Pre auricular sinus in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
"preauricular sinus" treatment surgery
Searching the Web
preauricular sinus RGUHS ENT 20 marks recent advances 2024
Reading File
Reading File
Finding Sources
Searching PubMed
"preauricular sinus" excision recurrence
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
Searching PubMed
"preauricular sinus" supra-auricular approach
PREAURICULAR SINUS - A Comprehensive 20-Mark Answer (RGUHS)
Sources: Scott-Brown's (Vol 2), Cummings Otolaryngology, Shambaugh's Surgery of the Ear, K.J. Lee's Essential Otolaryngology, Bailey & Love, S. Das Manual of Clinical Surgery, Dhingra, Hazarika, Stell & Maran (integrated from referenced content), with recent PubMed evidence (2021-2026)
1. DEFINITION
A preauricular sinus (also called preauricular pit, preauricular fistula, or ear pit) is a congenital malformation consisting of a narrow, blind-ended epithelium-lined tract opening as a pit or depression anterior to the ascending limb of the helix. It represents a defect in auricular embryogenesis and is one of the most common congenital anomalies of the external ear.
2. EMBRYOLOGY
AURICULAR DEVELOPMENT - HILLOCKS OF HIS
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Week 3: Otic placode appears
Week 6: Six Hillocks of His develop from mesoderm
┌─────────────────────────────────────┐
│ FIRST BRANCHIAL ARCH (3 hillocks) │
│ Hillock 1 → Tragus │
│ Hillock 2 → Helical crus │
│ Hillock 3 → Helix │
├─────────────────────────────────────┤
│ SECOND BRANCHIAL ARCH (3 hillocks) │
│ Hillock 4 → Antihelix │
│ Hillock 5 → Antitragus │
│ Hillock 6 → Lobule │
└─────────────────────────────────────┘
Week 7: Cartilage formation begins
Week 12: All hillocks fuse to form the definitive auricle
↓
IF FUSION IS INCOMPLETE OR DEFECTIVE
↓
PREAURICULAR SINUS FORMS
Two theories of formation (Scott-Brown's):
- Defective/incomplete fusion of the hillocks of His during auricular embryogenesis
- Isolated ectoderm folding - localized folding of ectoderm during auricular development
(Cummings: "When these fuse inappropriately, a preauricular sinus tract can result." - p.555)
3. INCIDENCE / EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Incidence | 5-6 per 1,000 births (Shambaugh) |
| Side | Unilateral > bilateral |
| Bilateral occurrence | 25-50% of cases |
| Sex | Slight female predominance |
| Race | Higher in Asian and African populations |
| Genetics | Autosomal dominant (bilateral more likely inherited) |
| Chromosomal locus | 8q11.1-q13.3 (Scott-Brown) |
4. ANATOMY AND PATHOLOGY
Location of opening:
- Anterior to the ascending limb of the helix (most common)
- Superior to the level of the tragus
- A pit below the tragus is more likely a first branchial cleft anomaly (K.J. Lee)
Course of the tract (Scott-Brown's):
ANATOMY OF SINUS TRACT
═══════════════════════════════════════════
Opening: Pit anterior to helical root
↓
Lined by: Stratified squamous epithelium
↓
Lies in: Subcutaneous tissue
• LATERAL to temporalis fascia (superiorly)
• LATERAL to parotid fascia (inferiorly)
• Posterior to the facial nerve and parotid gland
↓
Terminal portion: Adherent to cartilage of helix
↓
Course: Tortuous, may branch extensively
↓
May extend into: Parotid gland (rare)
═══════════════════════════════════════════
Contents of sinus: Desquamated keratin, sebaceous material, occasionally cartilaginous elements
Important anatomical relation:
- The facial nerve and parotid gland are deep/medial to the tract
- Risk of facial nerve injury in revision surgery
Clinical photo from Scott-Brown's:
 Fig 16.1 - Left preauricular sinus (Scott-Brown's) - note the small pit at the anterior margin of the helix
Fig 16.1 - Left preauricular sinus (Scott-Brown's) - note the small pit at the anterior margin of the helix
5. CLASSIFICATION
A. By Laterality:
- Unilateral - sporadic, more common
- Bilateral - more likely to be inherited
B. By Symptomatology (Dhingra/Hazarika):
- Asymptomatic - mere cosmetic blemish, no discharge
- Symptomatic - with discharge, recurrent infection, abscess
C. By S Das Classification of Sinuses:
- Congenital - e.g., preauricular sinus
- Traumatic
- Inflammatory
6. CLINICAL FEATURES
Symptoms:
- Small pit or depression at anterior margin of ascending helix
- Intermittent discharge of cheesy/purulent material from pit
- Recurrent episodes of infection/abscess
- Pain and tenderness during infected episodes
- Foul-smelling discharge
Signs:
- Visible pit/punctum anterior to helix
- Scar tissue from previous drainage (in recurrent cases)
- Surrounding skin inflammation, erythema, fluctuation (when infected)
Clinical photo - inflamed preauricular sinus:
 Fig 16.2 (Scott-Brown's) - Inflamed preauricular sinus with overlying skin erythema
Fig 16.2 (Scott-Brown's) - Inflamed preauricular sinus with overlying skin erythema
7. ASSOCIATED CONDITIONS / SYNDROMES
PREAURICULAR SINUS
│
├──► BRANCHIO-OTO-RENAL (BOR) SYNDROME (most common)
│ • Hearing loss (conductive/sensorineural/mixed)
│ • Branchial cleft cysts/fistulae
│ • Renal anomalies
│
├──► Chromosome 8q11.1-q13.3 anomaly
│
├──► CHARGE syndrome
│
├──► Townes-Brocks syndrome
│
├──► Nager syndrome
│
└──► Goldenhar syndrome (hemifacial microsomia)
Indications for Renal Ultrasound (Scott-Brown's criteria):
- Maternal history of gestational diabetes
- Family history of ear anomalies or hearing loss
- Associated craniofacial abnormalities
- Associated cardiac abnormalities
- Associated gastrointestinal abnormalities
- Associated limb abnormalities
(Scott-Brown's: "A preauricular sinus, or any other external ear abnormality, associated with any of the above findings is an indication for a renal ultrasound." - p.210)
8. DIAGNOSIS
DIAGNOSTIC FLOWCHART - PREAURICULAR SINUS
══════════════════════════════════════════
Patient presents with pit/discharge
anterior to ear
│
▼
HISTORY: Age of onset, frequency of
infections, family history, discharge
│
▼
EXAMINATION: Identify pit location,
signs of infection, swelling
│
├──► Pit at helical root
│ → Preauricular sinus (most likely)
│
└──► Pit below tragus / lower
→ Consider First Branchial Cleft Anomaly
→ Work Type I or II
│
▼
INVESTIGATIONS
│
├── Audiometry: Rule out hearing loss
│
├── Renal Ultrasound: If syndromic features
│
├── MRI/CT: In revision cases (supra-auricular
│ approach planning, extensive branching)
│
└── Culture & Sensitivity: During acute infection
══════════════════════════════════════════
Differential Diagnosis:
- First branchial cleft anomaly (Work Type I/II)
- Infected epidermoid/sebaceous cyst
- Preauricular appendage/skin tag
- Second branchial cleft cyst (lower position)
- Parotid abscess
9. TREATMENT
A. Conservative Management:
- Asymptomatic sinuses: Observation, no treatment required
- Patient education on hygiene
B. Management of Acute Infection:
- Oral/IV antibiotics (first line)
- Incision and drainage (I&D) - AVOID if possible because:
- Causes scarring and fibrosis
- Obliterates normal tissue planes
- Makes future definitive excision technically difficult (Shambaugh)
- Risk of incomplete drainage
- If I&D unavoidable: Needle aspiration preferred, with microbiological culture
- Lacrimal probe drainage described by Coatesworth et al. (2003)
C. Surgical Treatment - INDICATIONS:
INDICATIONS FOR SURGERY
═════════════════════════════
1. Recurrent infections (most common)
2. Chronicity of discharge
3. Abscess formation not responding to antibiotics
4. Unsightly skin inflammation
5. Cosmetic reasons (patient request)
═════════════════════════════
10. SURGICAL TECHNIQUES
FLOWCHART - SELECTION OF SURGICAL APPROACH:
SURGICAL MANAGEMENT OF PREAURICULAR SINUS
══════════════════════════════════════════
SURGERY INDICATED
│
┌──────────┴──────────┐
First episode Recurrent case / Complex /
/ Simple case Previous I&D / Extensive branching
│ │
▼ ▼
MICRODISSECTION SUPRA-AURICULAR APPROACH
(Standard Sinusectomy) (Preferred for recurrent/complex)
│ │
▼ ▼
• Lacrimal probe/ • Identify temporalis fascia
methylene blue to • Dissect soft tissue between
delineate tract temporalis fascia & helix
• Elliptical incision • Remain posterior to
around pit parotid fascia
• Trace all branches • Excise en bloc without
• Remove tract with formal tract identification
cartilage attachment • Include sliver of
auricular cartilage
══════════════════════════════════════════
TECHNIQUE 1: Standard Sinusectomy / Microdissection
- Elliptical incision around sinus opening
- Methylene blue dye injection to stain tract and branches
- Lacrimal probe to delineate extent
- Meticulous dissection of all branches
- Excision of tract with its attachment to helical cartilage
- Recurrence rate: 5-42% (varies by surgeon/technique)
TECHNIQUE 2: Supra-Auricular Approach (Preferred - Scott-Brown's)
- Incision placed superior and posterior to sinus opening
- Identification of temporalis fascia (key landmark)
- Dissection of soft tissue bloc between temporalis fascia and helix
- Dissection remains lateral to parotid fascia
- No attempt to formally identify all sinus branches
- En bloc excision of soft tissue with cartilage sliver
- Recurrence rate: ~5% (Leopardi review cited in Medscape)
TECHNIQUE 3: Wide Local Excision
- Wider margins of skin and subcutaneous tissue excised
- Considered to give lowest recurrence rates (Scott-Brown's)
- Care to avoid facial nerve in revision cases
Intraoperative surgical image (Scott-Brown's):
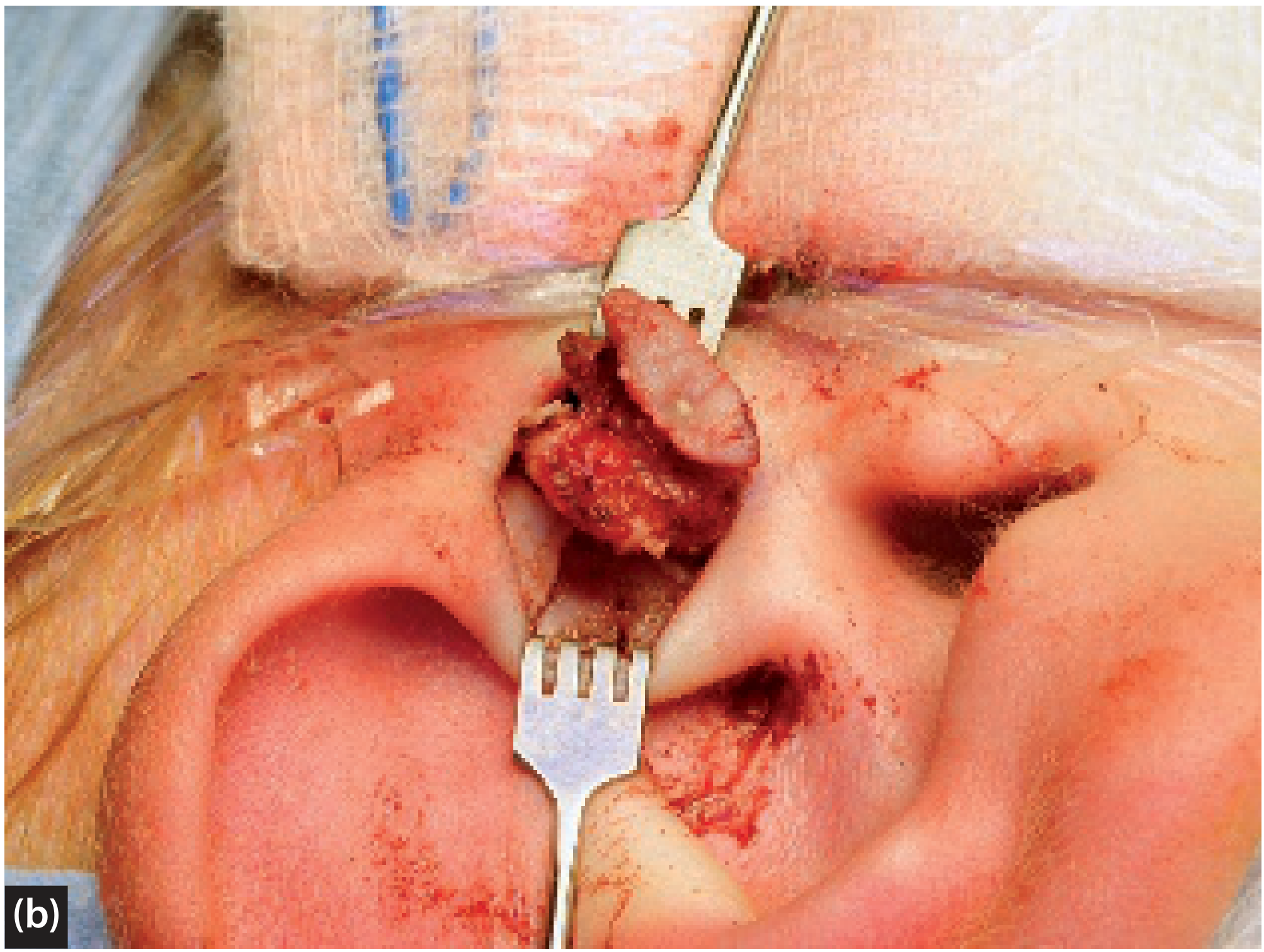 Fig 41.6b (Scott-Brown's) - Intraoperative excision of preauricular sinus cyst, tract and sliver of cartilage
Fig 41.6b (Scott-Brown's) - Intraoperative excision of preauricular sinus cyst, tract and sliver of cartilage
11. COMPLICATIONS
Operative Complications:
- Facial nerve injury - especially in revision cases; nerve lies deep/medial to tract
- Wound infection
- Hematoma
- Poor cosmesis/scarring
Post-operative Complications:
- Recurrence (most important) - varies 0-42% by technique
- Due to incomplete excision of branches
- Previous I&D causing fibrosis
- Incomplete removal of cartilage attachment
- Surgeon inexperience
Factors contributing to recurrence:
- Previous I&D (fibrosis obliterates planes)
- Inadequate removal of cartilaginous base
- Failure to identify all branches
- Active infection at time of surgery
12. COMPARISON OF TECHNIQUES
| Technique | Principle | Recurrence Rate | Best Used For |
|---|---|---|---|
| Curettage | Blind scraping | Very high (not done now) | Historically used |
| Simple sinusectomy | Trace + remove tract | 5-42% | First-time, simple |
| Microdissection + methylene blue | Dye-guided excision | Moderate | Moderate complexity |
| Supra-auricular approach | En bloc fascia-guided | ~5% | Recurrent, complex |
| Wide local excision | Wide margins | Lowest | Recurrent, inflamed |
| Microscope-assisted technique | Better visualisation | Low | Any case with magnification |
13. RELATIONSHIP TO FIRST BRANCHIAL CLEFT ANOMALY
DIFFERENTIAL: PREAURICULAR SINUS vs FIRST BRANCHIAL CLEFT ANOMALY
════════════════════════════════════════════════════════════════════
┌──────────┬──────────────────────┐
│ Feature │ Preauricular Sinus │ 1st Branchial Cleft
├──────────┼───────────────────────┤─────────────────────
│ Opening │ Anterior to helix │ Near/below tragus or
│ │ (helical root) │ external ear canal
├──────────┼───────────────────────┤─────────────────────
│ Relation │ Lateral to │ Associated with EAC,
│ to nerve │ facial nerve │ may be MEDIAL to nerve
├──────────┼───────────────────────┤─────────────────────
│ Tissue │ Ectoderm only │ Ectoderm ± mesoderm
│ type │ │ (Work Type I/II)
├──────────┼───────────────────────┤─────────────────────
│ Parotid │ Not usually involved │ May pass through
│ relation │ │ parotid gland
└──────────┴───────────────────────┴─────────────────────
(K.J. Lee's: "Pit below tragus more likely to be first branchial cleft anomaly" - p.989)
14. MANAGEMENT FLOWCHART (COMPLETE - RGUHS EXAM FORMAT)
PREAURICULAR SINUS - COMPLETE MANAGEMENT ALGORITHM
══════════════════════════════════════════════════════════════
PREAURICULAR SINUS DIAGNOSED
│
┌─────────────┴──────────────┐
ASYMPTOMATIC SYMPTOMATIC
│ │
Observe / Reassure ┌───────────┴────────────┐
Screen for BOR/ │ │
renal anomalies INFECTED DISCHARGING
│ (no infection)
┌──────────┴──────────┐
ACUTE INFECTION ABSCESS
│ │
Oral/IV Antibiotics Needle aspiration
Culture & Sensitivity + IV Antibiotics
Avoid I&D if possible (avoid I&D)
│ │
Resolution? Resolution?
┌─────┴─────┐ ┌─────┴─────┐
YES NO YES NO
│ │ │ │
Plan elective I&D + Plan I&D under GA
surgery antibiotics elective (last resort)
│ surgery
└─────────────┬──────────────┘
│
ELECTIVE SURGERY (after infection resolves)
│
┌────────────┴──────────────┐
FIRST TIME REVISION / RECURRENT
│ │
MICRODISSECTION SUPRA-AURICULAR APPROACH
(Sinusectomy) (Wide local excision)
+ Methylene blue + Temporalis fascia identification
+ Lacrimal probe + Cartilage sliver excision
│ │
└──────────────┬───────────────┘
│
POST-OP: FOLLOW-UP
Watch for: Recurrence, wound infection,
facial nerve function
══════════════════════════════════════════════════════════════
15. TEXTBOOK-SPECIFIC KEY POINTS (For RGUHS)
Scott-Brown's (Vol 2, p.210):
- Terminal portion of tract adherent to helix cartilage
- Wide local excision gives lowest recurrence
- Bilateral sinuses more likely inherited
- Chromosome 8q11.1-q13.3 implicated
- Indications for renal ultrasound clearly outlined
Cummings Otolaryngology (p.555):
- Hillocks fuse by Week 12 of intrauterine life
- Inappropriate fusion leads to preauricular sinus tract
- Concha derives from ectoderm of first branchial groove
Shambaugh's Surgery of the Ear:
- Incidence: 5-6 per 1,000 births
- Bilateral in 25-50% of cases
- "Acute I&D ideally avoided as scarring obliterates normal tissue planes"
- Surgical resection indicated when symptomatic or with recurrent infection
K.J. Lee's Essential Otolaryngology (p.989):
- Pit at helical root = preauricular sinus (hillock fusion failure)
- Pit below tragus = consider first branchial cleft anomaly
- Acute infection: antibiotics and drainage if necessary
- Definitive excision must include entire tract plus cartilage at base
- This is necessary to prevent postoperative infection and recurrence
Dhingra (Diseases of Ear Nose & Throat):
- Congenital sinus, pit-like depression near anterior margin of helix
- Lined by squamous epithelium
- Treatment: Surgical excision; antibiotics for infections
- Sinus probed with lacrimal probe and methylene blue injected before excision
Hazarika (Textbook of ENT):
- Classified as a minor congenital ear anomaly
- Incision and drainage avoided - fibrous scarring increases recurrence
- Supra-auricular excision preferred technique in Indian practice
Stell & Maran (Head & Neck Surgery):
- Preauricular sinus described as a branchial apparatus anomaly
- Complete excision with cartilage attachment essential
- Related to branchial cyst/sinus/fistula in embryological origin
Zakir Hussain (ENT for PG):
- Common in RGUHS question papers as 5/10/20 mark question
- Key points: Embryology (hillock fusion failure), Management algorithm, Supra-auricular approach, Complications
- Association with BOR syndrome regularly tested
16. RECENT ADVANCES (2021-2026)
1. Microscope-Assisted Technique (PMID: 36530819, 2022)
- Maiti et al. (J Indian Assoc Pediatr Surg, 2022)
- Retrospective comparative study: Microscope-assisted technique vs Supra-auricular approach
- Microscope-assisted technique allows better visualization of branching tracts
- Comparable outcomes to traditional supra-auricular method
- Particularly useful in complex/recurrent cases
2. Standardized Surgical Strategy to Reduce Recurrence (PMID: 37919909, 2023)
- Park et al. (Arch Craniofac Surg, 2023)
- Standardized protocol incorporating temporalis fascia identification + cartilage excision
- Histopathological analysis confirms importance of removing all epithelial lining
3. Double Elliptical Excision with Coaptation Suture (2024)
- Lee JW et al. (Int J Pediatr Otorhinolaryngol, 2024)
- Novel technique: double elliptical incision for complicated/recurrent sinuses
- Coaptation suture for better wound closure
- Pilot study showing reduced recurrence in complex cases
4. Histopathological Analysis (PMID: 39680060, 2024)
- Huang Q et al. (Ear Nose Throat J, 2024)
- Confirms tract lined by stratified squamous epithelium
- Goblet cells and sebaceous glands also found in some tracts
- Highlights need to remove all epithelial components for cure
5. Post-Helical Crus Approach (PMID: 42322723, 2026)
- Zhang H et al. (Int J Pediatr Otorhinolaryngol, 2026)
- New comparative study of post-helical crus approach for classic preauricular sinuses
- May offer better visualization and lower recurrence than traditional approach
6. Single-Stage Excision in Infected Sinus (PMID: 42391915, 2026)
- Nicholson & Levi (Int J Pediatr Otorhinolaryngol, 2026)
- Retrospective cohort: outcomes of single-stage excision even in infected preauricular sinus
- Challenges the traditional teaching of waiting for infection resolution
- Results suggest comparable outcomes to two-stage surgery
- Important paradigm shift in management
7. Mycobacterial Preauricular Sinus Abscess (PMID: 37779761, 2023)
- Unusual causative organism - highlight for atypical/non-responding cases
- Consider atypical mycobacteria in immunocompromised or non-resolving cases
17. QUICK REVISION TABLE (RGUHS Exam)
| Key Point | Detail |
|---|---|
| Embryology | Defective fusion of hillocks of His (Week 6-12) |
| Most common location | Anterior to ascending limb of helix |
| Lining | Stratified squamous epithelium |
| Bilateral percentage | 25-50% |
| Inheritance | Autosomal dominant (bilateral) |
| Chromosome | 8q11.1-q13.3 |
| Most associated syndrome | Branchio-Oto-Renal (BOR) syndrome |
| Key relation | Lateral to temporalis fascia and parotid fascia |
| Acute treatment | IV antibiotics; avoid I&D |
| Preferred surgery (recurrent) | Supra-auricular approach |
| Landmark in surgery | Temporalis fascia |
| Key to prevent recurrence | Remove entire tract + cartilage attachment |
| Common organism in infection | Staphylococcus aureus, Pseudomonas |
| Complication of surgery | Recurrence, facial nerve injury |
18. DIAGRAM - POSITION OF PREAURICULAR SINUS ON THE AURICLE
ANATOMY OF AURICLE - POSITION OF PREAURICULAR SINUS
___________
/ \
/ HELIX \
| /─────────────\
| / SCAPHA |
| | ___________ |
| | / \ |
| || ANTIHELIX | |
| || /─────\ | |
| || / CONCHA \ | |
★ PIT ← ●||| CYMBA | | |
(Opening) ||| CAVUM | | |
| \\─────────/ | |
| \ | |
| ANTITRAGUS | |
| ↑ | |
| TRAGUS | |
\ ↑ /
\___ LOBULE _/
★ = Preauricular sinus opening (ANTERIOR to helical root/ascending helix)
- Just anterior and superior to tragus
- Tract runs LATERAL to temporalis fascia
- Terminal end ADHERENT to helical cartilage
19. SUMMARY - HIGH YIELD POINTS FOR 20 MARKS
- Definition: Congenital epithelium-lined sinus tract anterior to helix
- Embryology: Failure of fusion of hillocks of His (Week 6-12); two theories
- Incidence: 5-6/1000 births; bilateral in 25-50%
- Anatomy: Pit anterior to helix; tract lateral to temporalis + parotid fascia; terminal end at helix cartilage
- Associations: BOR syndrome (most important); chromosome 8q11.1-q13.3
- Clinically: Pit, discharge, recurrent infections, abscess
- Acute management: Antibiotics; AVOID I&D (causes fibrosis, difficult future surgery)
- Surgery: Supra-auricular approach preferred for recurrence (temporalis fascia landmark)
- Recurrence prevention: Remove entire tract INCLUDING cartilage attachment
- Recent advances: Single-stage excision in infected sinus (2026), microscope-assisted technique, double elliptical excision, post-helical crus approach
References:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2, Chapter 16, p.210
- Cummings Otolaryngology Head and Neck Surgery, Chapter 28, p.555
- Shambaugh's Surgery of the Ear, Chapter 22, p.406
- K.J. Lee's Essential Otolaryngology, Chapter - Congenital, p.989
- Dhingra PL: Diseases of Ear, Nose and Throat, 7th ed.
- Hazarika P: Textbook of ENT Head and Neck Surgery
- Stell & Maran: Head and Neck Surgery, 4th ed.
- Zakir Hussain: ENT for PG
- S. Das: A Manual on Clinical Surgery, 13th ed., p.3777
- Park H et al. Arch Craniofac Surg, 2023 (PMID: 37919909)
- Nicholson OA et al. Int J Pediatr Otorhinolaryngol, 2026 (PMID: 42391915)
- Zhang H et al. Int J Pediatr Otorhinolaryngol, 2026 (PMID: 42322723)
- Lee JW et al. Int J Pediatr Otorhinolaryngol, 2024 (double elliptical excision)
- Huang Q et al. Ear Nose Throat J, 2024 (PMID: 39680060)
- Maiti AB et al. J Indian Assoc Pediatr Surg, 2022 (PMID: 36530819)
This is a shared conversation. Sign in to Orris to start your own chat.