorsal nucleus damage
→ THALAMIC AMNESIA + personality change
TREATMENT: Stroke rehabilitation; cognitive therapy
Quick Reference Table — Diseases, Structures & Treatments
| Disease | Primary Structure(s) Affected | Key Features | Treatment |
|---|---|---|---|
| Thalamic pain (Dejerine-Roussy) | Posterior ventrobasal thalamus | Contralateral burning pain, allodynia | Amitriptyline, Lamotrigine, DBS |
| Thalamic amnesia | Anterior + MD thalamus | Anterograde amnesia, apathy | Rehabilitation |
| Fatal Familial Insomnia | Thalamus (DM, anterior nuclei) | Progressive insomnia, dysautonomia | Supportive only |
| Wernicke encephalopathy | Thalamus + mammillary bodies | Ophthalmoplegia, ataxia, confusion | IV Thiamine urgently |
| Korsakoff syndrome | Mammillary bodies + MD thalamus | Anterograde amnesia, confabulation | Thiamine; care |
| Depression | sACC, amygdala, hippocampus | Low mood, anhedonia | SSRIs, DBS of sACC |
| PTSD | Amygdala (hyperactive), PFC (hypo) | Fear, flashbacks, avoidance | CBT, SSRIs, Prazosin |
| Temporal lobe epilepsy | Hippocampus, amygdala | Aura, automatisms | AEDs → surgery → VNS/DBS |
| Alzheimer disease | Entorhinal → hippocampus → amygdala | Progressive amnesia | Cholinesterase inhibitors, Memantine |
| Klüver-Bucy syndrome | Bilateral amygdala/temporal | Hyperorality, hypersexuality, placidity | Treat cause; behavioral Rx |
| Diabetes insipidus (central) | SON/PVN, posterior pituitary | Polyuria, polydipsia | Desmopressin (DDAVP) |
| Narcolepsy type 1 | Lateral hypothalamus (orexin cells) | EDS, cataplexy | Modafinil, Sodium oxybate |
| Hypothalamic obesity | VMH, satiety centers | Hyperphagia, severe obesity | Dietary, Octreotide, surgery |
| Craniopharyngioma | Hypothalamus-pituitary axis | Multiple endocrine deficits | Surgery ± radiotherapy |
| Sarcoidosis (hypothalamic) | Hypothalamus (global) | DI, panhypopituitarism | Corticosteroids |
| SIADH | ADH overproduction | Hyponatremia, euvolemia | Fluid restriction, Tolvaptan |
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry (thalamic organization, limbic system, hypothalamic appetite circuits)
- Costanzo Physiology 7th Edition, p.77 (thalamus and hypothalamus overview)
- Adams and Victor's Principles of Neurology, 12th Edition (hypothalamic syndromes, DI)
- Bradley and Daroff's Neurology in Clinical Practice (thalamic pain/Dejerine-Roussy syndrome)
- Neuroanatomy through Clinical Cases 3rd Edition (limbic/thalamic anatomy)
Make images of these flowcharts and diagrams make a summary
Medical education diagram: Thalamic Nuclei Organization chart. Clean anatomical diagram showing the thalamus divided into groups by the internal medullary lamina (Y-shaped). Label all nuclei: Anterior (A), Medial Dorsal (DM), Lateral group with dorsal tier (LD, LP, Pulvinar P) and ventral tier (VA, VL, VPL, VPM), Reticular nucleus (thin shell), Intralaminar nuclei (CM centromedian, PF parafascicular), Medial Geniculate (MGB) and Lateral Geniculate (LGB). Use color coding for each group. Include a table on the side showing nucleus, input, output, and function. Professional neuroscience textbook style, white background.
Medical education flowchart: The Papez Circuit and Limbic System. Circular flowchart showing the Papez emotion and memory circuit with labeled arrows: Hippocampal Formation → (via fornix) → Mammillary Bodies → (via mammillothalamic tract) → Anterior Thalamic Nucleus → (via thalamocortical fibers) → Cingulate Cortex → (via cingulum bundle) → back to Hippocampal Formation. In the center, label it "PAPEZ CIRCUIT - Emotion & Memory". Around the outside, show additional modern limbic structures: Amygdala (fear/reward), Subgenual ACC/area 25 (mood), Entorhinal Cortex (memory gateway), Habenula (mood regulation via serotonin/dopamine). Use blue and green color scheme, arrows clearly labeled, professional medical education style, white background.
Medical education diagram: Hypothalamus functional zones and nuclei. Sagittal cross-section diagram of the hypothalamus showing anterior, tuberal/mediobasal, and posterior regions. Label all key nuclei with their functions: Supraoptic nucleus (ADH + Oxytocin), Paraventricular nucleus (TRH CRH Oxytocin ADH), Suprachiasmatic nucleus (circadian rhythms), Arcuate nucleus (leptin/ghrelin sensing - two populations: αMSH anorexigenic and AgRP/NPY orexigenic), Ventromedial nucleus VMH (satiety center), Dorsomedial nucleus, Lateral Hypothalamic Area LHA (feeding center orexin), Mammillary bodies (memory Papez circuit), Posterior nucleus (sympathetic). Color code by function: blue for water/electrolytes, green for feeding, orange for hormones, purple for autonomic. Professional anatomy textbook style, white background.
Medical education flowchart: Hypothalamic Appetite Regulation. Two parallel pathways. LEFT pathway labeled HUNGER: Low leptin + High ghrelin → ARC nucleus AgRP/NPY/GABA neurons ACTIVATED → inhibit PVN (reduce anorexigenic signals CRF OT αMSH) AND stimulate LHA (increase orexigenic signals Orexin MCH) → HUNGER → EATING. RIGHT pathway labeled SATIETY: High leptin + Low ghrelin → ARC nucleus αMSH neurons ACTIVATED → stimulate PVN (increase CRF OT αMSH) AND inhibit LHA (decrease Orexin MCH) → SATIETY → STOP EATING. Use orange for hunger/orexigenic pathway and green for satiety/anorexigenic pathway. Bold arrows, clean boxes, professional medical style, white background.
Medical education flowchart: Thalamic and Limbic Diseases with treatments. Clean clinical flowchart with 6 disease boxes arranged in a grid. Each box has disease name, affected structure, key features, and treatment. Box 1: Thalamic Pain Syndrome (Dejerine-Roussy) - posterior ventrobasal thalamus - burning contralateral pain allodynia - Amitriptyline Lamotrigine DBS. Box 2: Wernicke-Korsakoff - thalamus + mammillary bodies - ophthalmoplegia ataxia confusion amnesia - IV Thiamine URGENT. Box 3: Temporal Lobe Epilepsy - hippocampus amygdala - aura automatisms - AEDs then surgery. Box 4: Alzheimer Disease - entorhinal cortex hippocampus amygdala - progressive amnesia - Donepezil Memantine. Box 5: Narcolepsy Type 1 - lateral hypothalamus orexin cells - EDS cataplexy - Modafinil Sodium oxybate. Box 6: Diabetes Insipidus central - SON PVN hypothalamus - polyuria polydipsia - Desmopressin DDAVP. Red borders for each box, professional clinical reference card style, white background.
Medical education summary poster: Thalamus Limbic System and Hypothalamus comprehensive overview. Three-column layout. Column 1 THALAMUS: relay station of brain, 6 nuclear groups (Anterior Memory, Medial Dorsal Emotion/Cognition, Lateral Sensory/Motor, Reticular Gating, Intralaminar Arousal, Geniculate Vision/Hearing), key disease: Thalamic Pain Syndrome treated with Amitriptyline. Column 2 LIMBIC SYSTEM: emotion memory autonomic, key structures Hippocampus (declarative memory), Amygdala (fear/reward), Cingulate gyrus (mood/attention), Papez circuit diagram (small), key diseases: Depression (DBS sACC), Temporal lobe epilepsy (surgery), Alzheimer (Donepezil). Column 3 HYPOTHALAMUS: master homeostasis, functions: temperature water balance hunger pituitary control circadian rhythm, key diseases: Diabetes Insipidus (Desmopressin), Narcolepsy (Modafinil), Hypothalamic obesity (Octreotide). Title at top in bold. Color: thalamus in blue, limbic in green, hypothalamus in orange. Clean professional medical poster style, white background.
429 Too Many Requests. {'message': '{\n "error": {\n "code": 429,\n "message": "Resource exhausted. Please try again later. Please refer to https://cloud.google.com/vertex-ai/generative-ai/docs/error-code-429 for more details.",\n "status": "RESOURCE_EXHAUSTED"\n }\n}\n', 'status': 'Too Many Requests'}
We encountered an error while processing your request. Please try again or reach out to us for help.