Nephrotic vs nephritic syndrome from harrison book in notes concise form
Nephrotic vs Nephritic Syndrome
Harrison's Principles of Internal Medicine, 22E (2025)
Quick Comparison Table
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Core defect | Glomerular barrier permeability loss (podocyte injury) | Glomerular inflammation |
| Proteinuria | Heavy (>3.5 g/day) | Mild-moderate |
| Hematuria | Minimal/absent | Prominent (RBCs + RBC casts) |
| Pyuria | Absent | Present (PMN leukocytes) |
| Urinary casts | Fatty/waxy casts | RBC casts, cellular casts |
| Edema | Marked (hypoalbuminemia-driven) | Present (salt/water retention) |
| Hypertension | Present | Prominent |
| GFR/Urine output | Variable | Low (oliguria/anuria common) |
| Serum albumin | Low | Normal or mildly low |
| Cholesterol | High (hypercholesterolemia) | Usually normal |
| Complement | Variable | Often LOW (immune complex types) |
Nephritic Syndrome - Key Points
- Hematuria (with RBC casts)
- Pyuria (PMN leukocytes)
- Mild-moderate proteinuria
- Poststreptococcal GN (prototype - endocapillary proliferative GN; M-type nephritogenic streptococci; throat/skin infection preceding renal disease)
- Lupus nephritis
- IgA nephropathy
- ANCA vasculitis
- Anti-GBM disease
Nephrotic Syndrome - Key Points
- Heavy proteinuria (>3.5 g/day; foamy urine)
- Hypoalbuminemia
- Hypercholesterolemia
- Edema (generalized)
- Hypertension
- Hypercoagulability - loss of clotting factor binding proteins (treat with anticoagulants)
- Hyperlipidemia - increased CV risk (treat with lipid-lowering agents)
- Altered drug/hormone binding - e.g., loss of thyroid-binding globulin alters TFT results
- Progressive GFR loss - higher 24-h proteinuria = faster GFR decline
- Subnephrotic albuminuria = focal disease (<50% glomeruli)
- Full NS = diffuse disease (most glomeruli involved)
| Disease | Key Feature | Age Group |
|---|---|---|
| Minimal Change Disease (MCD) | Normal LM; foot process effacement on EM; T-cell cytokines (IL-13, IL-4); responds to steroids | 70-90% in children; 10-15% in adults |
| Focal Segmental Glomerulosclerosis (FSGS) | APOL1 mutations in African ancestry; second hit (infection/inflammation) → podocyte damage | Adults |
| Membranous Nephropathy | PLA2R, THSD7A antibodies | Adults |
- Diuretics for edema (avoid intravascular depletion)
- Statins for hypercholesterolemia
- Anticoagulation if hypercoagulable complications
- RAAS inhibitors + SGLT2i to reduce proteinuria and preserve GFR
Memory Hook
"Nephr-OTic = pOur Out protein" (big proteinuria, no blood) "Nephr-ITic = inflam-IT-ion" (blood + casts + inflammatory cells)
Biopsy Terminology (Harrison's)
| Term | Meaning |
|---|---|
| Focal | <50% glomeruli involved |
| Diffuse | >50% glomeruli involved |
| Segmental | Part of the glomerular tuft |
| Global | Most of the glomerulus |
| Endocapillary proliferation | Cell proliferation within capillary tuft |
| Extracapillary proliferation | Proliferation into Bowman's space (crescents) |
| Crescents | Fibrocellular collections in Bowman's space - severe disease |
| Interstitial fibrosis | Irreversible; sign of progression to kidney failure |
Gr
Create it in picture form with child examplee
Medical education infographic comparing Nephrotic Syndrome vs Nephritic Syndrome with child patient examples. Clean, colorful, easy-to-read clinical notes style poster. LEFT SIDE - NEPHROTIC SYNDROME (blue theme): - Title: "NEPHROTIC SYNDROME" with a sad puffy child cartoon (swollen eyes, swollen belly, swollen legs) - Child example: "7-year-old boy with puffy eyes in morning, swollen legs, foamy urine" - Classic cause in kids: MINIMAL CHANGE DISEASE - Key features listed with icons: * Massive Proteinuria >3.5g/day (foamy urine icon) * Hypoalbuminemia (low protein) * Pitting Edema (periorbital + legs) * Hypercholesterolemia * NO blood in urine * Urine: FATTY CASTS, no RBC casts - Memory tip: "Pour Out Protein - NO blood" RIGHT SIDE - NEPHRITIC SYNDROME (red/orange theme): - Title: "NEPHRITIC SYNDROME" with a child cartoon looking sick with red/bloody urine - Child example: "10-year-old boy, 2 weeks after sore throat, cola-colored urine, puffy face, high BP" - Classic cause in kids: POST-STREPTOCOCCAL GN - Key features listed with icons: * Hematuria - COLA/TEA colored urine (blood drop icon) * RBC Casts in urine * Mild-Moderate Proteinuria * Hypertension (prominent) * Oliguria / Low urine output * Low Complement (C3) - Memory tip: "Inflammation - BLOOD in urine" CENTER COMPARISON TABLE: Feature | Nephrotic | Nephritic Proteinuria | +++ Heavy | + Mild Hematuria | Minimal | +++ Prominent RBC Casts | Absent | Present Edema | Massive | Moderate BP | Elevated | Very High Complement | Variable | LOW Lipids | HIGH | Normal Albumin | LOW | Normal BOTTOM: Memory Hook banner: "Nephr-OTic = pOur Out protein | Nephr-ITic = Inflam-IT-ion + blood" Style: Bright medical education poster, clean fonts, cartoon child illustrations, color-coded sections, professional medical infographic look
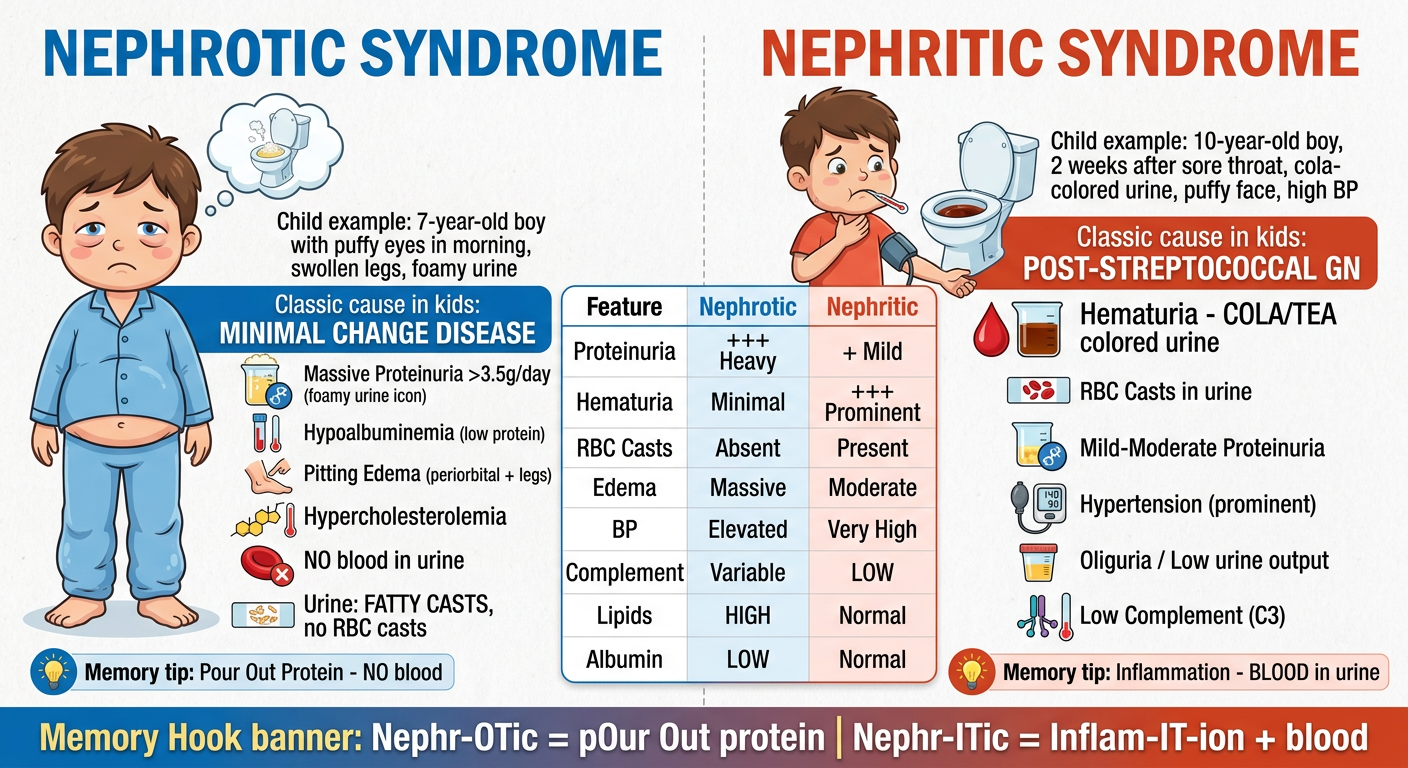
- Nephrotic (blue side): 7-year-old with puffy eyes on waking, swollen legs, foamy urine - classic Minimal Change Disease. No blood, just massive protein loss.
- Nephritic (red side): 10-year-old, 2 weeks after strep throat, cola-colored urine + high BP - classic Post-Streptococcal GN. Think inflammation, RBC casts, low C3.
Give me a 10 marks answer for UMN and LMN leison from a standard books of medicine lij manipal or harrison
UMN vs LMN Lesion - 10 Marks Answer
Source: Harrison's Principles of Internal Medicine, 22E & Neuroanatomy through Clinical Cases, 3E
Introduction
- Upper Motor Neuron (UMN): Cell bodies in layer V of the primary motor cortex (precentral gyrus, Brodmann area 4) and premotor/supplementary motor cortex. Their axons descend through the corticospinal (pyramidal) tract to synapse on lower motor neurons.
- Lower Motor Neuron (LMN): Located in the anterior horn of the spinal cord (or brainstem motor nuclei for cranial nerves). They project via peripheral nerves directly to skeletal muscle - the "final common pathway."
Anatomy of the Pathways
- 10-30% remain ipsilateral (anterior corticospinal tract)
- Direct monosynaptic connections to LMNs of hand/distal muscles (for fine motor control)
Signs and Differences
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Weakness | Yes (pyramidal pattern) | Yes (distal/segmental) |
| Muscle tone | Increased - Spasticity | Decreased - Flaccidity |
| Reflexes | Hyperreflexia (increased DTRs) | Hyporeflexia / Areflexia |
| Atrophy | None (or mild disuse atrophy) | Severe (denervation atrophy) |
| Fasciculations | Absent | Present (spontaneous motor unit discharge) |
| Babinski sign | Present (extensor plantar response) | Absent (flexor) |
| Clonus | May be present | Absent |
| Distribution | Pyramidal/regional; distal > proximal; extensors in arm, flexors in leg | Distal or segmental; follows nerve/root distribution |
| Involuntary movements | Spasms may occur | Fasciculations |
| EMG | Reduced maximal discharge frequency of motor units | Fibrillation potentials; reduced recruitment |
Note: With acute UMN lesions (e.g., spinal shock, acute stroke), there is initially flaccid paralysis with hyporeflexia - spasticity develops over hours to weeks as descending inhibitory pathways recover partially.
Pathophysiology
UMN Weakness Mechanism:
- Decreased activation of LMNs
- Distal muscles > proximal muscles affected
- Axial movements spared unless lesion is severe and bilateral
- Spasticity arises NOT from corticospinal tract damage alone but from damage to descending inhibitory pathways (reticulospinal, vestibulospinal) travelling alongside - their loss increases excitability of anterior horn motor neurons
- Corticobulbar lesions: Weakness of lower face and tongue; upper face, pharynx, and jaw muscles spared (bilateral cortical representation)
- Bilateral corticobulbar lesions: Pseudobulbar palsy - dysarthria, dysphagia, dysphonia, emotional lability, brisk jaw jerk
LMN Weakness Mechanism:
- Decrease in number of muscle fibers that can be activated
- Motor unit degeneration → fasciculations (spontaneous discharge of motor units)
- Muscle fiber denervation → fibrillation potentials (seen on EMG, not clinically visible)
- Progressive denervation atrophy
Localizing UMN Lesions
| Level | Additional Features |
|---|---|
| Cerebral cortex | Seizures, cognitive changes, contralateral hemiplegia (face + arm + leg), visual field defects |
| Internal capsule | Dense contralateral hemiplegia (pure motor stroke), face + arm + leg equally affected |
| Brainstem | "Crossed" signs - ipsilateral cranial nerve palsy + contralateral limb weakness |
| Spinal cord | Sensory level, sphincter dysfunction, bilateral signs below level; mixed UMN + LMN at level of lesion |
Localizing LMN Lesions
| Level | Features |
|---|---|
| Anterior horn (spinal cord) | Segmental weakness + atrophy + fasciculations; no sensory loss (e.g., poliomyelitis, ALS) |
| Spinal root | Radiating pain, weakness + sensory loss in root distribution, loss of reflexes |
| Peripheral nerve | Weakness + sensory loss in nerve distribution; "stocking-glove" if polyneuropathy |
Classic Examples
| Disease | Type | Key Feature |
|---|---|---|
| Stroke (cortical/capsular) | Pure UMN | Contralateral spastic hemiplegia, hyperreflexia, Babinski |
| Spinal cord compression | UMN below level | Spastic paraparesis/quadriparesis, sensory level, bladder dysfunction |
| Amyotrophic Lateral Sclerosis (ALS) | Combined UMN + LMN | UMN signs (spasticity, hyperreflexia) + LMN signs (atrophy, fasciculations) in same patient |
| Poliomyelitis | Pure LMN | Flaccid asymmetric paralysis, atrophy, areflexia, no sensory loss |
| Guillain-Barre Syndrome | LMN (peripheral) | Ascending flaccid paralysis, areflexia, sensory symptoms |
| Bell's palsy | LMN (CN VII) | Entire ipsilateral face involved (forehead + lower face) |
| UMN facial palsy (stroke) | UMN (CN VII) | Lower face only involved; forehead spared (bilateral cortical representation) |
Memory Summary
UMN = SHHHB - Spasticity, Hyperreflexia, Hypertonia, Hoffmann/Babinski, No atrophy LMN = FAFF - Flaccidity, Atrophy, Fasciculations, hyporeFlexia
Create a visual comparison poster with pathological diagrams
Medical education poster: UMN vs LMN Lesion - Visual Comparison with Pathological Diagrams. Clean, professional, colorful medical infographic style. TOP HEADER: Bold title "UPPER MOTOR NEURON vs LOWER MOTOR NEURON LESION" with subtitle "Corticospinal Tract Anatomy & Clinical Signs" CENTER ANATOMY DIAGRAM (spanning full width): A detailed anatomical diagram showing the full motor pathway from brain to muscle: - Brain (cerebral cortex, motor cortex labeled) at top - Arrow going down through Internal Capsule - Brainstem (pons, medulla) with DECUSSATION point clearly labeled at cervicomedullary junction with X crossing symbol - Spinal cord going down - RED DASHED LINE dividing: "UMN LESION above this point" on left side, "LMN LESION below anterior horn" on right side - Anterior horn cell labeled in spinal cord - Peripheral nerve going to muscle at bottom - Lightning bolt symbols showing where lesions occur: one in cortex/internal capsule area (UMN), one at anterior horn/peripheral nerve (LMN) LEFT PANEL - UMN LESION (red/orange color theme): Title: "UMN LESION" with brain icon Lesion sites listed: Cortex, Internal Capsule, Brainstem, Spinal Cord Clinical Signs with icons: - SPASTICITY (increased tone) - spring/coil icon - HYPERREFLEXIA - hammer icon with upward arrow - BABINSKI SIGN POSITIVE - foot with upward toe arrow - NO ATROPHY (or mild disuse) - NO FASCICULATIONS - Weakness: Pyramidal pattern (extensors arm, flexors leg) - Clonus present Small muscle diagram showing: Normal bulk, stiff appearance Example diseases box: Stroke, MS, Cord compression, Cerebral palsy RIGHT PANEL - LMN LESION (blue/green color theme): Title: "LMN LESION" with spinal cord/nerve icon Lesion sites listed: Anterior horn, Nerve root, Peripheral nerve Clinical Signs with icons: - FLACCIDITY (decreased tone) - limp muscle icon - HYPOREFLEXIA / AREFLEXIA - hammer icon with downward arrow - BABINSKI ABSENT (flexor plantar) - ATROPHY - shrunken muscle diagram - FASCICULATIONS - twitching muscle waves icon - Weakness: Distal/segmental pattern - NO Clonus Small muscle diagram showing: Wasted, atrophied muscle Example diseases box: Polio, GBS, ALS (LMN component), Bell's palsy COMPARISON TABLE at bottom: | Feature | UMN | LMN | | Tone | Spastic UP arrow | Flaccid DOWN arrow | | Reflexes | Hyper UP | Hypo/Absent DOWN | | Atrophy | None | Severe | | Fasciculations | No | Yes | | Babinski | Positive checkmark | Negative X | | Distribution | Pyramidal | Segmental/Distal | SPECIAL BOX: "ACUTE UMN LESION = Initially FLACCID (spinal shock) - spasticity develops later over weeks" SPECIAL BOX: "ALS = COMBINED UMN + LMN signs in same patient" MEMORY AID banner at bottom: "UMN = SHHHB (Spasticity, Hyperreflexia, Hypertonia, Hoffmann/Babinski, No atrophy) | LMN = FAFF (Flaccidity, Atrophy, Fasciculations, hyporeFlexia)" Style: Bright medical textbook illustration style, color-coded panels, anatomical accuracy, clean sans-serif fonts, professional medical poster layout
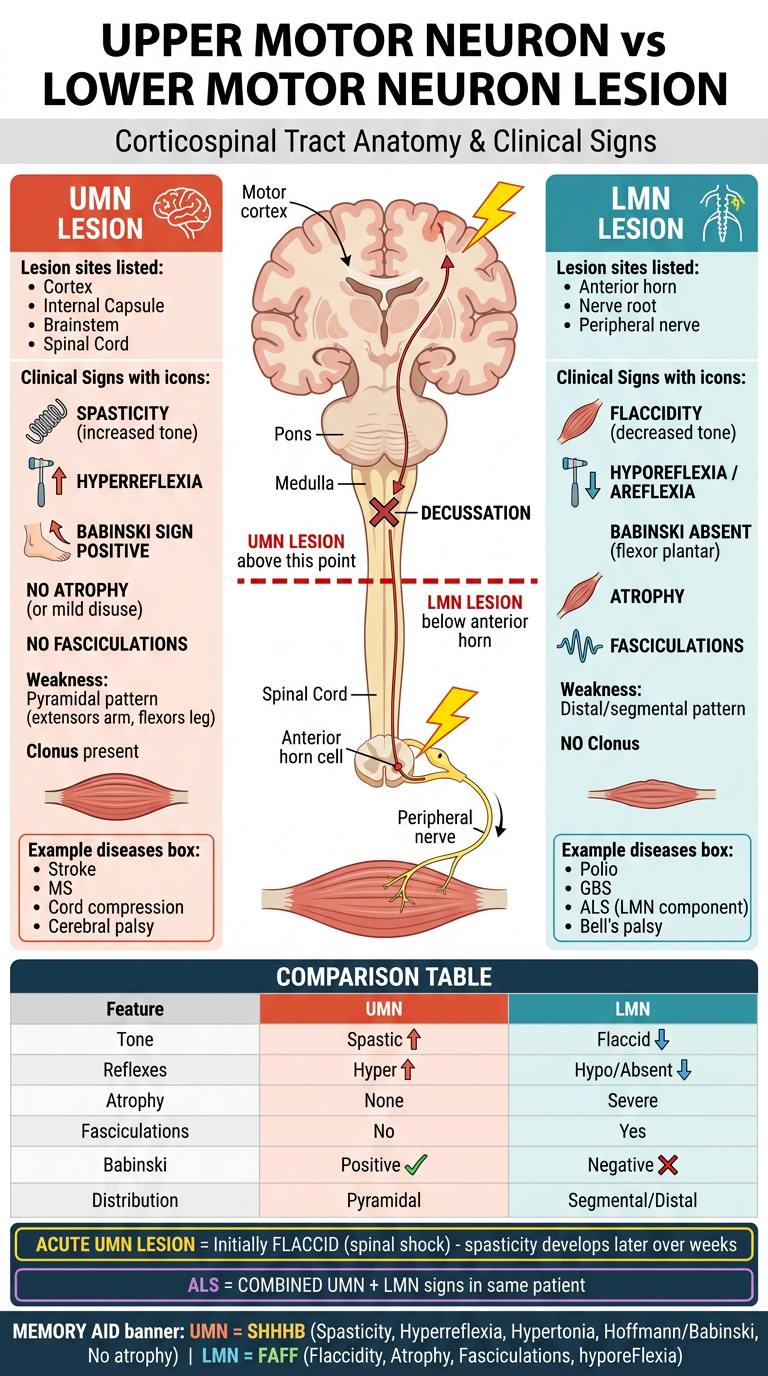
- Acute UMN lesion starts as flaccid (spinal shock) - spasticity comes later
- ALS has both UMN + LMN signs simultaneously - a classic exam point