Lung tumors in detail with flow charts and diagrams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Lung Tumors - Comprehensive Reference
Sources: Harrison's Principles of Internal Medicine 22E (2025), Fishman's Pulmonary Diseases and Disorders, Grainger & Allison's Diagnostic Radiology, Mulholland & Greenfield's Surgery 7e, The Washington Manual of Medical Therapeutics
1. Overview & Classification
The WHO defines lung cancer as tumors arising from the respiratory epithelium (bronchi, bronchioles, alveoli). Lung cancer remains the leading cause of cancer death in both men and women worldwide.
WHO Classification - Major Cell Types
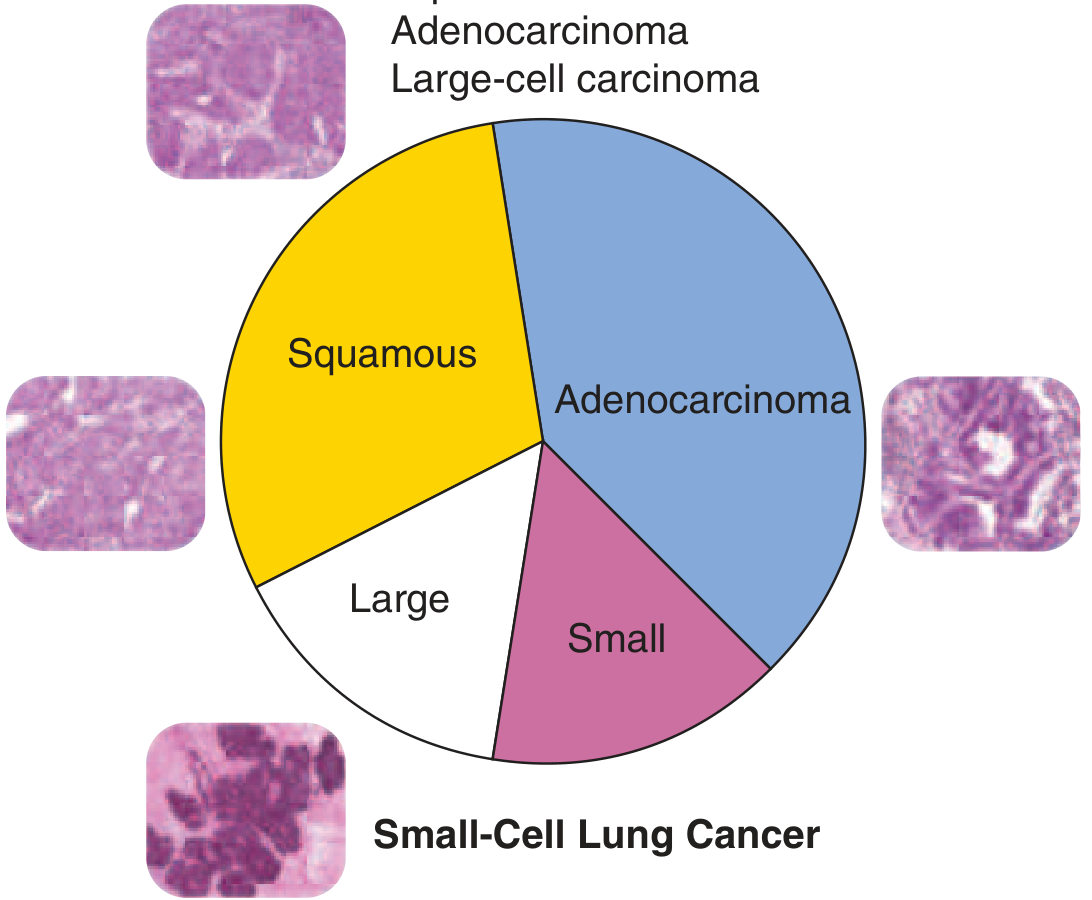
FIGURE: Histologic subsets of lung cancer - Harrison's Principles of Internal Medicine 22E, p. 659
LUNG TUMORS
│
├── PRIMARY MALIGNANT (Epithelial - Bronchogenic Carcinoma)
│ ├── NON-SMALL CELL LUNG CANCER (NSCLC) ~85%
│ │ ├── Adenocarcinoma (~40%) — most common overall
│ │ ├── Squamous Cell Carcinoma (~25-30%)
│ │ └── Large Cell Carcinoma (<10%)
│ │
│ └── SMALL CELL LUNG CANCER (SCLC) ~15%
│
├── NEUROENDOCRINE TUMORS
│ ├── Typical Carcinoid
│ ├── Atypical Carcinoid
│ ├── Large Cell Neuroendocrine Carcinoma (LCNEC)
│ └── Small Cell Lung Carcinoma (SCLC)
│
├── BENIGN TUMORS
│ ├── Hamartoma (most common benign lung tumor)
│ ├── Bronchial Adenoma
│ └── Bronchogenic Cyst
│
└── METASTATIC (Secondary)
└── Most common: Breast, Colon, Kidney, Melanoma
2. Risk Factors
| Factor | Details |
|---|---|
| Cigarette smoking | 10-fold or greater increased risk; one mutation per ~15 cigarettes; squamous and SCLC most strongly linked |
| Passive/ETS smoking | ~20-30% increased risk |
| Radon gas | Alpha irradiation; risk comparable to ETS |
| Asbestos | Occupational; synergistic with smoking |
| Other occupational | Arsenic, hexavalent chromium, nickel, bischloromethyl ether, polycyclic aromatic hydrocarbons, mustard gas |
| Ionizing radiation | Atom bomb survivors, uranium miners |
| Prior lung disease | Chronic bronchitis, emphysema, tuberculosis |
| Genetic | EGFR, KRAS, ALK, ROS1, BRAF mutations; inherited predisposition |
- Harrison's Principles of Internal Medicine 22E, pp. 1332-1336
3. Individual Tumor Types in Detail
3A. ADENOCARCINOMA
- Most common subtype in the United States and most countries
- Most frequent in never-smokers, women, younger adults (<60 years)
- Arises peripherally; shows glandular differentiation or mucin production
- Growth patterns: acinar, papillary, lepidic (formerly BAC), solid, or mixed
- 2021 WHO subtypes: adenocarcinoma in situ (AIS), minimally invasive (MIA), invasive
- Driver mutations (targetable): EGFR, ALK, KRAS, ROS1, BRAF, RET, MET, ERBB2, NTRK
- Mucinous lepidic subtype → usually KRAS-driven; signet ring subtype → ALK fusion
3B. SQUAMOUS CELL CARCINOMA
- Strongly linked to cigarette smoking (strongest correlation of all subtypes)
- Arises centrally from bronchial epithelium
- Shows keratinization and/or intercellular bridges; sheets of cells
- Produces PTH-related peptide → hypercalcemia (most common paraneoplastic endocrine syndrome)
- IHC: p40/p63 positive, TTF-1 negative
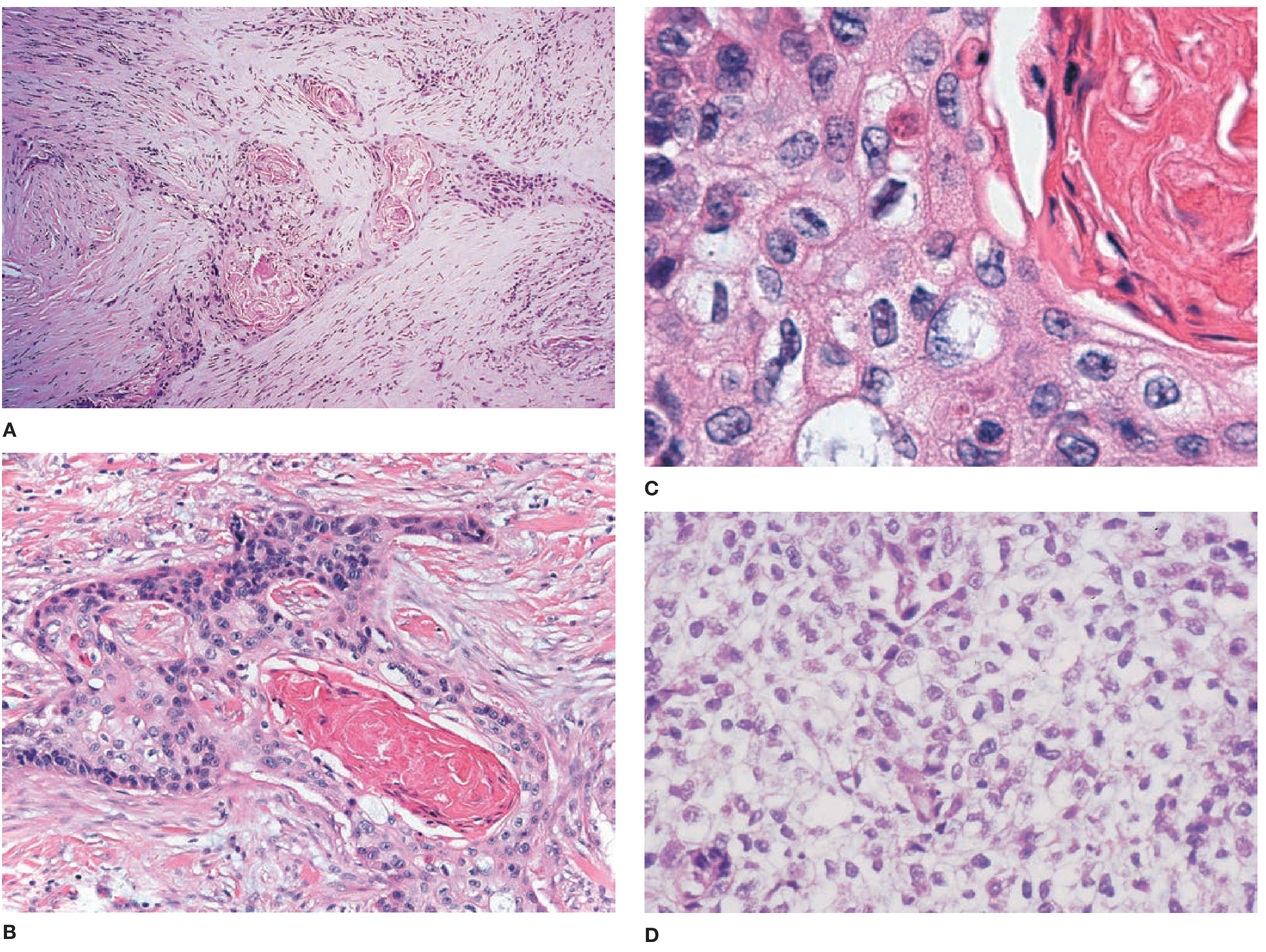
FIGURE: Squamous cell carcinoma histology. A: Desmoplastic response with infiltrating nests. B: Keratinization and intercellular bridges. C/D: High-power views - Fishman's Pulmonary Diseases, p. 1966
3C. LARGE CELL CARCINOMA
- Represents <10% of lung carcinomas
- Diagnosis of exclusion - lacks cytologic features of SCLC, glandular or squamous differentiation
- Requires morphologic examination of resected tumor + IHC
- Large cells with prominent nucleoli, moderate cytoplasm
- Most are immunophenotypically adenocarcinoma or squamous - only a small subset are truly "marker-null"
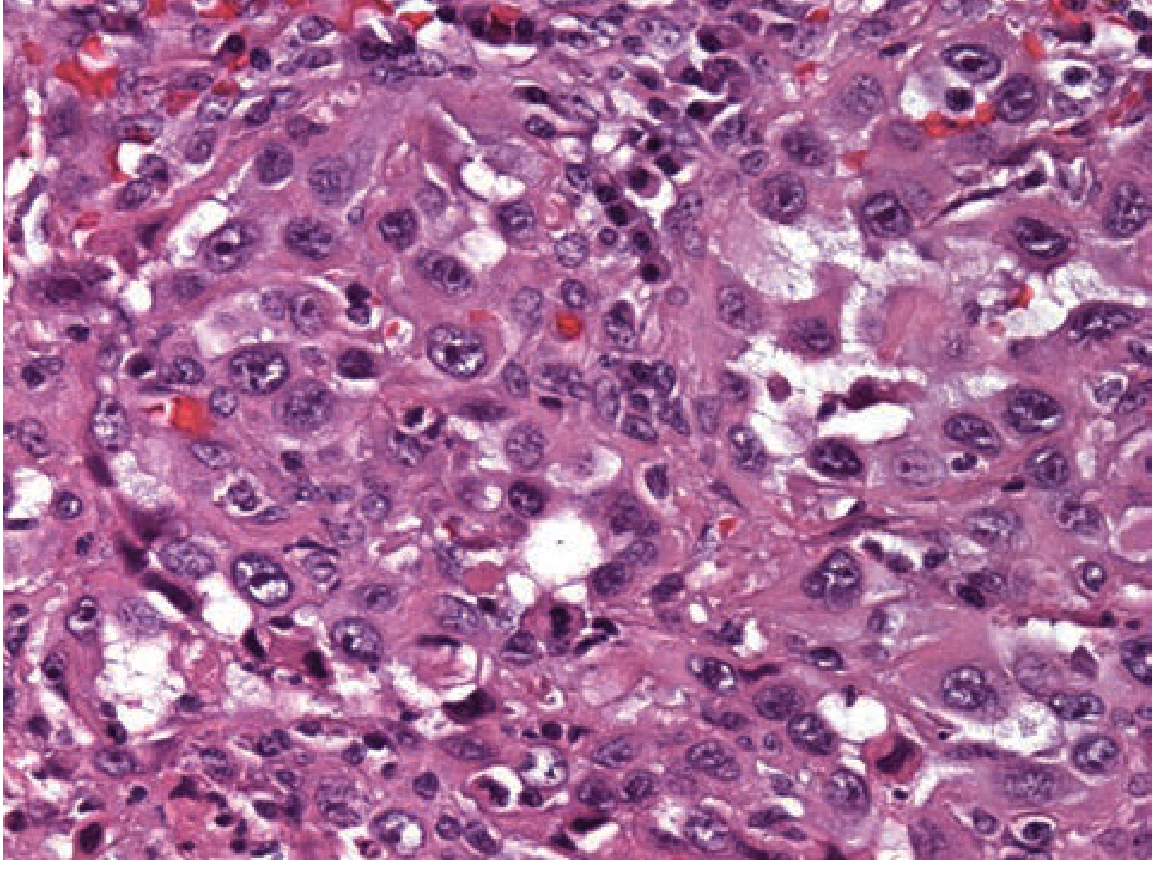
FIGURE: Large-cell carcinoma - Fishman's Pulmonary Diseases, p. 1967
3D. SMALL CELL LUNG CANCER (SCLC)
- Most aggressive lung cancer; rapid doubling time, early dissemination
- Origin: pulmonary neuroendocrine cells (Kulchitsky cells)
- Histology: small cells, scant cytoplasm, ill-defined borders, finely granular chromatin ("salt and pepper"), absent nucleoli, high mitotic rate
- IHC markers: CD56, NCAM, synaptophysin, chromogranin, INSM1
- Staged as Limited Disease (LD) vs Extensive Disease (ED) (rather than TNM)
- LD: confined to one hemithorax within a tolerable radiation field
- ED: beyond one hemithorax, including malignant pericardial/pleural effusion
- Strongly associated with paraneoplastic syndromes (see below)
4. Molecular Biomarkers & Targeted Therapy
Current guidelines mandate routine testing of NSCLC (especially non-squamous) for:
| Gene Alteration | Frequency | Primary Subtype |
|---|---|---|
| EGFR exon 19 del / L858R | ~15% NSCLC | Adenocarcinoma |
| EGFR exon 20 insertion | ~2-3% | Adenocarcinoma |
| ALK fusion | ~3-7% | Adenocarcinoma (often signet ring) |
| KRAS G12C | ~13% | Adenocarcinoma |
| ERBB2 (HER2) mutation | ~2-4% | Adenocarcinoma |
| ROS1 fusion | ~1-2% | Adenocarcinoma |
| RET fusion | ~1-2% | Adenocarcinoma |
| MET exon 14 skipping | ~3% | Adenocarcinoma |
| BRAF V600E | ~1-3% | Adenocarcinoma |
| NTRK 1/2/3 fusion | <1% | Various |
PD-L1 expression is also routinely tested to predict benefit from immune checkpoint inhibitors.
- Grainger & Allison's Diagnostic Radiology, pp. 1124-1125
5. Clinical Presentation
Symptoms by Location
CLINICAL PRESENTATION
│
├── CENTRAL TUMORS (SCC, SCLC)
│ ├── Cough, hemoptysis
│ ├── Wheezing, stridor
│ ├── Postobstructive pneumonia
│ └── Atelectasis
│
├── PERIPHERAL TUMORS (Adenocarcinoma)
│ ├── Often asymptomatic early
│ ├── Pleuritic chest pain
│ └── Pleural effusion
│
├── MEDIASTINAL INVOLVEMENT
│ ├── SVC syndrome (facial/arm swelling)
│ ├── Horner's syndrome (Pancoast tumor)
│ ├── Hoarseness (recurrent laryngeal nerve)
│ ├── Dysphagia (esophageal compression)
│ └── Phrenic nerve palsy
│
└── METASTATIC SYMPTOMS
├── Brain: headache, seizures, neuro deficits
├── Bone: pain, pathologic fractures, cord compression
├── Liver: hepatomegaly, RUQ pain
└── Adrenal: usually asymptomatic
Paraneoplastic Syndromes
| Syndrome | Tumor Type | Mechanism |
|---|---|---|
| Hypercalcemia | Squamous cell (most common) | Ectopic PTH-rP |
| SIADH | SCLC | Ectopic ADH secretion |
| Cushing's syndrome | SCLC, carcinoid | Ectopic ACTH |
| Lambert-Eaton syndrome | SCLC | Anti-VGCC antibodies |
| Clubbing / Hypertrophic osteoarthropathy | NSCLC (30%) | Unknown |
| Trousseau's syndrome (DVT) | Adenocarcinoma | Hypercoagulability |
| Subacute sensory neuropathy | SCLC | Anti-Hu antibodies |
- Harrison's Principles of Internal Medicine 22E, pp. 1477-1486
6. TNM Staging (AJCC 8th Edition - NSCLC)
TNM STAGING SYSTEM (IASLC/AJCC 8th Edition)
T - PRIMARY TUMOR
├── TX Positive cytology, no lesion identified
├── T0 No evidence of primary tumor
├── Tis Carcinoma in situ
├── T1 ≤3 cm, surrounded by lung/visceral pleura, no bronchoscopic
│ ├── T1a ≤1 cm
│ ├── T1b >1 cm, ≤2 cm
│ └── T1c >2 cm, ≤3 cm
├── T2 >3 cm, ≤5 cm OR involves main bronchus / visceral pleura / atelectasis
│ ├── T2a >3 cm, ≤4 cm
│ └── T2b >4 cm, ≤5 cm
├── T3 >5 cm, ≤7 cm OR chest wall, pericardium, phrenic nerve / satellite nodule same lobe
└── T4 >7 cm OR diaphragm, mediastinum, heart, great vessels, trachea / satellite nodule different lobe
N - REGIONAL LYMPH NODES
├── N0 No nodes
├── N1 Ipsilateral peribronchial / hilar / intrapulmonary nodes
├── N2 Ipsilateral mediastinal / subcarinal nodes
└── N3 Contralateral mediastinal/hilar OR supraclavicular/scalene nodes
M - DISTANT METASTASIS
├── M0 No distant metastasis
├── M1a Within thoracic cavity (opposite lobe, pleural/pericardial effusion)
├── M1b Single extrathoracic metastasis
└── M1c Multiple extrathoracic metastases
STAGE GROUPINGS
Stage IA1 T1a N0 M0
Stage IA2 T1b N0 M0
Stage IA3 T1c N0 M0
Stage IB T2a N0 M0
Stage IIA T2b N0 M0
Stage IIB T3 N0 M0 / T1-2 N1 M0
Stage IIIA T4 N0-1 / T1-3 N2 M0
Stage IIIB T1-2 N3 / T3-4 N2 M0
Stage IIIC T3-4 N3 M0
Stage IVA Any T, Any N, M1a or M1b
Stage IVB Any T, Any N, M1c
- Mulholland & Greenfield's Surgery 7e, p. 4271
7. Diagnostic Workup
Approach to a Solitary Pulmonary Nodule (Flowchart from Harrison's 22E)
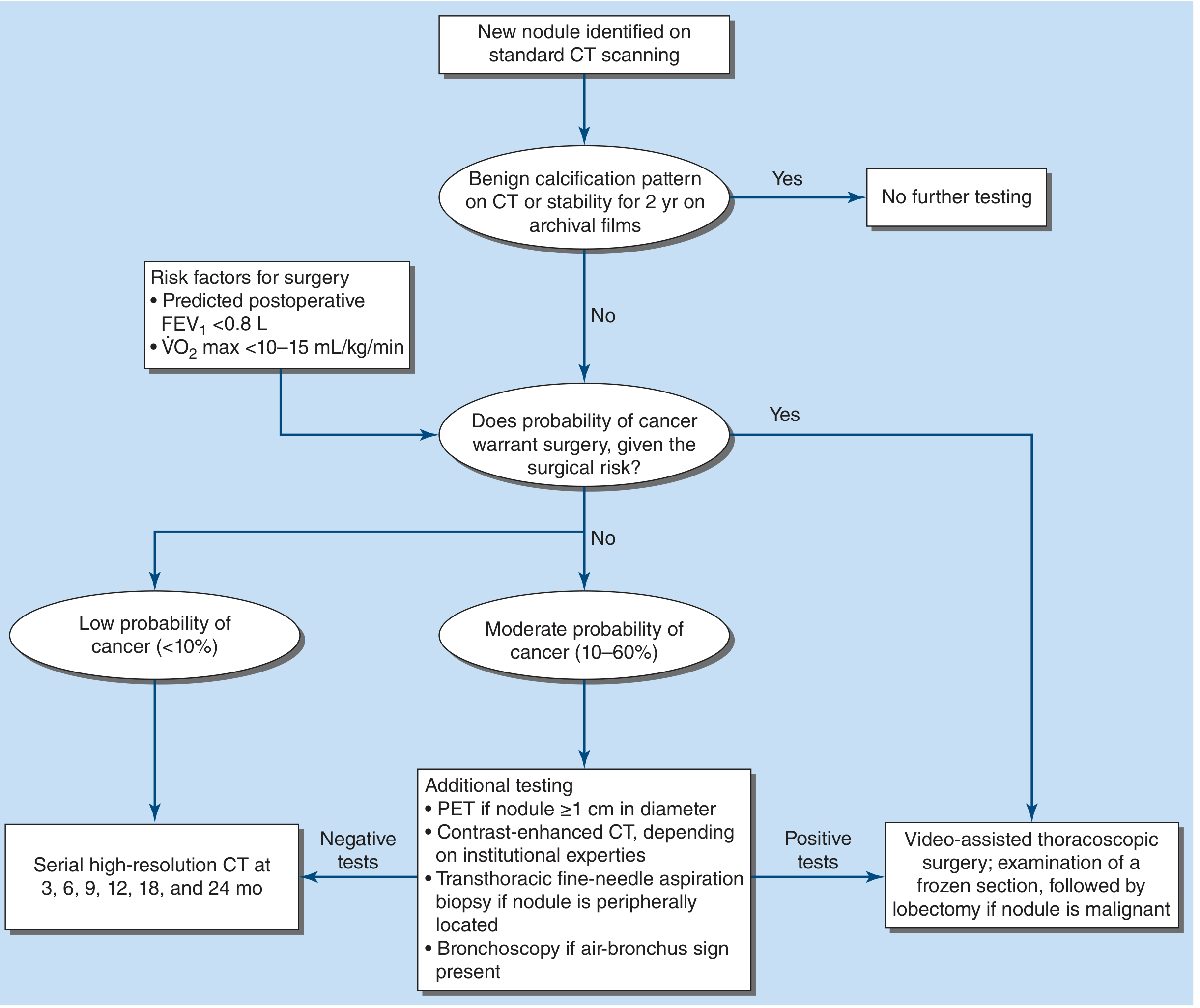
FIGURE 83-5: Approach to the solitary pulmonary nodule - Harrison's Principles of Internal Medicine 22E, p. 1617
Key principles:
- Benign calcification pattern OR stability for 2 years on archival imaging → no further testing
- Low probability (<10%) → serial HRCT at 3, 6, 9, 12, 18, and 24 months
- Moderate probability (10-60%) → PET (if ≥1 cm), contrast CT, TTNA if peripheral, bronchoscopy if air-bronchus sign
- High probability / surgical candidate → Video-assisted thoracoscopic surgery (VATS) with frozen section; lobectomy if malignant
- TTNA: sensitivity >90%, but false-negative rate up to 20-30%; 15% pneumothorax risk
8. Treatment
NSCLC Treatment by Stage
NSCLC TREATMENT ALGORITHM
│
├── Stage I-II (Resectable)
│ ├── Surgery (lobectomy preferred; segmentectomy/wedge if poor pulmonary reserve)
│ ├── Adjuvant chemotherapy (stages II-IIIA; cisplatin-based x4 cycles)
│ ├── From 2020+: Adjuvant osimertinib (EGFR+), adjuvant atezolizumab (PD-L1+)
│ └── SBRT for medically inoperable stage I
│
├── Stage IIIA-B (Locally Advanced)
│ ├── Concurrent chemoradiation (cisplatin/etoposide + RT)
│ └── Durvalumab consolidation (if no progression post-CRT, PD-L1 ≥1%)
│
└── Stage IV (Metastatic)
├── Test for driver mutations → Targeted therapy (TKI)
└── If driver-negative → Immunotherapy ± chemotherapy by PD-L1 and histology
Targeted Therapy Flowchart for Stage IV NSCLC (from Harrison's 22E)
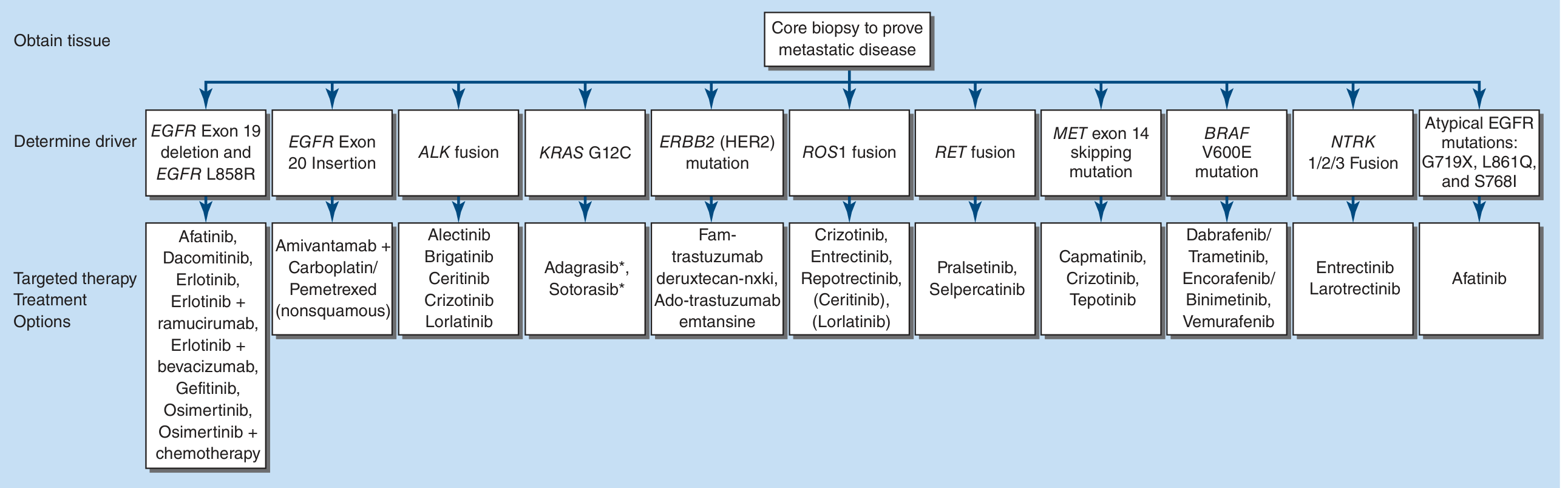
FIGURE 83-6: Targeted therapy by driver mutation - Harrison's Principles of Internal Medicine 22E, p. 1759
Immunotherapy Flowchart - Stage IV Driver-Mutation-Negative NSCLC
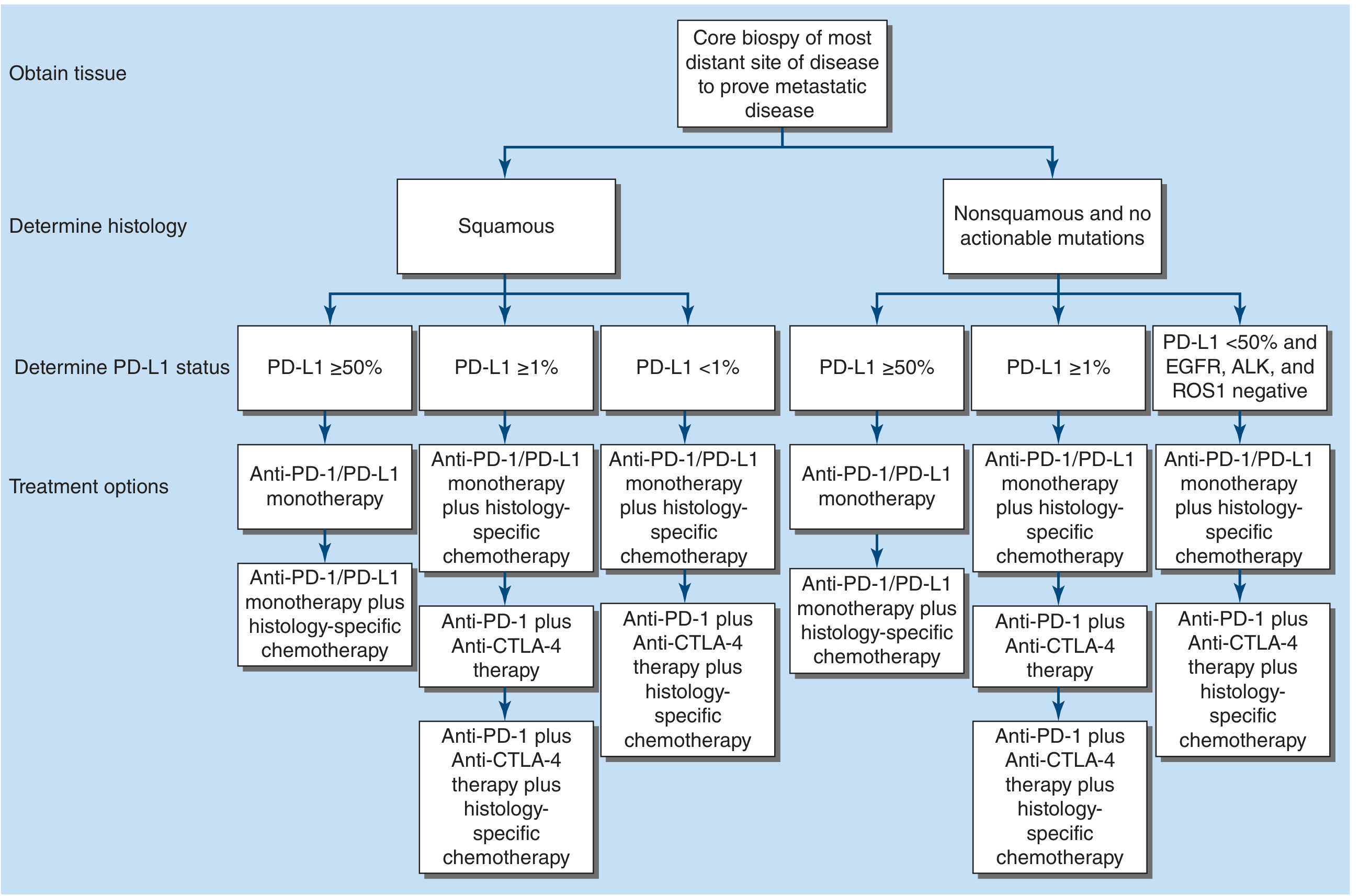
FIGURE 83-7: First-line therapy for stage IV, driver mutation-negative NSCLC by PD-L1 and histology - Harrison's Principles of Internal Medicine 22E, p. 1766
SCLC Treatment Algorithm (from Harrison's 22E)
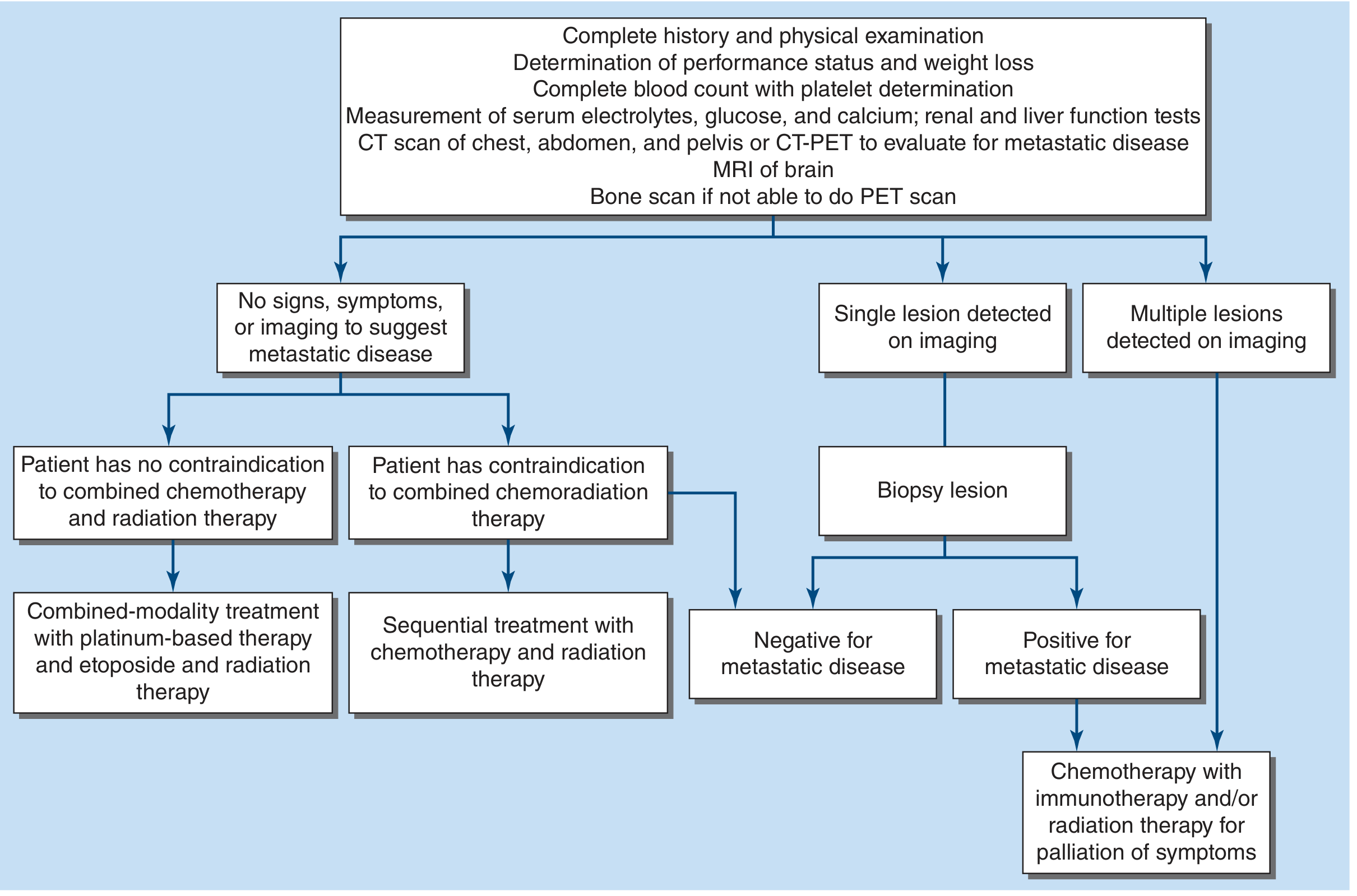
FIGURE 83-8: Algorithm for management of SCLC - Harrison's Principles of Internal Medicine 22E
SCLC Chemotherapy:
- Limited disease: Concurrent cisplatin + etoposide x4 cycles + thoracic RT → standard of care for >40 years. Adding atezolizumab or durvalumab to chemo now preferred in appropriate patients.
- Extensive disease: Carboplatin/etoposide + atezolizumab (IMpower133) or durvalumab (CASPIAN); superior PFS and OS vs chemo alone.
- Median survival: 12-20 months (LD), ~12 months (ED); despite 80% initial response rates, almost all relapse.
- Second-line: Topotecan (IV or oral) or lurbinectedin (35% response rate).
- PCI (Prophylactic Cranial Irradiation): Reduces brain metastasis risk in responders; controversial in ED.
9. Chemotherapy by Histology (NSCLC)
| Regimen | Best For |
|---|---|
| Cisplatin + pemetrexed | Non-squamous (adenocarcinoma) - higher TS expression in squamous makes pemetrexed less effective |
| Cisplatin + gemcitabine | Squamous cell carcinoma |
| Carboplatin (substitution) | Renal impairment, neuropathy, hearing loss |
| Adjuvant cisplatin-based x4 cycles | Stage II-IIIA resected NSCLC |
10. Summary Comparison Table
| Feature | Adenocarcinoma | Squamous Cell | Large Cell | SCLC |
|---|---|---|---|---|
| Frequency | ~40% | ~25-30% | <10% | ~15% |
| Location | Peripheral | Central | Peripheral | Central |
| Smoking link | Moderate | Strong | Moderate | Strongest |
| Common in never-smokers | Yes | No | No | No |
| Key driver mutations | EGFR, ALK, KRAS | FGFR1, DDR2 | None specific | TP53, RB1 |
| IHC markers | TTF-1, Napsin A | p40, p63 | Exclusion | CD56, Synaptophysin |
| Key paraneoplastic | DVT/PE | Hypercalcemia | - | SIADH, Cushing's, Lambert-Eaton |
| Staging | TNM | TNM | TNM | LD/ED |
| Surgery role | Yes (early stage) | Yes (early stage) | Yes (early stage) | Limited (stage I only) |
11. Screening
- Low-dose CT (LDCT) screening is recommended for:
- Age 50-80 years
- ≥20 pack-year smoking history
- Currently smoking or quit within the past 15 years
- Reduces lung cancer mortality by ~20% in high-risk populations (National Lung Screening Trial)
Key Takeaways
- Adenocarcinoma is now the most common lung cancer subtype, having surpassed squamous cell over the past 30 years due to changes in smoking habits.
- The critical first distinction is SCLC vs NSCLC - they have fundamentally different biology, staging systems, and treatment approaches.
- All advanced NSCLC should have molecular profiling before starting systemic therapy - targeted TKIs can be dramatically more effective than chemotherapy for driver-positive tumors.
- PD-L1 expression and histology (squamous vs non-squamous) drive first-line immunotherapy decisions in driver-mutation-negative NSCLC.
- SCLC, despite high initial chemotherapy response rates (up to 80%), almost universally relapses, making it one of the most challenging malignancies to treat.
This is a shared conversation. Sign in to Orris to start your own chat.