Toxaemia of pregnancy
Reading File
Finding Sources
Searching PubMed
"preeclampsia"[MeSH Terms] AND "pathophysiology"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Toxaemia of Pregnancy (Preeclampsia/Eclampsia)
"Toxaemia of pregnancy" is an older umbrella term that encompasses the spectrum of gestational hypertension, preeclampsia, eclampsia, and HELLP syndrome - conditions that arise after 20 weeks of gestation and reflect widespread maternal endothelial injury, originating in placental dysfunction.
Definition and Diagnostic Criteria
Preeclampsia is defined as new-onset hypertension (≥140 mmHg systolic or ≥90 mmHg diastolic) after 20 weeks of gestation in a previously normotensive woman, combined with proteinuria or evidence of other end-organ involvement. Proteinuria (≥300 mg/24h, protein:creatinine ratio ≥0.3, or dipstick ≥1+) is present in approximately 75% of cases but is no longer an absolute requirement for the diagnosis if other features are present.
| Criterion | Threshold |
|---|---|
| Systolic BP | ≥140 mmHg (×2, ≥4 hours apart) |
| Diastolic BP | ≥90 mmHg (×2, ≥4 hours apart) |
| Proteinuria | ≥300 mg/24h or P:Cr ratio ≥0.3 |
| Thrombocytopenia | Platelets <100,000/μL |
| Renal insufficiency | Creatinine >1.1 mg/dL or doubling of baseline |
| Liver dysfunction | Transaminases ×2 normal, or RUQ/epigastric pain |
| Pulmonary edema | - |
| Cerebral/visual disturbances | - |
- Tintinalli's Emergency Medicine, p.1632-1635
Severe Features
Severe preeclampsia is defined by any of the following:
- Systolic BP ≥160 mmHg or diastolic ≥110 mmHg (×2, at least 4 hours apart while at rest)
- Thrombocytopenia (platelets <100,000/μL)
- Transaminases ≥2× normal, or severe RUQ/epigastric pain
- Serum creatinine >1.1 mg/dL or doubling of creatinine
- Pulmonary edema
- New-onset headache unresponsive to medication, or visual disturbances
Epidemiology and Risk Factors
Preeclampsia complicates 7-10% of pregnancies in the United States. Eclampsia is far less common (1 in 10,000-15,000 pregnancies). Severe preeclampsia contributes to ~7% of maternal deaths and ~20% of perinatal deaths, with maternal deaths most often due to stroke, pulmonary edema, or hepatic necrosis/rupture.
Risk factors include:
-
Nulliparity (highest risk - primigravid state)
-
Multiple gestation (10-20% for twins, 25-60% for triplets, up to 90% for quadruplets)
-
Prior history of preeclampsia
-
Pregestational diabetes (2-4× increased risk)
-
Maternal age >40 years
-
Chronic hypertension, renal disease, collagen-vascular disease
-
High altitude (2-4× increased incidence due to hypoxia)
-
Assisted reproductive technologies
-
Creasy & Resnik's Maternal-Fetal Medicine, p.3001-3003
-
Morgan & Mikhail's Clinical Anesthesiology, p.1644
Pathophysiology
The pathophysiology operates in two stages, both rooted in the placenta.
Stage 1 - Defective Placentation
In normal pregnancy, extravillous cytotrophoblasts invade the uterine spiral arteries of the decidua and myometrium, converting them from narrow resistance vessels into wide-caliber, low-resistance capacitance vessels. In preeclampsia, this invasion is incomplete - cytotrophoblast invasion is limited to the superficial decidua, and the myometrial segments remain narrow and undilated. Cytotrophoblasts fail to undergo the normal adhesion-molecule switching ("pseudovasculogenesis"), driven in part by excess HIF-1 activity and altered TGF-β3 signaling.
This results in placental ischemia - supported by abnormal uterine artery Doppler (decreased uteroplacental perfusion) seen weeks before clinical onset, and by the histological finding of acute atherosis (fibrin deposition, intimal thickening, endothelial damage, and infarcts) in decidual arteries.
Stage 2 - Maternal Endothelial Dysfunction
The ischemic placenta releases factors into the maternal circulation, producing widespread endothelial injury. The key mediators include:
- sFlt-1 (soluble fms-like tyrosine kinase-1): A soluble decoy receptor that binds and neutralises free VEGF and PlGF (placental growth factor), dramatically reducing circulating levels of these pro-angiogenic factors. VEGF is critical for maintaining fenestrated endothelium in the kidney, brain, and liver - the exact organs most affected in preeclampsia. sFlt-1 levels rise weeks before clinical disease, while PlGF levels fall (as shown in the figure below).
- sEng (soluble endoglin): A co-receptor for TGF-β that impairs NO-dependent vasodilation.
- TXA2/PGI2 imbalance: Elevated thromboxane A2 (vasoconstrictor, pro-platelet aggregation) and reduced prostacyclin (vasodilator, anti-platelet aggregation).
- Endothelin-1: Potent vasoconstrictor, further activates platelets.
- Reduced nitric oxide production.
- Markers of endothelial activation: elevated von Willebrand antigen, cellular fibronectin, soluble E-selectin, IL-8, ICAM-1, CRP, leptin, and oxidative stress products.
The result is vasoconstriction, systemic hypertension, glomerular endotheliosis (causing proteinuria), and end-organ ischemia.
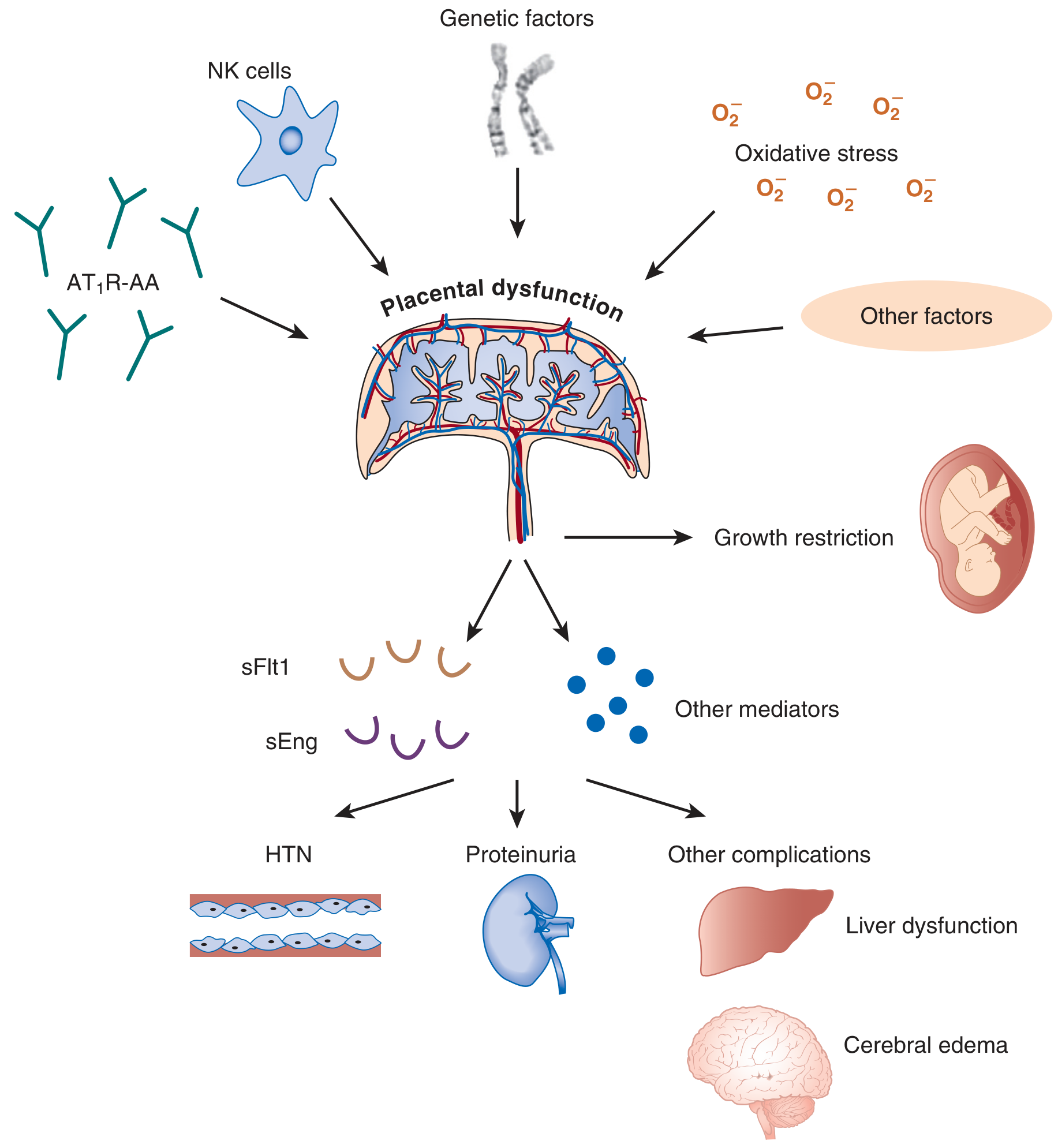
Pathogenesis of preeclampsia: placental dysfunction triggered by genetic, immunologic (NK cells, AT₁R autoantibodies), and oxidative-stress factors releases sFlt1 and sEng, causing hypertension, proteinuria, and end-organ damage. - Brenner & Rector's The Kidney
- Brenner & Rector's The Kidney, p.2148-2153
- Morgan & Mikhail's Clinical Anesthesiology, p.1644-1645
Renal Lesion
The histological hallmark of preeclampsia in the kidney is glomerular endotheliosis - swelling and vacuolization of glomerular endothelial cells with loss of fenestrations, reducing glomerular filtration. This is driven by VEGF deficiency (secondary to excess sFlt-1) and endothelin-1 excess, both reducing nephrin expression in podocytes. Clinically, this manifests as proteinuria, reduced GFR, sodium retention, and occasionally oliguria or acute kidney injury.
Organ System Complications
| System | Manifestation |
|---|---|
| Neurological | Headache, visual disturbances, hyperexcitability, seizures (eclampsia), cerebral edema, intracranial hemorrhage |
| Cardiovascular | Decreased intravascular volume, increased arteriolar resistance, hypertension, heart failure |
| Renal | Proteinuria, sodium retention, reduced GFR, acute kidney failure |
| Hepatic | Elevated transaminases, hepatic hematoma, hepatic rupture (in HELLP) |
| Haematological | Thrombocytopenia (~50% of cases), microangiopathic haemolytic anaemia |
| Pulmonary | Upper airway oedema, pulmonary oedema |
| Placental | Intrauterine growth restriction, placental abruption |
- Morgan & Mikhail's Clinical Anesthesiology, p.1645
HELLP Syndrome
HELLP = Hemolysis, Elevated Liver enzymes, Low Platelets - a severe variant of preeclampsia. It is more common in multigravid patients. Hypertension may be absent initially, and presenting symptoms (epigastric or RUQ pain, nausea, malaise) mimic gastroenteritis, cholecystitis, or hepatitis, making diagnosis easy to miss.
Diagnostic criteria:
- Peripheral smear: schistocytes (microangiopathic haemolysis)
- Platelet count <100,000/μL
- LDH elevated (haemolysis)
- Transaminases ≥2× normal
Complications include DIC, spontaneous hepatic rupture, splenic haemorrhage, abruptio placentae, and maternal/fetal death. Management mirrors severe preeclampsia - stabilise, control BP, IV magnesium, and deliver. The syndrome usually resolves within 3 days postpartum; persistence beyond 3 days should prompt consideration of TTP, HUS, or DIC.
- Tintinalli's Emergency Medicine, p.1673-1692
- Goldman-Cecil Medicine, p.1815
Eclampsia
Eclampsia is defined as new-onset seizures superimposed on preeclampsia, occurring from 20 weeks of gestation to 4 weeks postpartum. Seizures can occasionally occur in the absence of hypertension or proteinuria. It may present antepartum, intrapartum, or postpartum.
Management:
- Seizure control: Magnesium sulfate 4-6 g IV over 20-30 min, then 2 g/hr infusion for ≥24 hours
- Magnesium is renally excreted; reduce dose in renal insufficiency
- Toxicity signs: loss of patellar reflexes → respiratory depression → cardiac arrest
- Antidote: calcium gluconate 1 g IV
- Antihypertensive therapy (see below)
- Emergent obstetric consultation for delivery
Management
Definitive Treatment
Delivery is the only cure. Timing and mode depend on gestational age and severity.
Antihypertensive Therapy (Acute)
Target BP: 140-150/90-100 mmHg (do not normalise BP acutely - risks placental hypoperfusion)
| Agent | Dose | Route |
|---|---|---|
| Hydralazine | 5 mg | IV or IM |
| Labetalol | 20 mg | IV bolus |
| Nifedipine | 10-30 mg | PO |
Chronic management: Labetalol (first-line, 100-400 mg PO BD), methyldopa (250 mg 6-hourly PO), long-acting nifedipine (30-120 mg/day).
Contraindicated: ACE inhibitors and ARBs (teratogenic - damage fetal skull, lungs, kidneys).
Seizure Prophylaxis and Prevention
- IV magnesium sulfate for severe preeclampsia/eclampsia
- Low-dose aspirin (60-162 mg/day) from 12-16 weeks reduces preeclampsia incidence by ~50% in high-risk women (including diabetes, prior preeclampsia, multiple gestation)
HELLP
-
IV magnesium, BP control, hospital admission
-
Correct coagulopathy if indicated
-
Corticosteroids if <34 weeks (to delay delivery, improve fetal lung maturity)
-
Definitive treatment: delivery (especially if ≥34 weeks)
-
Tintinalli's Emergency Medicine, p.1695-1707
-
Creasy & Resnik's Maternal-Fetal Medicine, p.1802-1804
Laboratory Evaluation
| Test | Significance |
|---|---|
| CBC + peripheral smear | Thrombocytopenia, schistocytes (haemolysis) |
| Serum creatinine | Elevation = severe disease |
| ALT/AST | Elevation = severe disease / HELLP |
| LDH | Elevated in microangiopathic haemolysis |
| Uric acid | ≥5.5 mg/dL may indicate superimposed preeclampsia |
| 24-hr urine protein | >5 g = severe disease |
| Protein:creatinine ratio | ≥0.3 = significant proteinuria |
Prevention and Biomarkers
- sFlt-1/PlGF ratio is emerging as a predictive and diagnostic biomarker, rising weeks before clinical onset while PlGF levels fall
- Low-dose aspirin (initiated ideally before 16 weeks) is recommended by SMFM, ACOG, and ADA for all high-risk women
- Preeclampsia in a prior pregnancy significantly increases recurrence risk
Long-term Consequences
- Preeclampsia is associated with increased future risk of maternal cardiovascular disease, hypertension, and renal disease
- IUGR, prematurity, low birth weight, and abruption placentae in the index pregnancy
- Preeclampsia in a prior pregnancy increases risk in subsequent pregnancies
Key sources: Brenner & Rector's The Kidney | Creasy & Resnik's Maternal-Fetal Medicine | Morgan & Mikhail's Clinical Anesthesiology, 7e | Tintinalli's Emergency Medicine | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.