I now have extremely rich, comprehensive data from multiple authoritative textbooks. Let me compose the full MBBS-level burns guide.
Burns - Complete MBBS Guide
From Basic Science to Clinical Management
1. ANATOMY RELEVANT TO BURNS
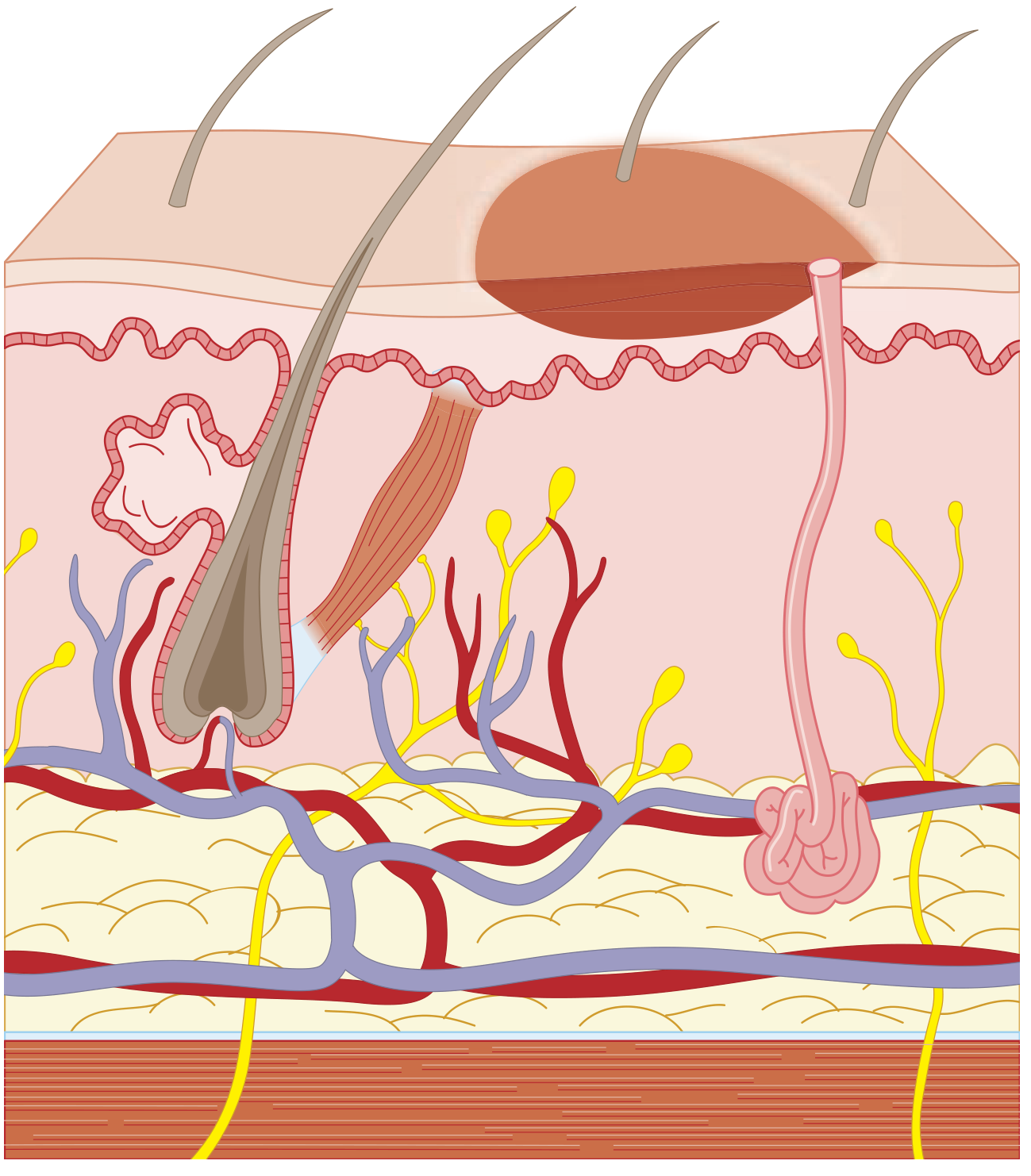
The skin has two main layers:
- Epidermis - avascular, composed of stratified squamous epithelium (keratinocytes). Regeneration occurs from the basal layer and skin appendages (hair follicles, sweat glands).
- Dermis - vascular, contains collagen, elastin, sweat glands, sebaceous glands, and hair follicles. Divided into:
- Papillary dermis (superficial) - thin, loosely organized
- Reticular dermis (deep) - thick, densely organized
- Subcutaneous tissue (hypodermis) - fat and connective tissue
- Deep structures - fascia, muscle, periosteum, bone
The depth of burn injury through these layers forms the basis of classification.
2. DEFINITION & ETIOLOGY
A burn is tissue injury caused by:
- Thermal - flame, scalds (hot liquids/steam), contact with hot objects
- Chemical - acids (coagulation necrosis), alkalis (liquefaction necrosis - deeper, more dangerous)
- Electrical - low voltage (<1000V) or high voltage (>1000V); injury follows path of least resistance (nerves, blood vessels)
- Radiation - UV light (sunburn), ionizing radiation
- Friction - road rash, abrasion burns
3. BURN DEPTH CLASSIFICATION
This is the most important basic science concept and forms the backbone of management decisions.
| Degree | Old Term | Depth | Appearance | Sensation | Healing |
|---|
| 1st degree | Superficial | Epidermis only | Red, dry, no blisters | Painful | 7 days, no scar |
| 2nd degree - superficial partial thickness | Partial thickness | Epidermis + papillary dermis | Blisters, red/moist, brisk capillary refill | Very painful | 14-21 days, minimal scar |
| 2nd degree - deep partial thickness | Partial thickness | Epidermis + reticular dermis | Pale/white/yellow, no capillary refill, may blister | Decreased pain (nerve damage) | 3 weeks to 2 months, significant scarring |
| 3rd degree | Full thickness | All skin layers + appendages | Dry, leathery, white/brown/charred, depressed | Painless (destroyed nerves) | Does NOT self-heal; needs grafting |
| 4th degree | Deep full thickness | Down to muscle/bone/tendon | Charred, black | Painless | Amputation often needed |
From Schwartz's Surgery 11e: "Burn wounds are commonly classified as superficial (first-degree), partial-thickness (second-degree), full-thickness (third-degree), and fourth-degree based on the original burn depth classification by Dupuytren in 1832."
From Tintinalli's Emergency Medicine: Deep partial-thickness burns "extend into the deep dermis (reticular layer). Hair follicles and sweat and sebaceous glands are damaged, but their deeper portions usually survive. Hot liquids (e.g., oil or grease), steam, or flame usually cause this type of injury. The burned area does not blanch; it has absent capillary refill and absent pain sensation."
Key clinical pearl: Superficial burns (1st degree) are NOT included in TBSA calculations for fluid resuscitation purposes.
4. ESTIMATING BURN AREA - TBSA (Total Body Surface Area)
Rule of Nines (Wallace's Rule of Nines) - Adults
| Body Region | %TBSA |
|---|
| Head and neck | 9% |
| Each upper limb | 9% |
| Anterior trunk | 18% |
| Posterior trunk | 18% |
| Each lower limb | 18% |
| Perineum/genitalia | 1% |
| Total | 100% |
Lund and Browder Chart
- More accurate than Rule of Nines, especially in children, because it accounts for age-related changes (head larger, legs smaller in infants).
- From Sabiston Surgery: The Berkow Formula (similar principle) adjusts head from 19% at birth to 7% in adults, and thighs from 5.5% at birth to 9.5% in adults.
Palmar Method
- Patient's palm (including fingers) = approximately 1% TBSA - useful for patchy/scattered burns.
Galveston Formula (Children)
For pediatric fluid resuscitation: 5000 mL/m² per %TBSA burn + 1500 mL/m² TBSA for maintenance in first 24 hours.
5. BURN SEVERITY CLASSIFICATION (ABA - American Burn Association)
| Severity | Criteria | Management |
|---|
| Minor | Partial thickness <15% TBSA (adults), <10% TBSA (children/elderly), full thickness <2% | Outpatient |
| Moderate | Partial thickness 15-25% (adults), 10-20% (children/elderly); full thickness ≤10% | Hospital admission |
| Major | Partial thickness >25% (adults), >20% (children/elderly); full thickness >10%; burns of face/hands/feet/perineum; circumferential burns; electrical burns; inhalation injury; burns + trauma | Burn center |
6. PATHOPHYSIOLOGY
Local Response - Jackson's Zones of Burns (1953)
Three concentric zones from center outward:
- Zone of Coagulation (center) - irreversible cell death, no blood flow, no viable tissue
- Zone of Stasis - potentially viable tissue with decreased perfusion; can be salvaged or may progress to necrosis if not resuscitated properly
- Zone of Hyperemia (periphery) - vasodilatation, increased blood flow, fully recovers
Clinical implication: Aggressive fluid resuscitation is aimed at preserving the zone of stasis.
Systemic Response
Large burns (>20% TBSA) trigger a massive systemic inflammatory response:
Cardiovascular:
- Fluid shifts from intravascular to interstitial (burn edema) due to release of inflammatory mediators (histamine, prostaglandins, bradykinin, oxygen free radicals)
- Decreased cardiac output, increased peripheral vascular resistance
- "Burn shock" - distributive + hypovolemic
Metabolic (Hypermetabolic State):
- Basal metabolic rate increases up to 200% (Schwartz's Surgery 11e)
- Marked protein catabolism and muscle wasting
- Hyperglycemia common, insulin resistance
- Persistent for months after injury
Immunological:
- Skin barrier disruption leads to infection risk
- Systemic immunosuppression
- Increased susceptibility to sepsis
7. INITIAL EVALUATION AND EMERGENCY MANAGEMENT
Primary Survey (ABCDE)
A - Airway
- Most critical priority. Inhalation injury can cause rapid, severe airway edema.
- Warning signs: hoarse voice, stridor, wheezing, subjective dyspnea, oropharyngeal mucosal burns
- From Schwartz's 11e: "Perioral burns and singed nasal hairs alone do not indicate upper airway injury, but are signs that the oral cavity and pharynx should be evaluated for mucosal injury."
- Early elective orotracheal intubation if any concern - do not wait for complete obstruction
B - Breathing
- 100% oxygen via non-rebreather mask for all burn patients
- Mandatory for CO poisoning treatment
- Check for circumferential chest burns - may need escharotomy
C - Circulation
- IV access (2 large-bore IVs, preferably through unburned skin)
- Start fluid resuscitation
- Estimate TBSA and begin Parkland formula
D - Disability
- Neurological status, screen for CO/cyanide poisoning
E - Exposure/Environment
- Remove all clothing and jewelry
- Stop the burning process (cool water for 20 minutes for thermal burns)
- Prevent hypothermia (especially in children)
8. INHALATION INJURY
A major independent predictor of mortality - increases mortality significantly even in small burns.
Three Types:
- Upper airway (supraglottic) injury - direct thermal injury; causes edema and obstruction
- Lower airway (infraglottic) injury - chemical injury from toxic combustion products; causes tracheobronchitis, bronchospasm, mucosal sloughing
- Systemic toxin injury - CO and cyanide poisoning
Carbon Monoxide (CO) Poisoning
- CO has 200-250x greater affinity for hemoglobin than oxygen (forms carboxyhemoglobin)
- Also inhibits cytochrome oxidase (mitochondrial toxicity), uncouples oxidative phosphorylation
- Pulse oximetry is falsely normal - must check arterial blood gas with co-oximetry
- Symptoms: headache, confusion, coma, cardiac arrhythmias
- Treatment: 100% normobaric O₂ (reduces CO half-life from 250 minutes to 40-60 minutes)
- Hyperbaric O₂: controversial; logistically difficult in major burns
Cyanide Poisoning (from burning plastics, synthetics)
- Inhibits cytochrome c oxidase - blocks oxidative phosphorylation
- Features: severe lactic acidosis, neurological symptoms, pulmonary edema, ST changes on ECG
- Classic signs (bitter almond breath, cherry-red skin) are unreliable - do not rely on them
- Treatment: Hydroxocobalamin (first-line, rapidly complexes with cyanide) + sodium thiosulfate + 100% O₂
9. FLUID RESUSCITATION
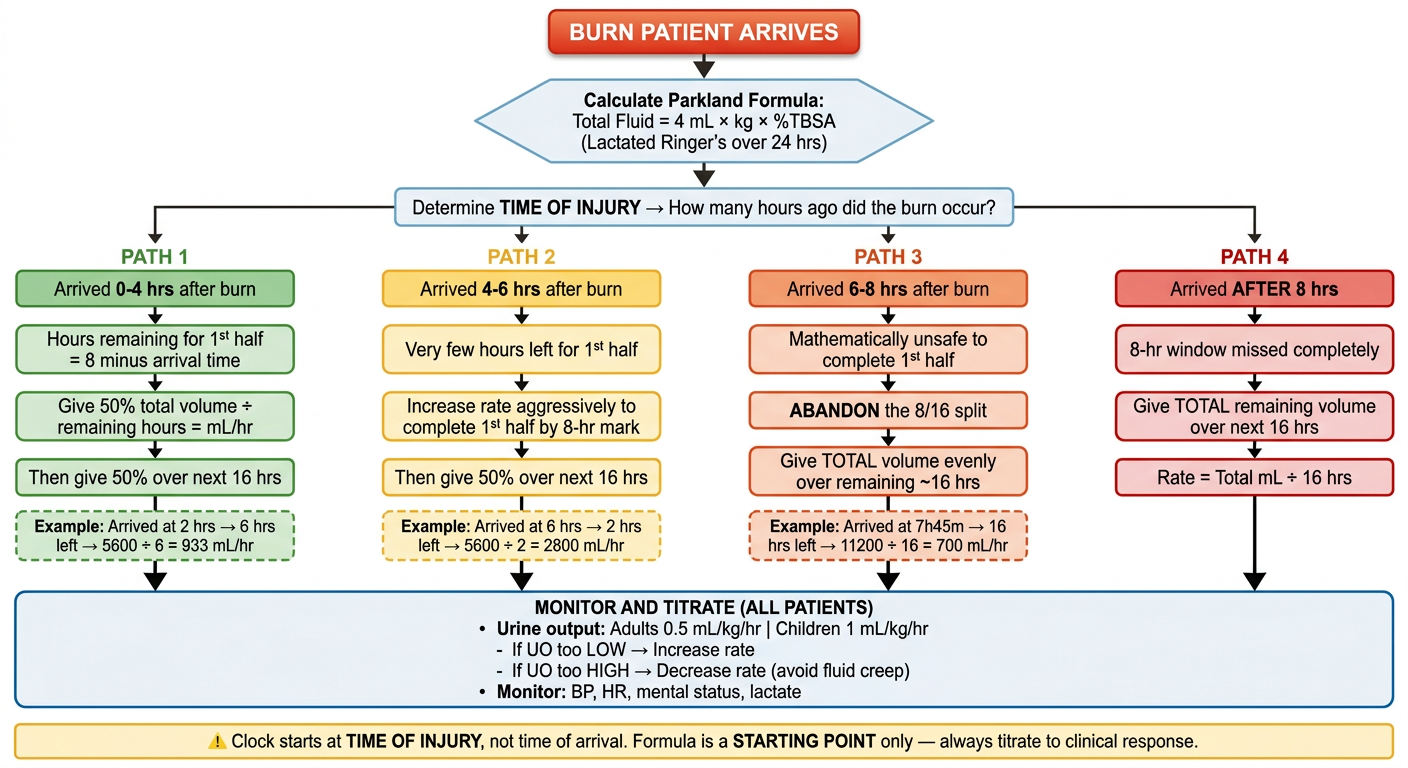
Parkland Formula (Baxter Formula) - Most Widely Used
Total fluid in first 24 hours = 4 mL × weight (kg) × %TBSA burned
- Fluid type: Lactated Ringer's (Normal Saline acceptable)
- Half (50%) given in first 8 hours from time of injury (not time of arrival!)
- Remaining half given over next 16 hours
- In children <2 years: 5% dextrose in LR (to prevent hypoglycemia)
Example: 70 kg adult with 40% TBSA burn
- Total = 4 × 70 × 40 = 11,200 mL over 24 hours
- First 8 hours: 5,600 mL (or ~700 mL/hr)
- Next 16 hours: 5,600 mL (or ~350 mL/hr)
From Tintinalli's EM: "Fluid resuscitation guided by the Parkland formula is only a rough starting point...monitor and adjust according to individual patient response."
Modified Brooke Formula (ABA Consensus Formula)
- 2-3 mL × kg × %TBSA of LR in first 24 hours (less fluid, reduce "fluid creep")
- Increasingly preferred
Monitoring Adequacy of Resuscitation
- Urine output is the gold standard endpoint:
- Adults: 0.5 mL/kg/hr (30-50 mL/hr)
- Children: 1 mL/kg/hr
- Other markers: Blood pressure, heart rate, mental status, lactate clearance
"Fluid Creep"
A major complication - over-resuscitation common in burn care. Leads to abdominal compartment syndrome, pulmonary edema, extremity compartment syndrome.
10. WOUND CARE & DRESSINGS
First Aid
- Cool running water for 20 minutes (not ice water - causes vasoconstriction and hypothermia)
- Remove clothing, rings, and constricting items
Wound Cleaning
- Gentle cleaning with chlorhexidine or dilute povidone-iodine
- Blister management: small intact blisters may be left; large blisters or those over joints are typically deroofed
Topical Antimicrobials
| Agent | Advantages | Disadvantages |
|---|
| Silver sulfadiazine (SSD) | Broad spectrum, painless application | Eschar formation, pseudoeschar, sulfa allergy, methemoglobinemia |
| Mafenide acetate | Penetrates eschar, good for ear burns | Painful, metabolic acidosis (carbonic anhydrase inhibition) |
| Silver nitrate | Very broad spectrum | Electrolyte disturbances (hyponatremia), stains |
| Bacitracin/neomycin | Good for facial burns, superficial burns | Limited depth penetration |
| Cerium nitrate-SSD | Improved antimicrobial spectrum | Limited availability |
Modern Wound Dressings
- Biological dressings: cadaveric allograft (gold standard temporary cover), xenograft (porcine skin)
- Biosynthetic: Biobrane, Integra (dermal regeneration template)
- Silver-impregnated dressings: Mepilex Ag, Aquacel Ag
11. ESCHAROTOMY
Indication: Circumferential full-thickness burns of extremities or chest causing:
- Extremity compartment syndrome (tense swelling, absent pulses, pallor, pain on passive stretch)
- Chest: inadequate ventilation due to restricted chest wall expansion
Technique: Longitudinal incisions through the eschar (not fascia) along medial and lateral surfaces of limb. For chest: bilateral anterior axillary line incisions ± subcostal transverse connection.
Fasciotomy: Required when escharotomy is insufficient or in electrical burns (deeper injury); involves incision of fascia.
12. SURGICAL MANAGEMENT
Early Excision and Grafting
- Modern standard of care for deep partial-thickness and full-thickness burns
- Early tangential excision (within 48-72 hours) improves outcomes: reduced infection, reduced hospital stay, reduced mortality
- Split-thickness skin graft (STSG) is the standard coverage
- Donor site: thighs, back, scalp
- Meshed grafts expand coverage; meshing ratio typically 1:1.5 to 1:4
Wound Coverage Options
- Autograft (patient's own skin) - definitive, permanent
- Allograft (cadaveric skin) - temporary biological dressing, immunologically rejected in 2-3 weeks
- Xenograft (porcine skin) - temporary biological dressing
- Cultured Epithelial Autograft (CEA) - cultured from patient's own keratinocytes; used for massive burns where donor sites are limited
- Integra (artificial dermis) - bovine collagen + chondroitin sulfate matrix covered with silicone; two-stage process
13. BURN INFECTIONS AND SEPSIS
Burn wound infection is the leading cause of morbidity and mortality in surviving burn patients.
Common Organisms
- Early (<5 days): Gram-positive (S. aureus, Streptococcus)
- Late: Gram-negative (Pseudomonas aeruginosa - most common and feared; Klebsiella, E. coli)
- Fungal: Candida, Aspergillus (especially in prolonged hospitalization)
Diagnosis
- Burn wound biopsy with quantitative culture: >10⁵ organisms/gram of tissue = wound infection
- Systemic signs: fever, tachycardia, leukocytosis - unreliable (common in burns without infection)
- Conversion of partial-thickness to full-thickness wound is a key sign
Systemic sepsis criteria in burns (ABA definition):
Temperature >39°C or <36.5°C, heart rate >110 bpm, respiratory rate >25 or ventilation >12 L/min, thrombocytopenia (<100,000) after day 3 - plus documented infection source.
14. COMPLICATIONS OF BURNS
Early Complications
| Complication | Mechanism | Management |
|---|
| Hypovolemic/burn shock | Fluid shifts, capillary leak | Aggressive fluid resuscitation |
| Airway obstruction | Edema, inhalation injury | Early intubation |
| Acute Tubular Necrosis | Myoglobinuria (electrical), hypovolemia | Forced alkaline diuresis, mannitol |
| Ileus/Curling's ulcer | Stress ulcer of stomach/duodenum | NG tube, PPI/H2 blockers prophylaxis |
| Hypoglycemia (children) | Depleted glycogen stores | Dextrose in IV fluids |
| Compartment syndrome | Circumferential burns, fluid edema | Escharotomy/fasciotomy |
| Carbon monoxide poisoning | Smoke inhalation | 100% O₂ |
| ARDS | Inhalation injury, sepsis | Lung-protective ventilation (6 mL/kg tidal volume) |
Late Complications
| Complication | Features |
|---|
| Hypertrophic scar | Raised, red, pruritic scars within wound margins; collagen overproduction |
| Keloid | Extends beyond wound margins; more in dark skin |
| Contractures | Limit joint ROM; common at elbow, shoulder, wrist, ankle. Tx: physiotherapy, pressure garments, surgical release |
| Heterotopic ossification | Lamellar bone in soft tissue; 1-3% incidence; risk factors: >30% TBSA, arm burns, prolonged ventilation |
| PTSD/Depression | Up to 38% of burn patients |
| Marjolin's ulcer | Squamous cell carcinoma arising in chronic burn scar; latency 20-30 years |
15. SPECIAL TYPES OF BURNS
Electrical Burns
- Entry and exit wounds - entry usually small, dry, charred; exit wound larger (explosive)
- Deep injury along path of least resistance (nerves, vessels, muscles)
- Massive internal injury with deceptively small surface area
- Cardiac arrhythmias (immediate ECG monitoring mandatory)
- Myoglobinuria - from massive rhabdomyolysis; causes acute kidney injury; treat with:
- Aggressive IV fluids to maintain urine output 1-2 mL/kg/hr (higher than thermal burns)
- Urinary alkalinization (sodium bicarbonate)
- Mannitol
- Cataract - delayed complication of high-voltage electrical burns (especially head and neck entry)
- Tetanic muscle contractions can cause spinal fractures
Chemical Burns
- Acid burns: coagulation necrosis - forms a protective eschar that limits depth
- Alkali burns: liquefaction necrosis - more dangerous, continues to penetrate deeper
- Treatment: Copious irrigation with water (minimum 20-30 minutes) - DO NOT neutralize (exothermic reaction causes additional injury)
- Hydrofluoric acid (HF): unique - forms insoluble calcium salts; causes systemic hypocalcemia → life-threatening cardiac arrhythmias; treat with topical/injected calcium gluconate
- Phenol burns: systemic absorption causes CNS toxicity; dilute with water, use polyethylene glycol
- White phosphorus: spontaneously ignites in air; keep covered with water, remove under water
Radiation Burns
- UV (sunburn): treated as superficial/first-degree burn
- Ionizing radiation: delayed presentation, progressive tissue damage; no standard antidote
Tar/Asphalt Burns
- Cool with cold water immediately
- Remove with lipid-based solvents (e.g., mineral oil, butter) - do NOT pull off hot tar
Scald Burns (Scalds)
- Most common in children and elderly
- Hot liquids: superficial partial-thickness pattern ("splash/drip" pattern)
- Immersion scalds: uniform, stocking/glove distribution - raises suspicion of non-accidental injury (NAI)
16. NUTRITION IN BURNS
The hypermetabolic response is most severe in burn patients of all surgical conditions:
- Metabolic rate increases up to 200% of baseline
- Early enteral nutrition (within 6-12 hours) is the standard: reduces catabolism, lowers infection rate, prevents ileus
- Caloric calculation: Curreri formula = 25 kcal/kg/day + 40 kcal × %TBSA/day
- Protein: 1.5-2.5 g/kg/day
- Glutamine supplementation: reduces infectious complications
- Micronutrients: Vitamins C, E; zinc, selenium, copper support wound healing
- β-blockers (propranolol): attenuate hypermetabolism, reduce heart rate, decrease catabolism - especially in pediatric burns
- Oxandrolone (anabolic steroid): improves lean body mass, reduces length of stay, used in major burns
- Strict glucose control: hyperglycemia worsens outcomes; target 100-150 mg/dL
17. PROGNOSIS - BAUX SCORE
Baux Score = Age + %TBSA burned
- Score >100: historically associated with ~50% mortality
- Score >140: very high mortality
Revised Baux Score = Age + %TBSA + 17 (if inhalation injury present)
LD₅₀ (lethal dose for 50% mortality) has dramatically improved with modern care - from 30% TBSA in 1950s to >80% TBSA in current burn centers for young patients.
18. BURN CENTER REFERRAL CRITERIA (ABA)
Transfer to a specialized burn center is indicated for:
- Partial-thickness burns >10% TBSA
- Burns involving face, hands, feet, genitalia, perineum, or major joints
- Full-thickness (3rd degree) burns at any size
- Electrical burns (including lightning)
- Chemical burns
- Inhalation injury
- Burns in patients with preexisting medical conditions
- Burns with concomitant trauma
- Burns in children at hospitals without pediatric expertise
- Burns in patients requiring special social/emotional/rehabilitative intervention
19. PEDIATRIC BURNS - KEY DIFFERENCES
- Head = larger proportion of TBSA (9% at 1 year vs 7% in adult) - adjust with Lund-Browder
- Greater risk of hypothermia (larger surface-to-volume ratio)
- Greater risk of hypoglycemia (use D5LR in children <2 years)
- Galveston formula for fluid resuscitation
- Non-accidental injury (NAI/child abuse) must always be considered:
- Symmetric stocking/glove scald distribution
- Delay in seeking treatment
- History inconsistent with injury pattern
- Multiple injuries at different stages of healing
20. REHABILITATION
- Early physiotherapy and splinting to prevent contractures
- Pressure garments: worn 23 hours/day for 12-18 months to reduce hypertrophic scarring
- Silicone gel sheets: reduce scar thickness and erythema
- Laser therapy for scar remodeling
- Psychological support: CBT, EMDR for PTSD
- Contracture release surgery when joints are functionally limited
- Return to work/school as early as possible (most patients recover function)
QUICK SUMMARY TABLE
| Topic | Key Fact |
|---|
| 1st degree | Epidermis only, heals in 7 days, not included in TBSA |
| 2nd degree superficial | Epidermis + papillary dermis, painful, blistered, heals 14-21 days |
| 2nd degree deep | Epidermis + reticular dermis, pale, painless, may need grafting |
| 3rd degree | Full thickness, leathery, painless, NEEDS grafting |
| Rule of Nines | 9-18-1 for adults; use Lund-Browder for children |
| Parkland formula | 4 mL × kg × %TBSA; half in first 8 hrs (from injury time!) |
| Urine output target | 0.5 mL/kg/hr adults; 1 mL/kg/hr children |
| CO poisoning | SpO₂ falsely normal; treat with 100% O₂ |
| Cyanide | Lactic acidosis; treat with hydroxocobalamin |
| Electrical burns | Myoglobinuria, rhabdomyolysis, cardiac arrhythmias, entry/exit wounds |
| Chemical burns | Copious water irrigation; NEVER neutralize |
| HF acid | Systemic hypocalcemia; calcium gluconate treatment |
| Zone of stasis | Target of resuscitation - can be salvaged |
| Baux score | Age + %TBSA (+17 if inhalation injury) |
| Marjolin's ulcer | SCC in chronic burn scar, 20-30 years latency |
| Curling's ulcer | Stress gastric ulcer; prevent with PPI/H2 blockers |
Sources: Schwartz's Principles of Surgery 11e; Sabiston Textbook of Surgery; Bailey and Love's Surgery 28e; Tintinalli's Emergency Medicine; Morgan & Mikhail's Clinical Anesthesiology 7e; Miller's Anesthesia 10e