Abdominal wall reconstruction
Reading File
Finding Sources
Searching PubMed
"abdominal wall reconstruction" AND "component separation"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
I now have rich content from multiple authoritative surgical textbooks plus recent meta-analyses. Let me compose the comprehensive response.
Abdominal Wall Reconstruction (AWR)
Overview
AWR refers to the restoration of structural and functional integrity of the musculofascial abdominal wall, most commonly for large or complex ventral/incisional hernias. The foundational principle for midline defects is medialization of the rectus abdominis (RA) muscles to restore the linea alba, achieved through a set of "releases" that overcome the resistance imposed by hernia-induced anatomical changes. Goals include:
- Restoration of linea alba and abdominal wall anatomy
- Creation of a dynamic, physiologic truncal muscle complex
- Adequate prosthetic reinforcement
- Durable, well-vascularized soft tissue coverage
Approximately 350,000 incisional hernia repairs are performed annually in the US, ranging from simple outpatient procedures to complex AWR with significant comorbidities and complications.
- Current Surgical Therapy 14e, p. 736; Fischer's Mastery of Surgery 8e, p. 897
Surgical Anatomy
Muscle Groups
| Region | Muscles |
|---|---|
| Midline | Rectus abdominis (RA), variable pyramidalis |
| Anterolateral | External oblique (EOM), internal oblique (IOM), transversus abdominis (TAM) |
The TAM extends medially under the lateral edge of the rectus and is a major contributor to the posterior rectus sheath in the upper abdomen. Near the xiphoid, TAM fibers interdigitate with the anterior diaphragm.
Key Tendinous Structures
- Linea alba: connects both RA complexes from xiphoid to pubic symphysis; composed of aponeuroses of EOM, IOM, TAM. Its restoration is the central goal of AWR.
- Linea semilunaris: connects the midline and anterolateral groups. Iatrogenic injury leads to major hernia and abdominal wall morbidity.
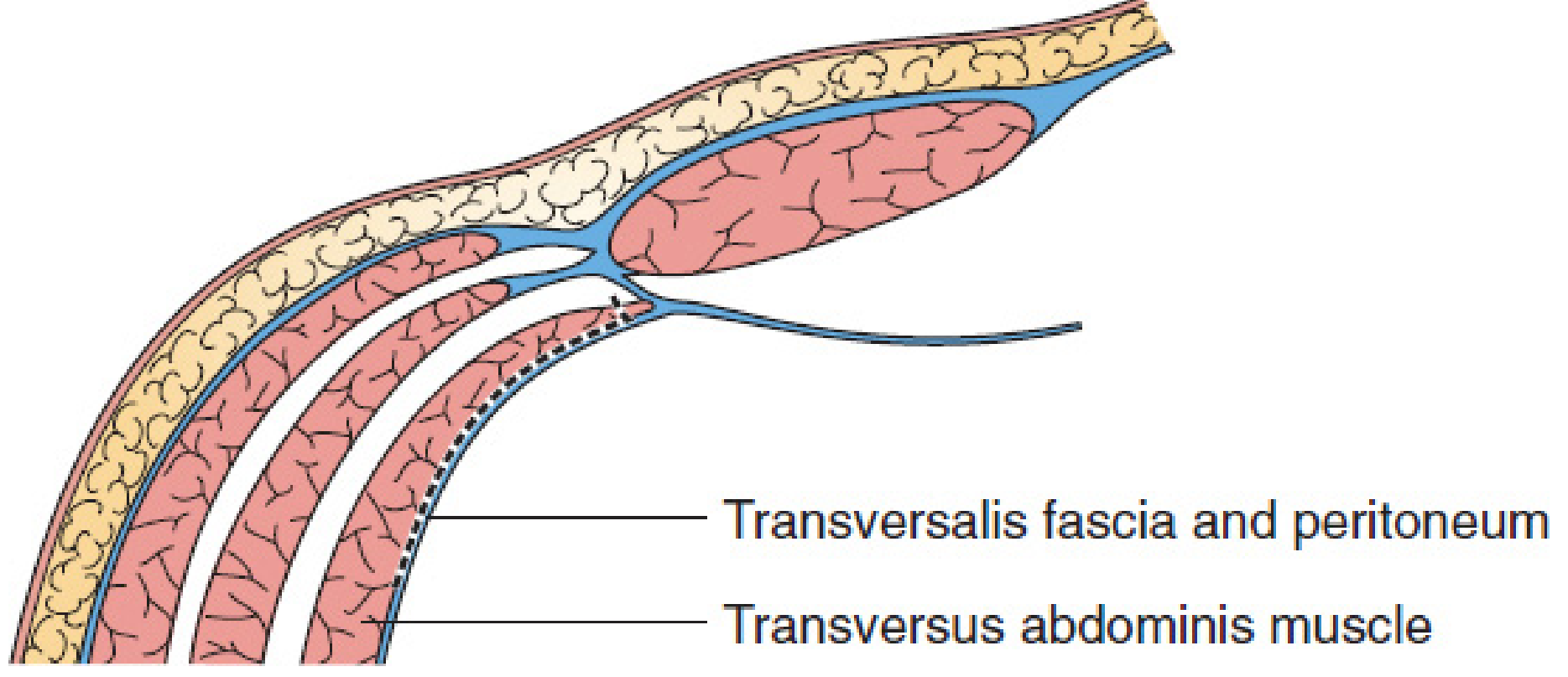
- Arcuate line of Douglas (linea semicircularis): inferior border of the posterior rectus sheath. Below this, only transversalis fascia and peritoneum form the posterior envelope.
Vascular Zones
| Zone | Location | Supply |
|---|---|---|
| Zone 1 | RA complex, above umbilicus | Superior + inferior epigastric arteries |
| Zone 2 | Below umbilicus | Iliac, femoral, inferior epigastric arteries |
| Zone 3 | Lateral to semilunar line | Lumbar + intercostal arteries |
Nerve Supply
Thoracolumbar spinal cord T6/7-T11/L1; neurovascular bundles run in the IOM-TAM plane, piercing the posterior sheath just medial to the linea semilunaris. This is the anatomical basis for both the TAP block and the key landmark during retrorectus dissection.
- Current Surgical Therapy 14e, p. 736
Indications and Patient Selection
AWR is indicated for:
- Large midline incisional hernias (especially with loss of domain)
- Complex hernias after damage control surgery / open abdomen
- Hernias with recurrence after prior repair
- Fascial defects after tumor resection
- Enteroatmospheric or enterocutaneous fistula with associated fascial disruption
Preoperative Optimization (Mandatory)
Complex AWR carries high morbidity if risk factors are not addressed:
| Risk Factor | Target |
|---|---|
| Diabetes | HbA1c < 7 |
| Smoking | Cessation ≥ 4-6 weeks (verify with urine cotinine) |
| Obesity | Normalize BMI where possible |
| Nutrition | Maximize protein-calorie repletion |
| MRSA history | Decolonization; vancomycin prophylaxis |
| Active infection | Clear before elective repair |
A preoperative CT scan of the abdominal wall is essential before any major reconstruction to plan the approach and assess residual anatomy.
- Sabiston Textbook of Surgery, p. 723
Surgical Techniques
1. Anterior Component Separation (ACS) - Ramirez Technique (1990)
The original description by Ramirez consists of:
- Large subcutaneous myocutaneous advancement flaps
- Release of the external oblique aponeurosis lateral to the semilunar line
- Allows 3-5 cm of additional length per side
Limitation: High wound morbidity due to extensive subcutaneous dissection, devascularization of skin perforators. Not recommended for high-risk patients.
Endoscopic modification: Avoids division of perforators by using an endoscopic camera to release the external oblique aponeurosis through small access incisions - reducing wound complications.
2. Rives-Stoppa-Wantz Repair (Retrorectus Repair)
The preferred technique for most midline defects without need for posterior release:
- The posterior rectus sheath is incised ~0.5 cm from the fascial edge of the defect
- The retrorectus plane is developed laterally to the linea semilunaris
- Lightweight macroporous synthetic mesh is placed in the retromuscular (sublay) position
- Posterior rectus sheath and peritoneum protect the bowel from direct mesh contact
- No major subcutaneous dissection - preserves neurovascular bundles and perforators
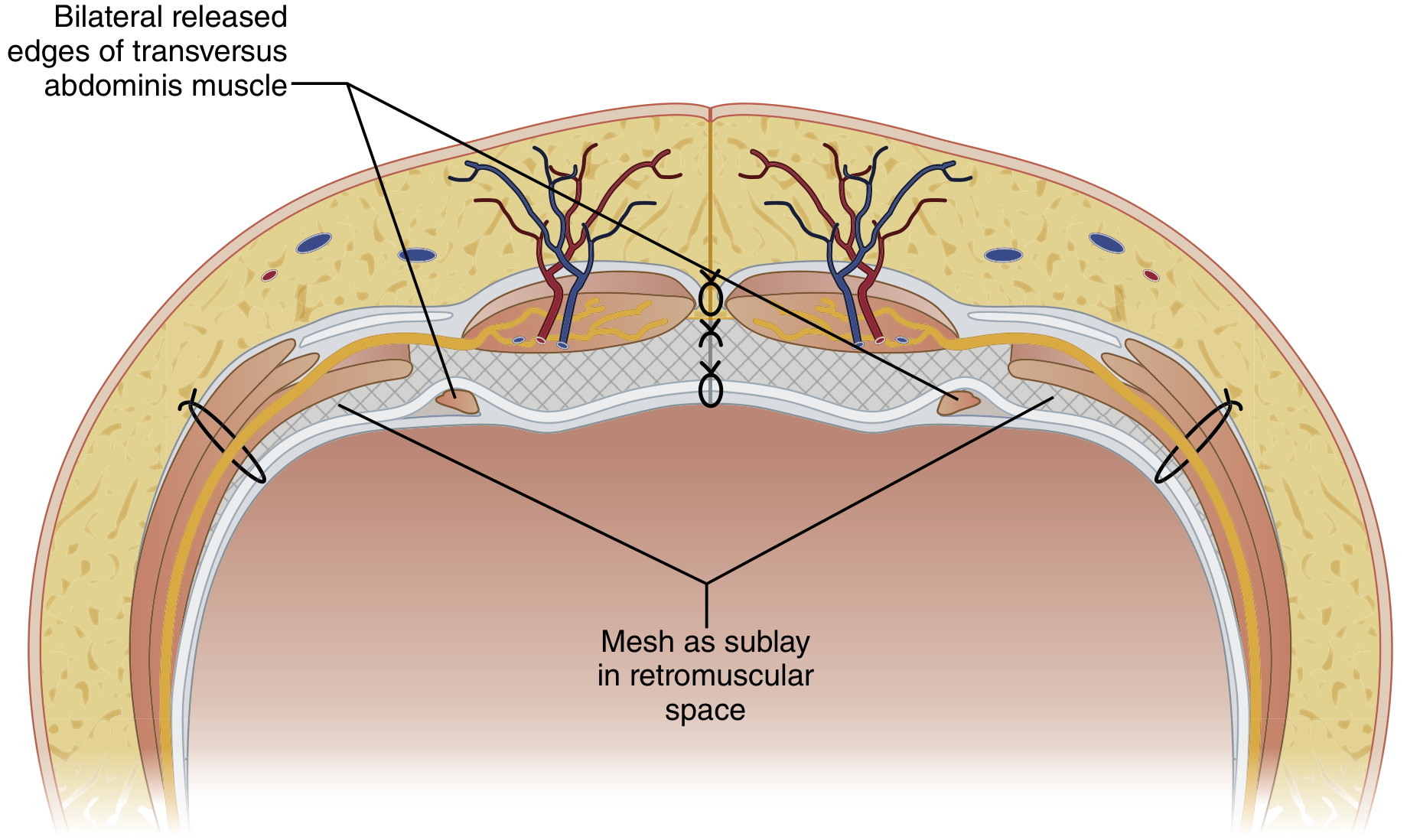
Retrorectus mesh positioning after Rives-Stoppa-Wantz repair, showing mesh as sublay in the retromuscular space with bilateral released edges of TAM.
3. Transversus Abdominis Release (TAR) - Posterior Component Separation
TAR is an extension of the retrorectus approach used when the standard retrorectus dissection is insufficient to close the posterior rectus fascia. It provides significantly greater fascial advancement.
Steps:
- Begin with retrorectus dissection to the linea semilunaris
- Incise the posterior lamella of the internal oblique (first layer of the posterior rectus sheath) just medial to the neurovascular bundles
- Divide the transversus abdominis muscle (upper abdomen) or its aponeurosis (mid/lower abdomen) to enter the pretransversalis plane or preperitoneal plane
- Lateral dissection continues to at least the mid-axillary line, and can reach the psoas posteriorly
- Superiorly: can extend under the diaphragm
- Inferiorly: extends into the Space of Retzius, exposing the symphysis and Cooper ligament
The posterior rectus sheath is incised 0.5-1 cm medial to the anterior/posterior junction, exposing the underlying TAM. Perforator nerves are preserved during retromuscular dissection.
Fascial advancement achieved (cadaver study data):
| Step | Anterior fascial gain (per side) |
|---|---|
| Retrorectus alone | 4-7 cm |
| + Posterior lamella of IOM incision | Slight additional gain |
| + TAM division | ~1 cm more |
| + Full lateral preperitoneal dissection | 5-10 cm total |
| Posterior sheath medialization | 7-11 cm (greatest gain) |
This disinsertion of the TAM releases the circumferential tension it applies, allowing medialization of the rectus abdominis across the midline defect. After posterior closure, a large retromuscular space is created for mesh placement.
- Mulholland and Greenfield's Surgery 7e, p. 3742-3743; Sabiston Textbook of Surgery, p. 723
Mesh Placement
| Position | Technique | Pros | Cons |
|---|---|---|---|
| Retromuscular (sublay) | RSW, TAR | Protected from bowel; wide overlap; best incorporation | Requires posterior sheath closure |
| Onlay | Anterior to fascia | Simple | High wound infection rate; poor overlap |
| Underlay (intraperitoneal) | IPOM | Laparoscopic-friendly | Bowel adhesion risk; requires anti-adhesion coating |
The retromuscular position is widely considered the procedure of choice - it avoids major subcutaneous dissection, protects the bowel via posterior sheath and omentum, and allows wide mesh overlap.
Staged Management of the Open Abdomen ("Difficult Abdominal Wall")
When primary fascial closure is not possible (achieved in 60-90% of damage control laparotomies), a staged approach is used:
Stage 1: Temporary Abdominal Closure (TAC)
- Techniques: Bogota bag, Wittmann patch, vacuum-assisted wound closure (VAC)
- Goals: tension-free, atraumatic, inexpensive, facilitates delayed primary closure
Stage 2: Skin Grafting / Wound Temporization
- For patients where fascial closure has failed and bowel is exposed
- Split-thickness skin graft over granulating viscera provides biological coverage
Stage 3: Definitive AWR
- Optimal timing: 6-12 months post-skin grafting, once graft has adequately separated from viscera
- Pinch test: if bowel falls away, adhesions are likely filmy and reconstruction is feasible
- Mid-portion of graft separates first; densest adhesions at the graft-musculofascial junction
- After 12 months, abdominal musculature contracts leading to progressive loss of domain
Modified component separation (Fischer's technique for giant defects) adds modifications to the standard Ramirez technique to accommodate the extreme fascial deficits typical of staged reconstruction.
- Fischer's Mastery of Surgery 8e, p. 7526; Sabiston Textbook of Surgery, p. 719
Perioperative Considerations
Intraoperative Monitoring
- Plateau pressure: if raised >6 mmHg after closure, pulmonary complications increase 9-fold
- Bladder pressure (indirect abdominal pressure): routinely recommended when defect >600 cm²
Pain Management
- Epidural catheters and TAP blocks substantially improve postoperative pain, reduce narcotic use, improve early mobilization
- Long-acting bupivacaine (e.g., liposomal) for prolonged relief
ICG Fluorescence Angiography (FA) for Flap Perfusion
-
Sensitivity 100%, specificity 91% for predicting flap necrosis
-
In the only prospective RCT: intraoperative flap modification was required in 37% when FA was used vs. 4% with clinical judgment alone (p<0.001)
-
ICG dose: 2.5 cc of 25 mg/10 mL solution IV; half-life 3-5 min allows repeat assessment
-
Note: intraoperative modification did not translate to reduced skin necrosis rates in the RCT
-
Fischer's Mastery of Surgery 8e, p. 897-898
Postoperative Care
- Incisional VAC changed at 24 hours to confirm midline viability
- Abdominal binder: throughout hospitalization and outpatient recovery
- NG tube: until true return of bowel function (avoid distension stress on repair)
- Antibiotics: 24 hours perioperatively; not needed beyond that unless contaminated field
- Early mobilization: key to success; aided by multimodal analgesia
- Drains: remove sequentially (one per side per day); remove before discharge when feasible
- Suture removal: 2 weeks in outpatient setting
- No heavy lifting for 2 months
Complications
| Complication | Notes |
|---|---|
| Wound infection / skin necrosis | Leading cause of repair failure. Risk with obesity (tense skin flaps) and very thin patients (devascularized thin flaps). Manage with negative-pressure dressings; skin graft if extensive |
| Seroma / hematoma | Prevented by meticulous hemostasis on fascial and skin flap surfaces; managed with careful drain management |
| Recurrence | Associated with wound complications, inadequate mesh overlap, or failure of fascial closure |
| Pulmonary complications | Due to raised intraabdominal pressure after closure; monitor plateau pressure intraoperatively |
| Abdominal compartment syndrome | Risk with large defect repair; bladder pressure monitoring for defects >600 cm² |
Recent Evidence (2024-2025)
Three recent meta-analyses are relevant:
-
Open vs. robotic TAR (Lima et al., Surg Endosc 2024, PMID 39528659): Updated systematic review and meta-analysis with meta-regression comparing open and robotic transversus abdominis release for ventral hernia repair.
-
Minimally invasive posterior component separation (Tryliskyy et al., Hernia 2024, PMID 38632220): Systematic review and meta-analysis of short-term outcomes comparing MIS techniques for posterior component separation.
-
Preoperative botulinum toxin A (BTA) (Florencio de Mesquita et al., Hernia 2025, PMID 39966195): Meta-analysis of propensity-matched studies with trial sequential analysis supporting BTA injection for progressive pneumoperitoneum and lateral muscle paralysis in complex AWR - allows gradual expansion of the abdominal domain before surgery.
Summary: Technique Selection Framework
Midline defect
├─ Small-moderate, no release needed → Rives-Stoppa-Wantz (retrorectus mesh)
├─ Larger, needs more mobilization → TAR (posterior component separation + retromuscular mesh)
├─ Lateral/oblique defect or EOM release needed → Anterior component separation (endoscopic preferred)
├─ Contaminated field → Biologic or biosynthetic mesh; avoid permanent synthetic
└─ Giant defect + open abdomen → Staged repair (TAC → skin graft → delayed AWR at 6-12 months)
Sources: Current Surgical Therapy 14e; Sabiston Textbook of Surgery; Fischer's Mastery of Surgery 8e; Mulholland and Greenfield's Surgery 7e
This is a shared conversation. Sign in to Orris to start your own chat.