Canal stenosis lumbar cervical recent advances
Reading File
Finding Sources
Finding Sources
Searching PubMed
lumbar spinal stenosis treatment
Searching PubMed
cervical spinal stenosis myelopathy surgery
Searching the Web
lumbar cervical canal stenosis recent advances 2025 2026 treatment guidelines
Reading File
Reading File
Reading Article
PMID: 39379938
Reading Article
PMID: 39938000
Reading Article
PMID: 41802210
Reading File
Finding Sources
Searching PubMed
lumbar stenosis minimally invasive endoscopic decompression
Reading Article
PMID: 38764362
Reading File
Reading Article
PMID: 38190892
Reading Article
PMID: 39501233
Searching Images
lumbar spinal stenosis MRI canal narrowing
I now have comprehensive material. Let me compose the full answer.
Spinal Canal Stenosis: Lumbar & Cervical — A Comprehensive Review with Recent Advances
PART 1 — LUMBAR SPINAL STENOSIS (LSS)
Definition & Anatomy
Lumbar spinal stenosis is narrowing of the lumbar spinal canal, lateral recesses, or neural foramina causing symptomatic or asymptomatic compression of lumbosacral nerve roots. Three distinct anatomical subtypes exist:
| Subtype | Boundaries | Key Compressors |
|---|---|---|
| Central | Bordered laterally by medial border of superior articular process | Ligamentum flavum buckling, disc bulge, osteophytes |
| Lateral recess | From dural sac nerve root takeoff to medial pedicle border | Hypertrophied facet, LF |
| Foraminal | Disc (anterior), pars (posterior), pedicles (superior/inferior) | Disc height loss, osteophytes |
L4–5 is the most common level, followed by L3–4, L2–3, L5–S1, and L1–2; most patients have multilevel disease.
Epidemiology
- Congenital stenosis: ~7% of the general population
- Degenerative midsagittal stenosis: ~30%
- ~10% of patients have both cervical and lumbar stenosis simultaneously (tandem stenosis)
- More severe stenosis correlates with older age and more low back pain
- Diffuse idiopathic skeletal hyperostosis (DISH) strongly predisposes to stenosis
— Goldman-Cecil Medicine, p. 2315–2320
Pathophysiology
Static narrowing from degenerative spondylotic changes (disc bulging, osteophytic spurring, facet joint hypertrophy, ligamentum flavum thickening, posterior longitudinal ligament thickening, spondylolisthesis) superimposed on any congenital narrowing.
Dynamic narrowing is critical: lumbar extension causes the inferior articular processes to slide posteroinferiorly, narrowing the canal and foramina further; the ligamentum flavum buckles anteriorly; discs and PLL bulge posteriorly. This explains the postural provocation of symptoms.
Clinical Presentation — Neurogenic Claudication (Pseudoclaudication)
- Lower limb numbness, weakness, or pain on standing or walking, typically bilateral posterior leg symptoms
- Relieved by sitting or leaning forward (flexion widens the canal)
- Mimics vascular claudication but: improves with posture change (not just rest), absent peripheral arterial disease, pain may radiate to entire limb
- Fixed neurologic deficits (L5/S1 distribution) if concomitant peripheral neuropathy
- Bowel/bladder typically spared (unlike cauda equina syndrome)
Bicycling test: patients can often ride a bicycle (flexed posture) but cannot walk the same distance.
Diagnosis
| Test | Role |
|---|---|
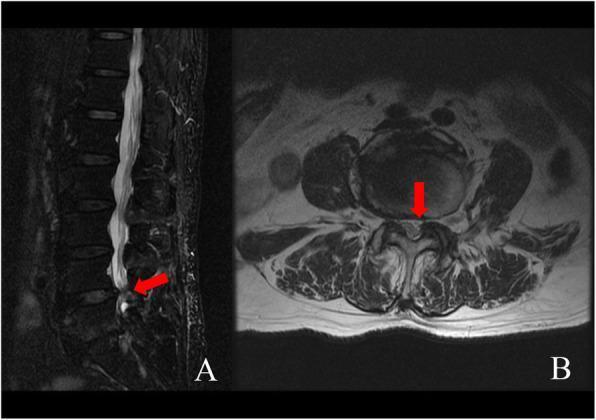
| MRI | Gold standard; shows canal, soft tissue, cord/nerve roots |
| CT plain | Screening; bony detail |
| CT myelography | Upright dynamic imaging; better for post-surgical cases |
| Flexion/extension X-rays | Detect spondylolisthesis or dynamic instability |
| EMG/NCS | Differentiates radiculopathy from peripheral neuropathy |
| Vascular studies | Exclude peripheral arterial disease |
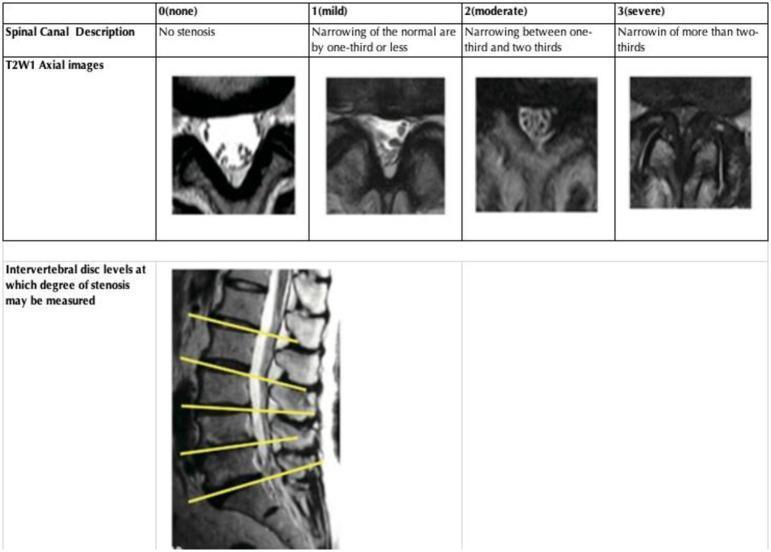
MRI grading of central canal stenosis:
- Grade 0: patent canal, CSF visible around nerve roots
- Grade 1 (mild): up to one-third narrowing
- Grade 2 (moderate): one-third to two-thirds narrowing
- Grade 3 (severe): >two-thirds narrowing, CSF effaced, nerve roots bundled
Treatment
Conservative (First-Line)
- Exercise: core/abdominal strengthening, reducing lumbar lordosis
- Assistive devices: cane or walker enables longer ambulation in flexed posture
- Lumbar corsets/braces: reduce lordosis when standing
- Weight loss in obese patients reduces lordosis and axial load
- Epidural corticosteroid injections (ESIs): controversial — the 2025 AAN systematic review (90 RCTs, PMID 39938000) found ESIs possibly reduce short-term disability in lumbar stenosis (SRD −26.2%, NNT 4) but evidence for pain reduction is insufficient. Long-term benefit uncertain.
Surgical Indications
- Symptoms >3 months interfering with work/leisure
- Progressive neurologic deficits
- Failure of conservative management
Standard Surgical Options
| Procedure | Indication | Notes |
|---|---|---|
| Laminectomy + partial medial facetectomy | Central stenosis | Standard; "open decompression" |
| Decompression of LF/lamina + partial facetectomy | Lateral recess stenosis | |
| Fusion added | Spondylolisthesis, scoliosis, facet removal causing instability, pars defect, radiographic instability | SPORT trial (4-yr) showed surgical > nonoperative for pain and function |
| Interspinous distraction device (e.g., X-Stop) | Unable to tolerate open surgery; short life expectancy | Placed outpatient under local anesthesia; prevents extension |
Key point (SPORT trial): operative treatment demonstrated significant improvement in pain and function vs. nonoperative at 4-year follow-up for both central stenosis and degenerative spondylolisthesis.
Fusion debate: Goldman-Cecil states lumbar fusion adds no incremental benefit even with spondylolisthesis ≥3 mm — however, recent network meta-analysis data (see below) suggests individual patient factors matter.
RECENT ADVANCES — LUMBAR STENOSIS
1. Endoscopic Decompression (Major Shift 2023–2025)
A systematic review & meta-analysis (Spine J, 2024) (n=1,997 patients, PMID 38190892) comparing full-endoscopic vs. microscopic decompression found:
- Significantly less intraoperative blood loss (WMD −33 mL)
- Shorter hospital stay (WMD −1.79 days)
- Fewer durotomies (RR 0.63) and wound infections (RR 0.23)
- Non-significant trend to better pain and function at 2 years
Biportal endoscopic (UBE) vs. uniportal endoscopic: a 2025 systematic review (Front Surg, PMID 40589530) confirms both are effective with comparable outcomes, with UBE offering better visualization for bilateral decompression via unilateral approach.
2. Surgical NMA — Which Operation is Best? (2024)
A landmark network meta-analysis in BMC Medicine (Chen et al., 2024, PMID 39379938) of 43 RCTs (5,017 patients, 14 surgical techniques) vs. laminectomy reference:
| Surgical Option | Short-term Function | Adverse Events |
|---|---|---|
| Endoscopic-assisted laminotomy | −8.61 (best, moderate evidence) | Fewer AEs (OR 0.27) |
| Laminectomy + Coflex interspinous | −8.41 (moderate evidence) | — |
| X-Stop | −6.65 (low evidence) | — |
Conclusion: Endoscopic-assisted laminotomy is likely the safest and most effective surgical intervention, though durability beyond 6 months needs larger studies.
3. Decompression vs. Fusion for Spondylolisthesis (Ongoing Debate)
Two systematic reviews/meta-analyses (2024–2025):
- Cheng et al., BMC Musculoskeletal Disorders, 2024 (PMID 39256670)
- Guo et al., World Neurosurgery, 2025 (PMID 39603451)
Both found no consistent superiority of fusion over decompression alone for single-level degenerative spondylolisthesis, challenging prior assumptions — though fusion remains indicated for dynamic instability and severe listhesis.
PART 2 — CERVICAL SPINAL STENOSIS & SPONDYLOTIC MYELOPATHY (CSM)
Definition
Cervical spinal stenosis is narrowing of the cervical spinal canal from congenital factors, acquired spondylosis, or both. Cervical spondylotic myelopathy (CSM) occurs when this stenosis causes spinal cord injury.
Epidemiology
- Cervical spondylosis prevalence: 95% in men and 89% in women over age 60
- 7.5% of asymptomatic patients at autopsy have spondylotic cord compression
- Risk factors: repeated trauma, male sex, older age, stenosis at another level, family history
Pathophysiology
Structures causing canal narrowing:
- Bulging discs → osteophytic spurring (spondylotic bars)
- Posterior longitudinal ligament (PLL) thickening
- Ligamentum flavum hypertrophy (posteriorly)
- Uncovertebral process enlargement
- Facet joint hypertrophy
Most commonly affected: C5–6 > C6–7 > C4–5 (usually multilevel)
Dual mechanism of injury: mechanical compression + impaired microcirculation
Dynamic component: flexion pulls cord over osteophytes; extension pinches cord between posteroinferior disc–osteophyte complex and posteriorly encroaching LF.
Clinical Features
| Syndrome | Features |
|---|---|
| Myelopathy | Spastic gait, Lhermitte's sign (neck flexion → electric shock sensation), hand dexterity loss, upper motor neuron signs (hyperreflexia, Babinski, Hoffmann) |
| Radiculopathy | Dermatomal pain/numbness/weakness depending on level |
| Mixed | Most common presentation |
Nurick / mJOA (modified Japanese Orthopaedic Association) scales are standard for grading severity.
Diagnosis
MRI is the gold standard:
- T2 hyperintensity in the cord = myelomalacia (indicates chronic injury, worse prognosis)
- Sagittal images show multilevel cord compression
- Axial images show cord deformity and loss of CSF around cord
(Goldman-Cecil describes Fig 369-7: multilevel cervical stenosis C3–4 > C4–5 > C5–6 with myelomalacia arrow at C3–4 level)
Treatment
Conservative
- Cervical collar (daytime), cervical pillow
- Physical therapy targeting imbalance and weakness — avoid vigorous neck range of motion
- NSAIDs for pain (naproxen 400 mg BID)
- Cervical ESIs for radicular pain (evidence weak — the 2025 AAN review found insufficient evidence for cervical stenosis specifically)
Surgical — Indications & Approaches
Indications: moderate–severe neurologic deficits OR progressively worsening myelopathy
| Approach | Procedures | Best For |
|---|---|---|
| Anterior | ACDF (anterior cervical discectomy & fusion), artificial disc replacement (1–2 levels) | 1–3 level disease, kyphosis, anterior pathology |
| Posterior | Laminectomy, laminoplasty (cervical) | >3 levels, preserved lordosis, ossification PLL |
- Surgical outcomes: 50–70% neurologic improvement; recovery plateaus ~6 months; some late deterioration
- Adjacent segment degeneration after fusion: ~3%/year (may need reoperation)
RECENT ADVANCES — CERVICAL STENOSIS
1. Laminoplasty vs. Laminectomy + Fusion (2024 Meta-Analysis)
Daher et al., Spine, 2024 (PMID 38764362) — 22 studies, 2,128 patients:
| Outcome | Laminoplasty (LP) | Laminectomy + Fusion (LF) |
|---|---|---|
| Operative time | ✅ Shorter (p=0.009) | Longer |
| Blood loss | ✅ Less (p=0.02) | More |
| Overall complications | ✅ Lower (p<0.00001) | Higher |
| C5 palsy rate | ✅ Lower (p=0.003) | Higher |
| Neck Disability Index | ✅ Lower (better, p=0.0004) | Higher |
| JOA, VAS, lordosis | No significant difference |
Conclusion: Laminoplasty has a more favorable complication profile; LF remains appropriate for patients with instability or kyphosis.
2. White Cord Syndrome After Cervical Surgery
A 2025 systematic review (Eur Spine J, PMID 39266775) characterized this rare but devastating reperfusion injury (sudden neurologic deterioration after decompression). Risk factors include severe preoperative stenosis and prolonged cord compression. High-dose steroids remain the primary treatment; no proven preventive strategy.
PART 3 — TANDEM SPINAL STENOSIS (TSS)
Stenosis at both cervical and lumbar levels simultaneously (~10% of stenosis patients).
New Treatment Algorithm (2026)
The most recent systematic review and meta-analysis — Kotheeranurak et al., JAAOS, May 2026 (PMID 41802210) — analyzed 1,006 surgical interventions and proposed a decision algorithm:
| Scenario | Recommended Strategy | JOA SMD |
|---|---|---|
| Myelopathy present | Staged: cervical-first decompression | 4.31 (highest improvement) |
| No myelopathy, fit patient | Simultaneous decompression (single anesthesia) | 2.65 |
| Lumbar-first staged | Not recommended | 1.94 (non-significant) |
Key takeaway: cervical decompression should be prioritized when myelopathy is present; simultaneous surgery is feasible in fit patients without myelopathy.
PART 4 — ARTIFICIAL INTELLIGENCE IN SPINAL STENOSIS (Emerging)
A 2024 systematic review (BMC Surgery, PMID 39501233) of 90 AI applications in spinal surgery found AI is increasingly being used for:
- Automated stenosis grading on MRI (deep learning, reducing interobserver variability)
- Surgical indication assessment (predicting who benefits from surgery)
- Intraoperative assistance (navigation, pedicle screw placement)
- Outcome prediction (identifying high-risk patients for complications preoperatively)
Summary Table — Therapeutic Hierarchy
| Condition | First-Line | Second-Line | Surgery (Gold Standard) |
|---|---|---|---|
| LSS (no instability) | Exercise, weight loss, gait aids | ESIs (short-term) | Endoscopic laminotomy or laminectomy |
| LSS + spondylolisthesis | Conservative 3 months | ESIs | Decompression ± fusion |
| CSM (mild, stable) | Conservative | Epidural injections (radiculopathy) | Monitor |
| CSM (moderate–severe, progressive) | Surgery | — | ACDF or laminoplasty/laminectomy |
| Tandem (with myelopathy) | Surgery | — | Staged: cervical first |
Key References
- Goldman-Cecil Medicine International Edition, pp. 2315–2414 — Lumbar & Cervical Stenosis
- Miller's Review of Orthopaedics 9th ed., pp. 9057–9070 — Lumbar Stenosis Classification & SPORT trial
- Chen L et al. BMC Med 2024 — Surgical NMA for LSS [PMID 39379938]
- Armon C et al. Neurology 2025 — AAN ESI Guideline [PMID 39938000]
- Daher M et al. Spine 2024 — Laminoplasty vs LF meta-analysis [PMID 38764362]
- Chin BZ et al. Spine J 2024 — Endoscopic vs. microscopic LSS [PMID 38190892]
- Kotheeranurak V et al. JAAOS 2026 — Tandem stenosis algorithm [PMID 41802210]
- Han H et al. BMC Surg 2024 — AI in spinal surgery [PMID 39501233]
This is a shared conversation. Sign in to Orris to start your own chat.