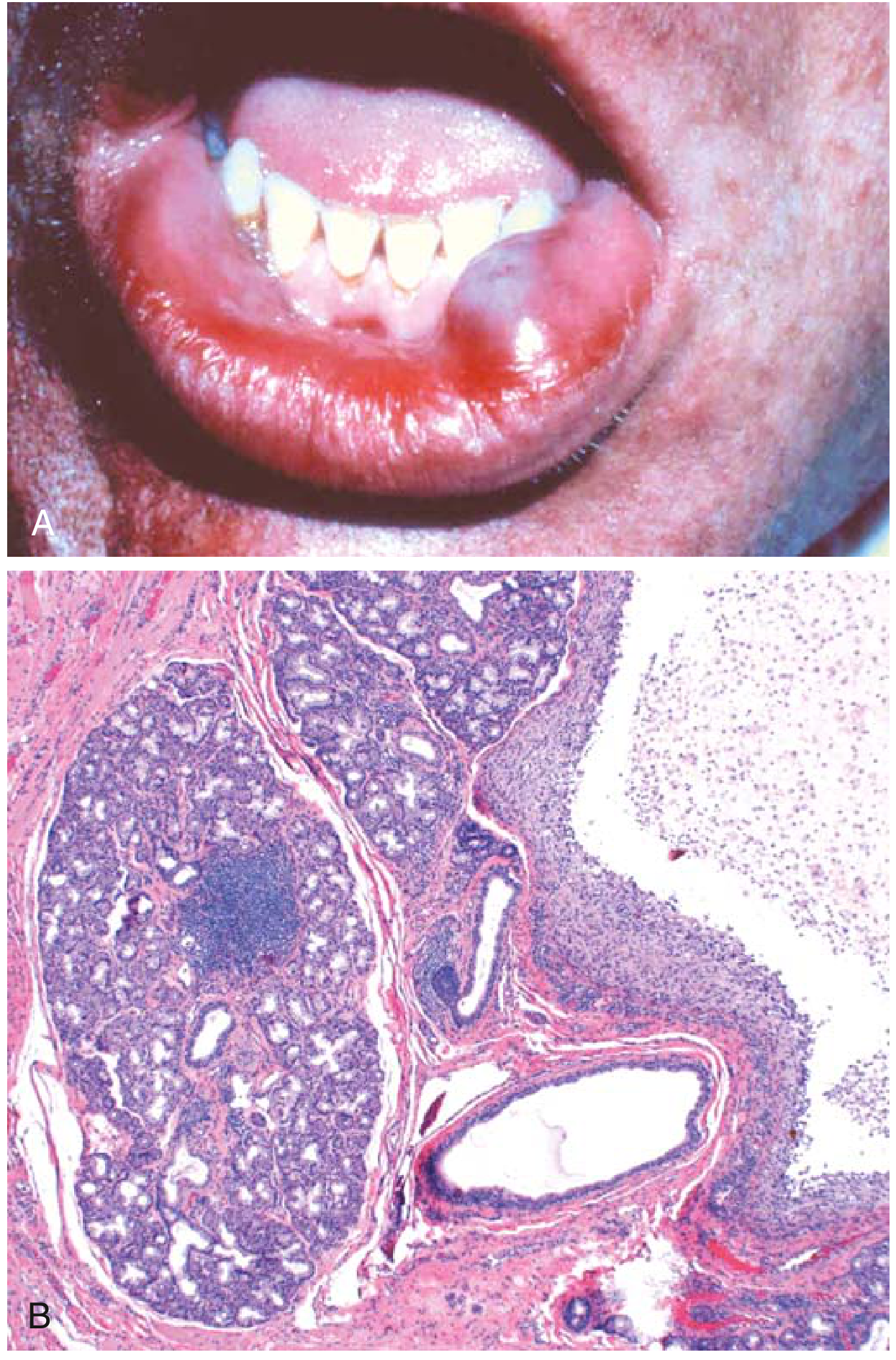
white fluid filled swelling on lower lip for 2 weeks in a 26yrs old male
Reading File
Finding Sources
Finding Sources
Searching Images
mucocele lower lip fluid filled swelling
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple textbooks. Here is a complete clinical answer:
Mucocele of the Lower Lip
The presentation — a white/translucent, fluid-filled swelling on the lower lip in a young adult for 2 weeks — is classic for a mucocele (mucous extravasation phenomenon), the most common minor salivary gland lesion.

Definition & Pathogenesis
A mucocele results from disruption of a minor salivary gland duct — typically from lip-biting trauma — causing extravasation of sialomucin into the submucosal connective tissue. This triggers an inflammatory response, granulation tissue formation, and eventual fibrosis around the mucus pool. The result is a pseudocyst (no true epithelial lining) filled with mucinous material. — Andrews' Diseases of the Skin, p. 34.21
A distinct but related entity — the mucous retention cyst — arises from true ductal obstruction and does have an epithelial lining; it tends to occur in the posterior oral mucosa.
Why the Lower Lip?
The lower lip is the most common site because it is the area most vulnerable to self-biting trauma, with minor salivary glands adjacent to the lower incisor region. — Pfenninger & Fowler's Procedures for Primary Care
Clinical Features
| Feature | Details |
|---|---|
| Age | Most common in 2nd–4th decades (your patient fits perfectly) |
| Location | Lower labial mucosa (most common); also buccal mucosa, ventral tongue |
| Appearance | Dome-shaped, smooth, soft, fluctuant, translucent with bluish/white tint |
| Size | 2–10 mm (occasionally larger) |
| Symptoms | Painless; tense |
| Contents | Sticky, straw-colored (or bluish if hemorrhage) mucous fluid |
| Behavior | Undergoes cycles of swelling → spontaneous rupture → refilling |
The color depends on depth: very superficial lesions appear vesicular/white; slightly deeper ones have a bluish hue; deep lesions show no color change. — Dermatology 2-Volume Set 5e, Fig. 72.22
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Mucous retention cyst | True epithelial lining; posterior oral mucosa; duct obstruction |
| Ranula | Mucocele of floor of mouth (sublingual gland); larger |
| Lipoma | Softer, doughy, not translucent, no fluid |
| Fibroma (traumatic) | Firm, flesh-colored, no fluid |
| Haemangioma | Blanches on pressure, vascular hue |
| Lymphangioma | Usually multilocular, different age group |
| Benign salivary gland tumor | Firm, slow-growing, non-fluctuant |
| Mucoepidermoid carcinoma | Rare at this site but consider if atypical appearance or rapid growth |
⚠️ Any atypical appearance, unusual location, or pulsating mass should be biopsied to exclude carcinoma.
Histopathology
- Cyst-like cavity filled with mucinous material
- No true epithelial lining (distinguishes it from a retention cyst)
- Lined by organizing granulation tissue / fibrous wall
- Surrounding inflammatory infiltrate
- Normal minor salivary gland acini adjacent to the lesion
Management
Conservative first:
- Small lesions or first presentation: observe, as some resolve spontaneously after rupture
- Avoid further trauma (advise against lip-biting)
Procedural options:
-
Incision & drainage + cryotherapy (first-line for small/initial lesions)
- Local anaesthesia (lidocaine 2% with 1:100,000 epinephrine injected under the lesion)
- Stab wound with no. 11 blade to express contents
- Cryotherapy with 2–3 mm ice rim around lesion
-
Surgical excision (preferred for larger, recurrent, or deep lesions)
- Excisional biopsy is both diagnostic and curative
- Roof shaved with no. 15 blade, then electrodesiccation/cryo of base
- For recurrent deep lesions: complete excision or marsupialization with fine absorbable sutures
-
Laser ablation (Er:Cr:YSGG or CO₂ laser) — effective with good haemostasis and healing
-
Micromarsupialization — 4-0 silk suture placed through the widest diameter, left for 7 days; good for small recurrent lesions
Recurrence is the main concern; complete removal of the associated minor salivary gland reduces recurrence. — Pfenninger & Fowler's Procedures for Primary Care, p. 213–214
Key Points Summary
- Diagnosis: Mucocele (mucous extravasation phenomenon) — most likely
- Cause: Minor trauma (lip biting) → duct rupture → mucus extravasation
- Confirm: Clinical appearance is usually diagnostic; excisional biopsy is definitive
- Treat: Surgical excision/destruction; include associated salivary gland tissue to prevent recurrence
- Refer: To oral surgery or ENT if recurrent, atypical, or suspicion of malignancy
Sources: Andrews' Diseases of the Skin (Clinical Dermatology); Robbins & Kumar Basic Pathology; Dermatology 2-Volume Set 5e; Pfenninger & Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.