Advanced coronary heart disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"coronary artery disease"[MeSH Terms] AND "advanced" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have rich textbook content. Let me compile the comprehensive answer.
Advanced Coronary Heart Disease (CHD)
Advanced coronary heart disease refers to severe, often multivessel or left main atherosclerotic disease of the epicardial coronary arteries, causing persistent myocardial ischemia, reduced left ventricular function, refractory angina, or prior MI. Management spans aggressive secondary prevention, anti-ischemic pharmacotherapy, revascularization decisions (PCI vs. CABG), and - when all else fails - alternative therapies.
1. Definition and Pathophysiology
Advanced CHD encompasses:
- Left main coronary artery disease (LMCAD) - stenosis ≥50% in the left main trunk, threatening perfusion of the majority of LV myocardium
- Three-vessel disease (3VD) - obstructive stenoses in all three major epicardial arteries (LAD, LCx, RCA)
- Two-vessel disease with proximal LAD involvement - significant stenosis of the proximal LAD plus one other vessel
- Chronic total occlusion (CTO) - complete obstruction of one or more vessels
- LV systolic dysfunction (EF <35-40%) from ischemic cardiomyopathy
Underlying biology: the plaque causing the most severe chronic stenosis is not necessarily the one that will subsequently rupture to cause an acute coronary syndrome; however, the extent and severity of coronary stenoses are potent predictors of the likelihood of critical plaque rupture somewhere in the epicardial circulation.
- Goldman-Cecil Medicine, p. 632
2. Clinical Presentation
Advanced CHD can present as:
- Stable exertional angina (classic) - graded by CCS class
- Dyspnea, fatigue, and reduced exercise tolerance as anginal equivalents, particularly in elderly patients (>80 years) and diabetics
- Asymptomatic/silent ischemia - common with sedentary lifestyle or autonomic neuropathy
- Acute coronary syndromes (NSTEMI, STEMI) when a vulnerable plaque ruptures
- Ischemic heart failure - reduced EF from repeated ischemia or infarction
Braunwald's Heart Disease notes that older adults (especially >80 yrs) are less likely to report exertional angina and more likely to report shortness of breath, fatigue, or even altered mentation as presenting features of myocardial ischemia.
3. Risk Stratification and Diagnosis
Noninvasive Testing
| Test | Role |
|---|---|
| Stress ECG (ETT) | Functional capacity, symptoms, risk; may be non-diagnostic |
| Stress echocardiography / stress SPECT/PET | Ischemia extent and severity, LVEF, MACE risk |
| Cardiac MRI stress perfusion | High accuracy for ischemia, viability assessment |
| Coronary CTA (CCTA) | Anatomical stenosis, plaque characterization |
| CCTA with CT-FFR | Functional significance of stenoses on CTA |
From the PROMISE trial (n=10,003): over 25 months, anatomical testing (CCTA) vs. functional stress testing had no difference in death, MI, or major procedural complications (3.3% vs. 3.0%), supporting a conservative strategy when patient preference is to avoid procedures.
From the ISCHEMIA trial (n=5179, patients with moderate-to-severe ischemia): over 3.2 years, an invasive strategy (coronary angiography + revascularization) vs. conservative strategy (optimal medical therapy) showed no difference in CV death or MI. However, patients randomized to the invasive strategy had better quality of life, especially if more symptomatic at baseline.
- Braunwald's Heart Disease, p. (Braunwald's block 13)
Invasive Assessment
-
Invasive coronary angiography (ICA) is recommended for patients with stable chest pain and obstructive CAD who have moderate-to-severe ischemia despite guideline-directed medical therapy (GDMT)
-
FFR (fractional flow reserve) or iFR (instantaneous wave-free ratio) is recommended for patients referred for ICA without prior stress testing to determine hemodynamic significance of lesions
-
A CCTA-defined stenosis ≥50% in the left main, FFR-CT ≤0.80, or severe stenosis ≥70% in all 3 main vessels warrants ICA for therapeutic decision-making
-
Fuster and Hurst's The Heart, 15th ed.
4. Comprehensive Medical Management
4a. Disease-Modifying Pharmacotherapy (Mortality Benefit)
Three drug classes have demonstrated mortality reduction in patients with chronic ischemic heart disease and preserved LV function:
| Drug Class | Key Points |
|---|---|
| Antiplatelet agents (Aspirin 81-325 mg/day) | Standard for all patients; clopidogrel if aspirin contraindicated/intolerant |
| ACE inhibitors / ARBs | Reduce all-cause mortality, MI, and stroke; especially beneficial with reduced EF, hypertension, or diabetes |
| High-intensity statins | Atorvastatin up to 80 mg or rosuvastatin up to 40 mg; target LDL <70 mg/dL (US) or <55 mg/dL (European) |
Additional lipid-lowering:
- Ezetimibe added to statins further reduces events in post-ACS patients even when LDL is 50-100 mg/dL
- PCSK9 inhibitors (evolocumab, alirocumab) can reduce LDL by ~60%, effective for residual elevated LDL despite statins ± ezetimibe
- Icosapent ethyl (IPE) - pure EPA omega-3 - significantly reduces cardiovascular death, MI, and stroke when added to statins in patients with well-controlled LDL but elevated triglycerides (135-500 mg/dL)
Diabetes and CAD:
-
In patients with type 2 diabetes: SGLT2 inhibitors (e.g., empagliflozin, dapagliflozin) or GLP-1 receptor agonists (e.g., semaglutide, liraglutide) reduce cardiac events independently
-
Goldman-Cecil Medicine, p. 632-633
4b. Anti-Anginal / Anti-Ischemic Therapy (Symptom Benefit, No Mortality Benefit in Stable CHD)
These drugs reduce ischemia and angina but have not been shown to reduce mortality in stable chronic ischemic heart disease:
| Drug | Mechanism | Notes |
|---|---|---|
| Beta-blockers | Reduce HR, contractility, MVO2 | First-line; especially post-MI or with LV dysfunction |
| Calcium channel blockers | Vasodilation, reduce HR (non-DHP) | Alternative or add-on if beta-blockers fail or contraindicated |
| Long-acting nitrates | Venodilation, reduce preload and angina | Require nitrate-free interval (6-8 hrs) to prevent tolerance |
| Sublingual nitroglycerin | Rapid symptom relief | For acute anginal episodes |
| Ranolazine | Late sodium channel inhibitor; reduces intracellular Ca2+ overload | Add-on anti-anginal; no mortality benefit; useful in refractory symptoms |
The management algorithm (depicted below) integrates these therapies in a stepwise fashion before considering revascularization:
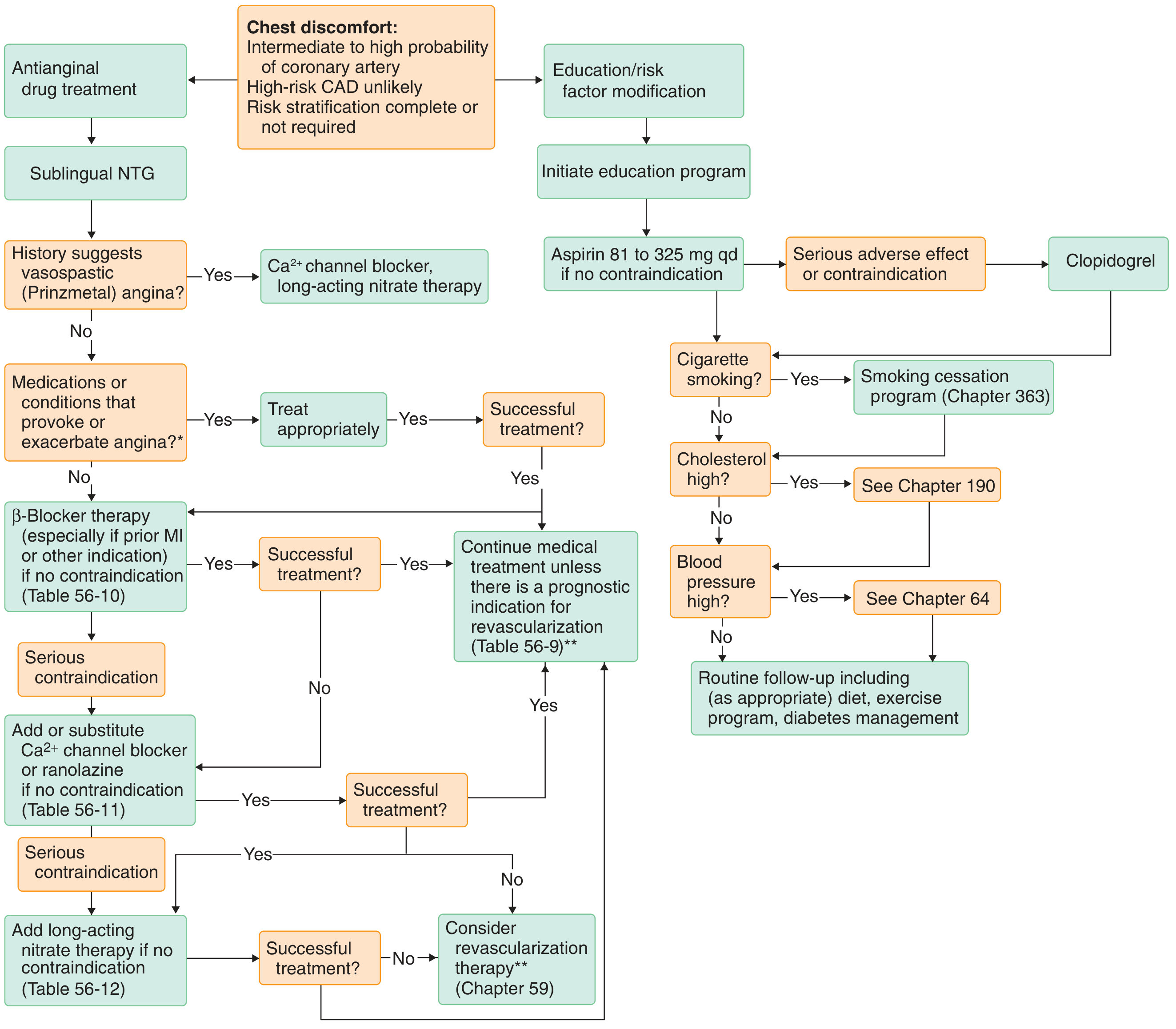
Goldman-Cecil Medicine - Algorithm for stable angina management
5. Revascularization: PCI vs. CABG
When to Revascularize
According to ACC/AHA guidelines (Table 56-8, Goldman-Cecil):
CABG is indicated for:
- Medically refractory angina - for symptom relief
- Left main CAD or three-vessel disease (regardless of LV function) - to prolong life
- Proximal LAD involvement (any number of vessels) - may prolong life
- Diabetic patients with 2-3 vessel disease - reduces composite death/MI/stroke vs. medical therapy; reduces CV events and death
PCI is indicated for:
- Symptomatic angina - for symptom relief
- Does not reduce death, MI, or major cardiovascular events when added to optimal medical therapy as initial management in stable ischemic heart disease
- Not indicated for purely anatomical stenosis in the absence of ischemia symptoms
PCI vs. CABG Comparison
| Feature | PCI | CABG |
|---|---|---|
| Single-vessel disease | Excellent symptom relief; repeat revascularization more common | Excellent symptom relief |
| Multivessel disease (non-diabetic) | Acceptable alternative | Acceptable alternative; preferred in complex/high-risk |
| Multivessel disease + diabetes | Inferior to CABG | Treatment of choice |
| Left main disease | Comparable for low-to-intermediate complexity (SYNTAX score); more repeat revascularization | Preferred especially for complex anatomy |
| LV dysfunction (EF ≤35%) | Similar mortality; higher MI and repeat revascularization risk; lower stroke risk | Favored for reducing MI and repeat revascularization |
| Older/frail patients | Lower procedural risk; preferred if surgical risk is prohibitive | Higher peri-operative risk; benefit must outweigh risk |
Key data on LV dysfunction: In 4616 patients with multivessel disease and severe LV dysfunction (EF ≤35%), PCI (EES) vs. CABG showed similar mortality (HR 1.01) but higher MI risk (HR 2.16) and higher repeat revascularization (HR 2.54) with PCI.
- Fuster and Hurst's The Heart, 15th ed.
6. Refractory Angina
Defined as persistent angina despite maximal medical therapy AND revascularization (or when revascularization is no longer feasible). This represents end-stage ischemic heart disease.
Options for Refractory Angina
| Therapy | Mechanism / Evidence |
|---|---|
| Spinal Cord Stimulation (SCS) | Electrode at C7-T1 dorsal epidural space; modulates sympathetic/parasympathetic tone, may improve coronary blood flow; ESBY trial: lower 6-month mortality vs. CABG in high-surgical-risk patients; subsequent trials underpowered |
| Enhanced External Counterpulsation (EECP) | Pneumatic cuffs on lower extremities synchronized to cardiac cycle; increases diastolic coronary perfusion pressure; ~35 hours of treatment; reduces angina frequency, improves exercise tolerance and QoL; best in non-smokers with severely limiting angina; contraindicated in aortic regurgitation, recent revascularization, severe hypertension |
| Coronary Sinus Reducing Device (Reducer) | Implanted hourglass-shaped stent in coronary sinus; redistributes blood from epicardium to ischemic subendocardium; COSIRA trial: significant improvement in symptoms and QoL |
| Transmyocardial Laser Revascularization (TMLR) | Surgical laser channels from LV epicardium; may promote angiogenesis; used in patients not amenable to standard revascularization |
| Chelation therapy | Limited evidence; not routinely recommended |
- Fuster and Hurst's The Heart, 15th ed.
- Goldman-Cecil Medicine
7. Special Populations
Elderly (>65-80 years)
- Atypical presentations (dyspnea, fatigue) are common; silent ischemia more prevalent
- Standard risk scores (Framingham, Pooled Cohort Equations) don't apply above age 80
- ISCHEMIA and PROMISE trials support conservative management with OMT as a reasonable first approach
- Revascularization decisions must weigh frailty, comorbidities, and patient preference
Diabetics
- CABG is preferred over PCI for multivessel disease
- SGLT2 inhibitors and GLP-1 agonists provide additional CV risk reduction
- Higher risk for silent ischemia, larger infarcts, and worse post-PCI outcomes
Advanced CHD with Heart Failure (Ischemic Cardiomyopathy)
- Revascularization (particularly CABG) should be considered in patients with HF and viable myocardium (hibernating myocardium)
- STICH trial extended follow-up (10 years) showed CABG + OMT reduced all-cause mortality vs. OMT alone in patients with EF ≤35%
- Cardiac MRI and PET viability imaging guide revascularization decisions
HIV and Advanced CHD
-
HIV patients have significantly higher MI rates even after controlling for traditional risk factors; inflammation and immune activation drive accelerated atherosclerosis
-
Dyslipidemia management requires awareness of statin-antiretroviral drug interactions: simvastatin is contraindicated with protease inhibitors; fluvastatin is safer but needs lower starting dose
-
HIV is now counted as a major cardiovascular risk factor for primary prevention decisions
-
Goldman-Cecil Medicine, p. 3729
8. Secondary Prevention - Summary Targets
| Risk Factor | Target / Intervention |
|---|---|
| LDL cholesterol | <70 mg/dL (US); <55 mg/dL (European guidelines) |
| Blood pressure | <130/80 mmHg |
| HbA1c (diabetes) | Individualized; SGLT2i/GLP-1 for CV risk reduction |
| Smoking | Complete cessation; formal cessation program |
| Weight/BMI | Target normal BMI; Mediterranean-style or DASH diet |
| Physical activity | Regular aerobic exercise; cardiac rehabilitation |
| Antiplatelet | Aspirin 81-100 mg/day (lifelong) |
| Statin | High-intensity; add ezetimibe or PCSK9i if target not reached |
| ACE-I/ARB | All patients with CAD + reduced EF, hypertension, or diabetes |
| Beta-blocker | Post-MI, reduced EF |
Recent Evidence (2024-2026)
- A 2025 meta-analysis on CT angiography (PMID: 40758074) confirmed that advanced CCTA analyses (CT-FFR, pericoronary fat attenuation, plaque characteristics) significantly predict future cardiac events beyond conventional angiographic stenosis severity.
- A 2025 systematic review and meta-analysis (PMID: 40472168) on antithrombotic therapy in patients with oral anticoagulation + stabilized CAD found that single antithrombotic therapy (OAC alone) was associated with lower bleeding risk without significantly increasing ischemic events compared to dual therapy.
- A 2026 network meta-analysis (PMID: 41145110) comparing drug-coated balloons (DCB) vs. drug-eluting stents (DES) for coronary lesions supports second-generation or newer DES as the preferred option for most lesions.
Key Takeaways:
- Advanced CHD is best managed with intensive secondary prevention as the foundation - statins, antiplatelet therapy, ACE-I/ARB, and lifestyle modification.
- CABG is life-prolonging in left main, three-vessel, and proximal LAD disease, and is the preferred revascularization strategy in diabetics with multivessel disease.
- PCI improves symptoms but does not reduce hard endpoints in stable CHD when added to optimal medical therapy.
- Refractory angina (despite maximal therapy) can be palliated with EECP, spinal cord stimulation, or the coronary sinus reducer device.
- Ischemic cardiomyopathy with viable myocardium benefits from revascularization (particularly CABG) for mortality reduction.
This is a shared conversation. Sign in to Orris to start your own chat.