Septoplasty incisions according to scott brown
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Excellent - I have the diagram and full text. Here is the complete answer based directly from Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1.
Septoplasty Incisions - Scott-Brown's Otorhinolaryngology
According to Scott-Brown's, the incision for septoplasty is the hemitransfixion incision, placed at the caudal edge of the septum to provide access to the whole septum including the caudal L-strut (unlike SMR, which cannot address the caudal and dorsal struts).
The diagram below illustrates the placement of all incisions:
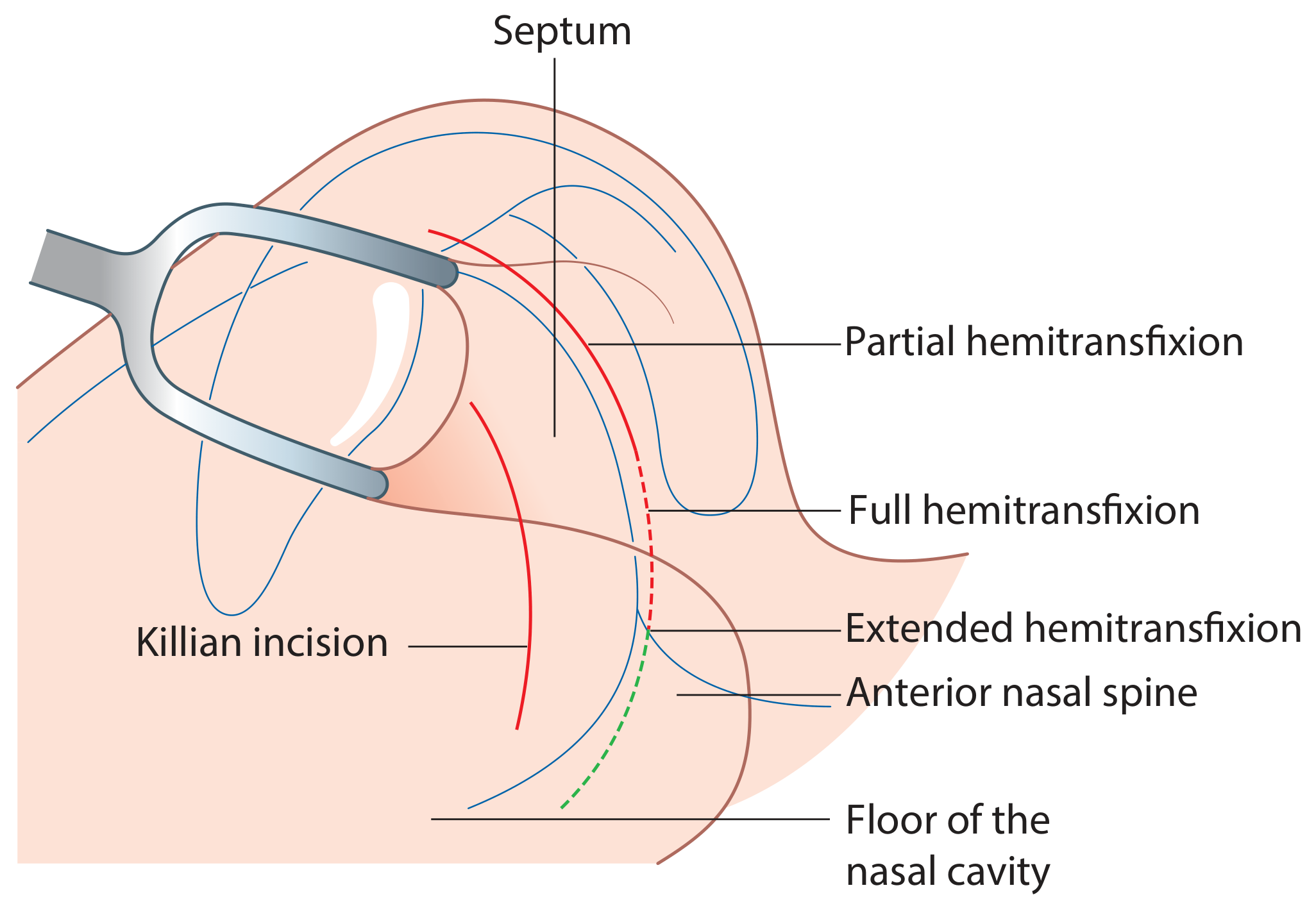
Figure 103.4 - Placement of different incisions for approach to the septum (Scott-Brown's Vol. 1, p. 1186)
Types of Hemitransfixion Incision
The length of the incision is chosen based on the access required:
| Incision | Indication |
|---|---|
| Partial hemitransfixion | When access to the most posterior parts of the septum is NOT required |
| Full hemitransfixion | When access to the whole of the caudal arm of the L-strut is needed |
| Extended hemitransfixion | When access to the floor of the nasal cavity is also required (extends down past the anterior nasal spine to the floor) |
Killian Incision (also shown in the diagram)
The Killian incision is placed more posteriorly on the septum (a few millimetres behind the caudal edge). It is a separate vertical incision used mainly in SMR (submucous resection) but is shown alongside the hemitransfixion variants for comparison. Because it is placed away from the caudal edge, it does NOT provide full access to the L-strut.
Mucosal Flap Principles After Incision
After the chosen incision is made:
-
Unilateral (concave side) flap elevation is sufficient in most cases - it allows excision of cartilage/bone, detachment of the osseocartilaginous junction, and scoring of the concave side, while keeping the opposite mucosa intact to reduce the risk of septal perforation.
-
Bilateral flap elevation is needed when:
- Sutures are to be placed within the mucosal envelope
- S-shaped deformities require scoring on both sides
- Access to both sides is otherwise required
-
Caudally, the perichondrium is tightly adherent to the cartilage, so the correct subperichondrial plane must be carefully identified, often by scoring the area first.
Two Techniques for Raising the Flap
1. Back-to-Front (Cephalad-to-Caudal) Technique:
- Flap is initially raised anteriorly and pushed cephalically
- Direction is then reversed - raised from cephalic position downward (posteriorly and caudally)
- The subperiosteal plane is established first (correct level), then transitions to subperichondrial, reducing the chance of mucosal tear
2. Front-to-Back Technique:
- An anterior tunnel is raised over the quadrilateral cartilage and bony septum
- A separate posterior tunnel is raised subperiosteally behind the septal spur
- The mucosa remains attached at the spur itself, which is then addressed by sharp dissection without tension from either side - reducing the risk of tearing over the most prominent part of the spur
Source: Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Vol. 1, Chapter 103, pp. 1185-1187
This is a shared conversation. Sign in to Orris to start your own chat.