
Screenshot_20260620-122126.png
Explain
Reading File
Finding Sources
Searching PubMed
gynecomastia etiology pathogenesis hormonal
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I have everything I need for a thorough answer. Here is the complete explanation:
Gynecomastia - Etiology, Hormonal Dependency, and Pathogenesis
Definition
Gynecomastia is enlargement of the male breast gland. True gynecomastia involves glandular breast tissue >4 cm in diameter (often tender, firmer than fat, with fibrous-like cords) and must be distinguished from pseudogynecomastia (simple excess adipose tissue without glandular proliferation).
- Harrison's Principles of Internal Medicine 22E, p. 3159
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 965
Core Hormonal Mechanism (Pathogenesis)
The fundamental defect is a relative or absolute increase in the estrogen-to-androgen ratio at the level of breast tissue.
- Estrogens stimulate ductal epithelial proliferation and connective tissue growth in the breast
- Androgens counteract this effect
- When this balance is disrupted - either by too much estrogen, too little androgen, or impaired androgen action - breast glandular tissue proliferates
Histologically, there is:
- Increase in dense collagenous connective tissue
- Epithelial hyperplasia of the duct lining
- Lobule formation is almost never seen (important distinction from female breast)
Etiology - Classification of Causes
1. Physiologic Gynecomastia (Normal at 3 Life Stages)
| Stage | Mechanism |
|---|---|
| Neonatal | Transplacental transfer of maternal and placental estrogens |
| Pubertal | High estrogen-to-androgen ratio in early puberty (transient) |
| Aging/Senescent | Increased aromatase activity in fat + age-related decline in testosterone |
2. Pathologic Causes
A. Androgen Deficiency (Hypogonadism)
Any cause of testosterone deficiency leads to gynecomastia because estrogen synthesis continues via aromatization of residual adrenal and gonadal androgens:
- Klinefelter syndrome (47,XXY) - a characteristic feature
- Androgen insensitivity disorders
- Bilateral orchiectomy, mumps orchitis, testicular torsion
- Androgen deprivation therapy (GnRH analogues +/- AR blockers) in prostate cancer - causes painful breast enlargement
B. Excess Estrogen Production
- Leydig cell tumors and Sertoli cell tumors (the latter alone or in Peutz-Jeghers syndrome or Carney complex)
- Granulosa cell tumors and adrenal tumors producing estrogen precursors
- hCG-secreting tumors (testicular germ cell tumors) - hCG stimulates Leydig cells to produce excess estrogen
C. Increased Peripheral Aromatization (Androgen → Estrogen Conversion)
- Obesity - adipose tissue is rich in aromatase; increased conversion of androstenedione to estrone
- Liver disease (cirrhosis) - diminished catabolism of androstenedione shunts precursors toward peripheral aromatase; the liver normally metabolizes estrogens
- Hyperthyroidism - elevates SHBG, which increases the free estradiol-to-free testosterone ratio
- Congenital adrenal hyperplasia (CAH) - increased substrate availability (androstenedione)
- Familial aromatase excess syndrome - autosomal dominant or X-linked disorder; chimeric CYP19 gene activated by regulatory elements of neighboring genes (TRPM7, TMOD3), causing excessive estrogen production in fat and extragonadal tissues; presents with peripubertal gynecomastia, advanced bone age, short stature, premature epiphyseal closure, and hypogonadotropic hypogonadism
D. Drug-Induced Gynecomastia
Drugs act through multiple mechanisms:
| Mechanism | Examples |
|---|---|
| Direct estrogen-like action | Oral contraceptives, phytoestrogens, digitalis |
| Inhibit androgen synthesis | GnRH agonists, ketoconazole |
| Block androgen receptor | Spironolactone, enzalutamide, flutamide |
| Mechanism unclear | Cimetidine, imatinib, antiretrovirals (ART for HIV), alcohol, marijuana, heroin, anabolic steroids |
Note: Spironolactone binds androgen receptors as an antagonist and is a classic cause of drug-induced gynecomastia.
Summary Diagram - Diagnostic Evaluation
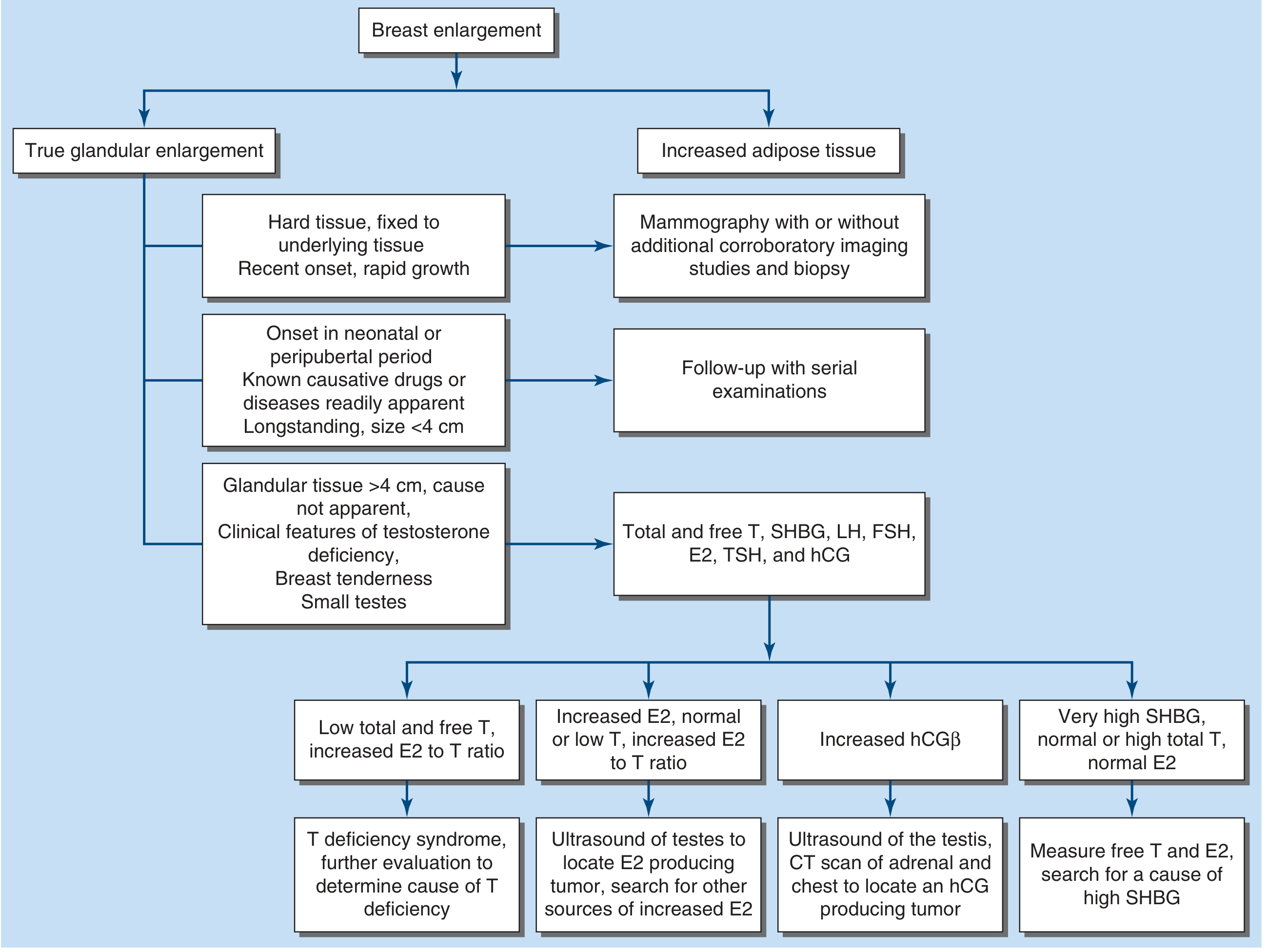
The flowchart guides workup based on tissue type and hormonal findings:
- Low T + high E2/T ratio → testosterone deficiency workup
- High E2 + normal/low T → search for estrogen-secreting tumor (testicular/adrenal ultrasound)
- Elevated hCGβ → search for hCG-producing tumor
- Very high SHBG → measure free T and E2, find cause of elevated SHBG
Quick Memory Aid
GYNECOMASTIA = Estrogen UP or Androgen DOWN
| Category | Key Examples |
|---|---|
| Physiologic | Neonatal, Pubertal, Aging |
| Hypogonadism | Klinefelter, orchiectomy, GnRH therapy |
| Tumor-related | Leydig cell tumor, Sertoli cell tumor, hCG-secreting GCT |
| Liver disease | Cirrhosis (key cause) |
| Obesity | Increased aromatase in fat |
| Hyperthyroidism | Elevated SHBG |
| Drugs | Spironolactone, cimetidine, ketoconazole, antiretrovirals, anabolic steroids |
| Familial | CYP19/aromatase excess syndrome |
Sources: Harrison's Principles of Internal Medicine 22E (p. 3159-3160) | Robbins & Cotran Pathologic Basis of Disease | Henry's Clinical Diagnosis (Laboratory Methods)
This is a shared conversation. Sign in to Orris to start your own chat.