Management protocol and opd prescription for 5 years old baby with history of head truma. Ct scan wnl .
minor head injury children management
Management of Minor Head Trauma in a 5-Year-Old with Normal CT Scan
Clinical Context
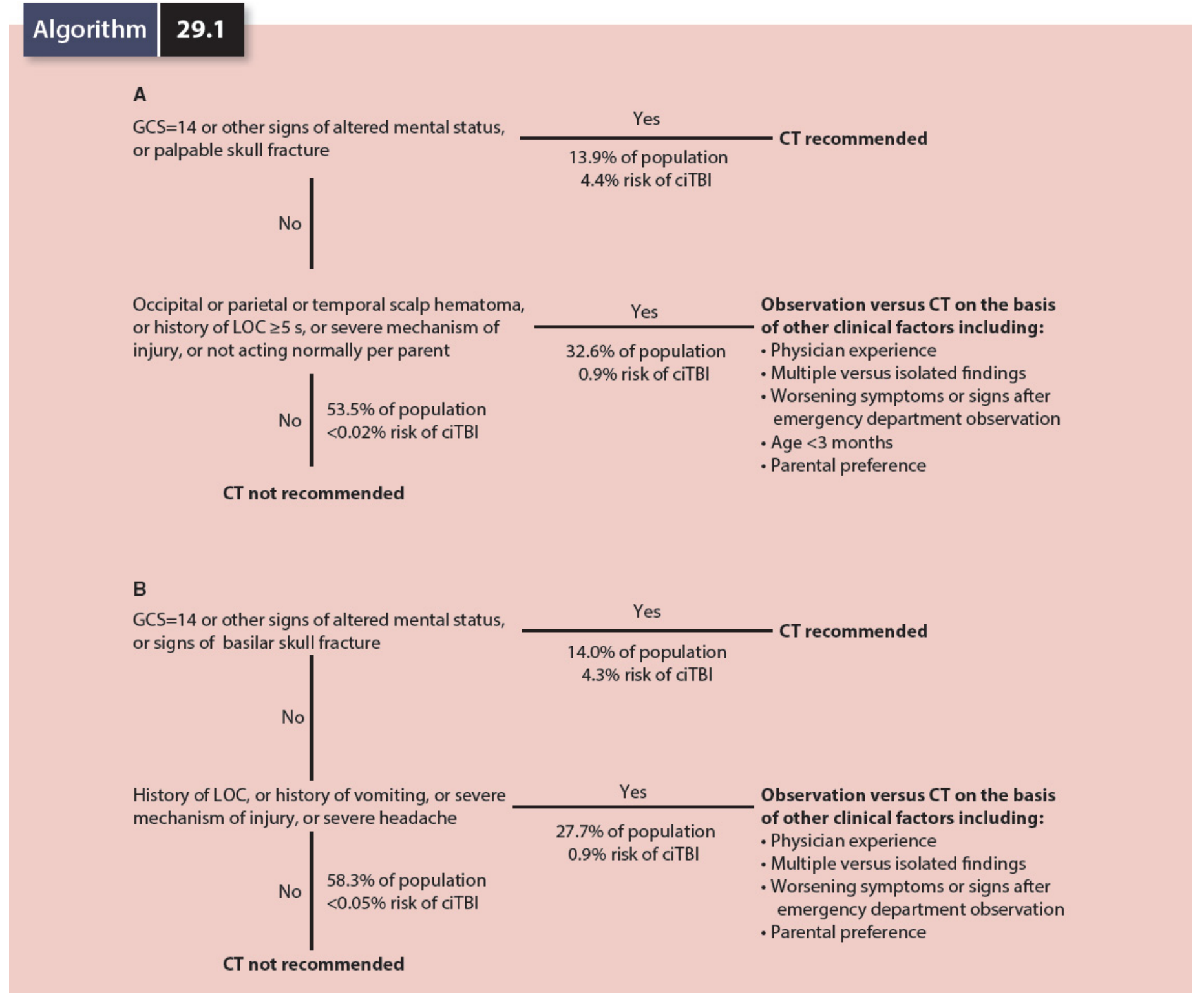
PECARN Decision Framework (for context / future reference)
EMERGENCY DEPARTMENT / INITIAL MANAGEMENT
1. Immediate Assessment
- GCS (should be 15 in a child with normal CT and no ongoing deficit)
- Neurological exam: pupils, focal deficits, cerebellar signs
- Scalp inspection: lacerations, hematoma size/location
- Rule out non-accidental injury (NAI): ensure mechanism matches developmental stage; look for bruising outside typical accident distribution
2. Observation Period in ED
- Minimum 4–6 hours of observation recommended after any head injury in a child
- Monitor: GCS every 30 min, pupillary response, vomiting, behavior
- If the child remains GCS 15, neurologically intact, tolerating fluids → eligible for discharge
3. Criteria to ADMIT (do NOT discharge if any present)
| Red Flag | Action |
|---|---|
| GCS declining or persistently <15 | Admit + neurosurgery consult |
| Repeated vomiting (≥4 episodes) | Admit for observation |
| Worsening headache not responding to analgesia | Admit |
| Seizure | Admit |
| Abnormal behavior or drowsiness | Admit |
| Suspected NAI | Admit + safeguarding |
OPD PRESCRIPTION / DISCHARGE PLAN
Medications
| Drug | Dose | Route | Frequency | Duration |
|---|---|---|---|---|
| Paracetamol (Acetaminophen) | 15 mg/kg/dose | Oral | Every 6 hours PRN | 3–5 days |
| Ibuprofen | 10 mg/kg/dose | Oral | Every 8 hours PRN (with food) | 3–5 days |
Note: Do NOT prescribe opioids, sedatives, or antiemetics (metoclopramide) routinely — they mask neurological deterioration. Avoid aspirin in children.
Symptomatic Management
- Headache: Paracetamol ± Ibuprofen as above
- Nausea/vomiting (if present): Ondansetron 0.15 mg/kg oral (max 4 mg) — single dose only if needed; reassess if vomiting is persistent
- Sleep: Normal sleep is safe and should not be withheld; parents should do a brief check at 4–6 hours after the child falls asleep (not every 15 minutes — this is outdated advice)
DISCHARGE INSTRUCTIONS FOR PARENTS
Return to ED IMMEDIATELY if child develops:
- Difficulty waking or cannot be roused
- Repeated vomiting (3 or more times)
- Seizure (any convulsive activity)
- Worsening or severe headache not relieved by paracetamol
- Unusual behavior, confusion, or agitation
- Weakness, numbness, or difficulty walking
- Unequal pupils or blurred/double vision
- Clear fluid from nose or ear
Activity Restrictions (Return-to-Learn / Return-to-Play Protocol)
| Stage | Activity | Timing |
|---|---|---|
| 1 | Rest (24–48 hrs), limit screen time | Day 1–2 |
| 2 | Light cognitive activity (reading, quiet play) | Day 2–3 |
| 3 | School return (half-day initially if needed) | Day 3–5 |
| 4 | Light physical activity (walking, no contact) | After symptom-free at school |
| 5 | Full return to school and non-contact sport | Symptom-free ≥1 day at each stage |
| 6 | Full return to contact sports | After medical clearance |
Do NOT rush return to contact sport. Each stage requires minimum 24 hours symptom-free before progressing.
OPD FOLLOW-UP SCHEDULE
| Visit | When | Purpose |
|---|---|---|
| 1st follow-up | 24–48 hours (phone or clinic) | Check symptom resolution, behavior, sleep |
| 2nd follow-up | Day 7–10 | Assess for post-concussion symptoms |
| 3rd follow-up | Day 28 (if symptoms persist) | Screen for Post-Concussion Syndrome |
| Neurology referral | If symptoms >4 weeks or GCS was 13 | Formal neuropsychological assessment |
POST-CONCUSSION SYNDROME (Watch For)
- Persistent headache
- Poor concentration or school performance drop
- Sleep disturbance, irritability, mood changes
- → Refer to pediatric neurology or concussion clinic
KEY TEACHING POINTS
- Normal CT does NOT rule out concussion — CT is normal by definition in concussion; it only rules out structural injury (bleed, fracture)
- Children (≥2 yrs) with normal CT and GCS 14–15 can be safely discharged with strict return precautions (Mulholland & Greenfield's Surgery 7e, p. 1439)
- Cognitive and physical rest in the first 24–48 hours, then graduated return
- NAI must always be considered — ensure mechanism is consistent with the child's developmental stage (Bailey & Love's Surgery 28e, p. 391)
- Do NOT wake child every hour at night — this is outdated; a single check at 4–6 hrs post-sleep is sufficient
Create a discharge handout/summary I can give to parents
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not foun…
mkdir -p /home/daytona/workspace/head-trauma-handout
~/head-trauma-handout/create_handout.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
AlignmentType, HeadingLevel, BorderStyle, WidthType, ShadingType,
VerticalAlign, UnderlineType
} = require('docx');
const fs = require('fs');
// ── helpers ──────────────────────────────────────────────────────────────────
const DARK_BLUE = "1B3A6B";
const MED_BLUE = "2E6DA4";
const LIGHT_BLUE = "D6E4F0";
const RED = "C0392B";
const RED_LIGHT = "FDECEA";
const GREEN = "1A7A4A";
const GREEN_LIGHT= "E8F6EE";
const AMBER = "B7621A";
const AMBER_LIGHT= "FEF3E2";
const GREY_LIGHT = "F4F6F9";
const WHITE = "FFFFFF";
const BORDER_NONE = { style: BorderStyle.NONE, size: 0, color: "FFFFFF" };
function heading(text, color = DARK_BLUE, size = 26) {
return new Paragraph({
spacing: { before: 240, after: 80 },
children: [new TextRun({ text, bold: true, size, color, font: "Calibri" })]
});
}
function subheading(text, color = MED_BLUE) {
return new Paragraph({
spacing: { before: 160, after: 60 },
children: [new TextRun({ text, bold: true, size: 22, color, font: "Calibri" })]
});
}
function body(text, bold = false, color = "222222") {
return new Paragraph({
spacing: { before: 40, after: 40 },
children: [new TextRun({ text, bold, size: 20, color, font: "Calibri" })]
});
}
function bullet(text, bold = false, color = "222222") {
return new Paragraph({
bullet: { level: 0 },
spacing: { before: 30, after: 30 },
children: [new TextRun({ text, bold, size: 20, color, font: "Calibri" })]
});
}
function redBullet(text) {
return new Paragraph({
bullet: { level: 0 },
spacing: { before: 30, after: 30 },
children: [new TextRun({ text, bold: true, size: 20, color: RED, font: "Calibri" })]
});
}
function divider(color = LIGHT_BLUE) {
return new Paragraph({
spacing: { before: 80, after: 80 },
border: { bottom: { style: BorderStyle.SINGLE, size: 6, color } }
});
}
function shaded(children, fill = LIGHT_BLUE) {
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: {
top: BORDER_NONE, bottom: BORDER_NONE,
left: BORDER_NONE, right: BORDER_NONE,
insideH: BORDER_NONE, insideV: BORDER_NONE
},
rows: [new TableRow({
children: [new TableCell({
shading: { fill, type: ShadingType.CLEAR },
margins: { top: 100, bottom: 100, left: 180, right: 180 },
borders: {
top: BORDER_NONE, bottom: BORDER_NONE,
left: BORDER_NONE, right: BORDER_NONE
},
children
})]
})]
});
}
// ── colored table helper ─────────────────────────────────────────────────────
function makeTable(headers, rows, headerFill = DARK_BLUE, altFill = GREY_LIGHT) {
const headerRow = new TableRow({
tableHeader: true,
children: headers.map(h =>
new TableCell({
shading: { fill: headerFill, type: ShadingType.CLEAR },
verticalAlign: VerticalAlign.CENTER,
margins: { top: 80, bottom: 80, left: 120, right: 120 },
children: [new Paragraph({
alignment: AlignmentType.CENTER,
children: [new TextRun({ text: h, bold: true, size: 18, color: WHITE, font: "Calibri" })]
})]
})
)
});
const dataRows = rows.map((row, idx) =>
new TableRow({
children: row.map(cell =>
new TableCell({
shading: { fill: idx % 2 === 0 ? WHITE : altFill, type: ShadingType.CLEAR },
verticalAlign: VerticalAlign.CENTER,
margins: { top: 70, bottom: 70, left: 120, right: 120 },
children: [new Paragraph({
children: [new TextRun({ text: cell, size: 18, font: "Calibri", color: "222222" })]
})]
})
)
})
);
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [headerRow, ...dataRows]
});
}
// ── document ─────────────────────────────────────────────────────────────────
const doc = new Document({
creator: "Orris Medical",
title: "Head Injury Discharge Handout",
sections: [{
properties: {
page: {
margin: { top: 720, bottom: 720, left: 900, right: 900 }
}
},
children: [
// ── TITLE BLOCK ─────────────────────────────────────────────────────
shaded([
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 80, after: 40 },
children: [new TextRun({ text: "🏥 DISCHARGE INSTRUCTIONS", bold: true, size: 32, color: DARK_BLUE, font: "Calibri" })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 80 },
children: [new TextRun({ text: "Head Injury in Children — What Parents Need to Know", bold: false, size: 22, color: MED_BLUE, font: "Calibri" })]
})
], LIGHT_BLUE),
new Paragraph({ spacing: { before: 120, after: 0 }, children: [] }),
// ── GOOD NEWS BOX ───────────────────────────────────────────────────
shaded([
new Paragraph({
spacing: { before: 60, after: 40 },
children: [new TextRun({ text: "✔ Good News", bold: true, size: 22, color: GREEN, font: "Calibri" })]
}),
new Paragraph({
spacing: { before: 0, after: 60 },
children: [new TextRun({
text: "Your child's CT scan of the head is NORMAL. There is no bleeding or serious structural injury in the brain. However, a head knock can still cause a temporary problem called a concussion, and your child needs rest and monitoring at home for the next 24–48 hours.",
size: 20, color: "222222", font: "Calibri"
})]
})
], GREEN_LIGHT),
new Paragraph({ spacing: { before: 120, after: 0 }, children: [] }),
// ── SECTION 1: MEDICINES ────────────────────────────────────────────
shaded([
heading("💊 Medicines Prescribed", DARK_BLUE, 24)
], LIGHT_BLUE),
new Paragraph({ spacing: { before: 80, after: 0 }, children: [] }),
makeTable(
["Medicine", "Dose", "How Often", "With Food?", "Duration"],
[
["Paracetamol (Calpol / Tylenol)", "15 mg/kg per dose", "Every 6 hours IF in pain", "Not required", "Up to 5 days"],
["Ibuprofen (Nurofen)", "10 mg/kg per dose", "Every 8 hours IF in pain", "Always with food", "Up to 5 days"]
]
),
new Paragraph({ spacing: { before: 100, after: 0 }, children: [] }),
shaded([
body("⚠ Do NOT give both medicines at the same time unless advised by your doctor.", true, AMBER),
body("⚠ Do NOT give aspirin to children.", true, AMBER),
body("⚠ Only give medicines when your child is uncomfortable — not on a fixed schedule.", false, "444444"),
], AMBER_LIGHT),
new Paragraph({ spacing: { before: 120, after: 0 }, children: [] }),
// ── SECTION 2: REST & ACTIVITY ───────────────────────────────────────
shaded([
heading("🛌 Rest & Activity Guide", DARK_BLUE, 24)
], LIGHT_BLUE),
new Paragraph({ spacing: { before: 80, after: 0 }, children: [] }),
makeTable(
["Stage", "Activity Allowed", "When to Start"],
[
["1 — Complete Rest", "Quiet time, no screens, no homework", "Day 1–2"],
["2 — Light Activity", "Reading, gentle play, short screen time", "Day 2–3 (if no headache)"],
["3 — Back to School", "Return to school (half-day if needed)", "Day 3–5 (if symptom-free)"],
["4 — Light Exercise", "Walking, cycling — NO contact sports", "After fully back to school"],
["5 — Full Return", "All activities including sport", "Only after medical clearance"]
]
),
new Paragraph({ spacing: { before: 100, after: 0 }, children: [] }),
body("⚠ Do NOT rush return to contact sports. Each stage needs at least 1 symptom-free day before moving on.", true, AMBER),
new Paragraph({ spacing: { before: 120, after: 0 }, children: [] }),
// ── SECTION 3: SLEEP ─────────────────────────────────────────────────
shaded([
heading("😴 Sleep — What is Safe?", DARK_BLUE, 24)
], LIGHT_BLUE),
new Paragraph({ spacing: { before: 80, after: 40 }, children: [] }),
body("✔ It is SAFE for your child to sleep after a head injury with a normal CT."),
body("✔ You do NOT need to wake them every hour — this is old advice and is no longer recommended."),
body("✔ Do ONE check 4–6 hours after they fall asleep. If you can rouse them and they respond normally, they are fine."),
new Paragraph({ spacing: { before: 120, after: 0 }, children: [] }),
// ── SECTION 4: RED FLAGS ─────────────────────────────────────────────
shaded([
heading("🚨 GO TO EMERGENCY IMMEDIATELY IF YOUR CHILD HAS:", RED, 24)
], RED_LIGHT),
new Paragraph({ spacing: { before: 80, after: 40 }, children: [] }),
redBullet("Cannot be woken up / very hard to rouse"),
redBullet("Vomiting 3 or more times"),
redBullet("A seizure / convulsion / shaking fit"),
redBullet("Worsening or very severe headache not relieved by paracetamol"),
redBullet("Confusion, strange behaviour, or does not recognise you"),
redBullet("Weakness or numbness in arms or legs, difficulty walking"),
redBullet("Unequal pupil sizes, blurred or double vision"),
redBullet("Clear or blood-stained fluid from the nose or ear"),
redBullet("Neck pain or stiffness"),
new Paragraph({ spacing: { before: 120, after: 0 }, children: [] }),
// ── SECTION 5: WHAT TO EXPECT ────────────────────────────────────────
shaded([
heading("📋 What to Expect at Home", DARK_BLUE, 24)
], LIGHT_BLUE),
new Paragraph({ spacing: { before: 80, after: 40 }, children: [] }),
body("These symptoms are NORMAL after a head injury and usually resolve within 1–2 weeks:"),
new Paragraph({ spacing: { before: 20, after: 0 }, children: [] }),
bullet("Headache (mild to moderate)"),
bullet("Tiredness or wanting to sleep more than usual"),
bullet("One episode of vomiting"),
bullet("Grumpiness or being emotional"),
bullet("Difficulty concentrating or feeling 'foggy'"),
bullet("Sensitivity to light or noise"),
new Paragraph({ spacing: { before: 60, after: 0 }, children: [] }),
body("These symptoms should gradually improve each day. If they are getting WORSE or not improving after 1 week, see your doctor.", true, AMBER),
new Paragraph({ spacing: { before: 120, after: 0 }, children: [] }),
// ── SECTION 6: FOLLOW-UP ─────────────────────────────────────────────
shaded([
heading("📅 Follow-Up Appointments", DARK_BLUE, 24)
], LIGHT_BLUE),
new Paragraph({ spacing: { before: 80, after: 0 }, children: [] }),
makeTable(
["Visit", "When", "Purpose"],
[
["1st Follow-up", "24–48 hours", "Check for worsening symptoms, sleep, and behavior"],
["2nd Follow-up", "Day 7–10", "Confirm recovery, clear for school and activity"],
["3rd Visit (if needed)", "Day 28", "If symptoms still present — further assessment"]
]
),
new Paragraph({ spacing: { before: 120, after: 0 }, children: [] }),
// ── SECTION 7: DIET ──────────────────────────────────────────────────
shaded([
heading("🥤 Diet & Fluids", DARK_BLUE, 24)
], LIGHT_BLUE),
new Paragraph({ spacing: { before: 80, after: 40 }, children: [] }),
bullet("Start with small amounts of clear fluids (water, diluted juice) if your child was vomiting"),
bullet("Progress to normal diet as tolerated once vomiting stops"),
bullet("Ensure adequate hydration — aim for frequent small sips if feeling nauseous"),
bullet("Avoid caffeinated drinks (cola, energy drinks)"),
new Paragraph({ spacing: { before: 120, after: 0 }, children: [] }),
// ── FOOTER ───────────────────────────────────────────────────────────
divider(DARK_BLUE),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 80, after: 40 },
children: [new TextRun({
text: "If you are ever unsure, do not wait — seek medical attention. Your child's safety comes first.",
bold: true, italics: true, size: 20, color: DARK_BLUE, font: "Calibri"
})]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 40 },
children: [new TextRun({
text: "Doctor: ________________________ Date: ________________ Hospital/Clinic: ________________________",
size: 18, color: "666666", font: "Calibri"
})]
}),
]
}]
});
Packer.toBuffer(doc).then(buffer => {
fs.writeFileSync("/home/daytona/workspace/head-trauma-handout/Head_Injury_Discharge_Handout.docx", buffer);
console.log("Done.");
});
cd /home/daytona/workspace/head-trauma-handout && node create_handout.js 2>&1
python3 /home/daytona/skills/docx/scripts/office/validate.py /home/daytona/works…
python3 -c " import zipfile, sys path = '/home/daytona/workspace/head-trauma-han…
Head Injury Discharge Handout
Word Document · DOCX
| Section | Content |
|---|---|
| Good News Box | Reassures parents the CT is normal, explains concussion in plain language |
| Medicines Table | Paracetamol & Ibuprofen with exact doses, frequency, food instructions |
| Activity Guide Table | 5-stage return-to-school/sport stepwise plan |
| Sleep Advice | Clears up the "wake every hour" myth with the correct 4–6 hr check advice |
| 🚨 Red Flags | Bold red section — 9 emergency warning signs to return immediately |
| What to Expect | Normal vs abnormal symptoms — reduces unnecessary ED re-visits |
| Follow-Up Schedule | 3 follow-up visits with timing and purpose |
| Diet & Fluids | Simple eating advice post-vomiting |
| Doctor Sign-off Line | Space for your name, date, and clinic at the bottom |
The pt with history of head truma has already been over 48 hours and pt has normal ct scan . Write me a OPD prescription and tell me how to explain concussion and post concussion syndrome to parents
5-Year-Old, Head Trauma >48 Hours, Normal CT — OPD Visit
CLINICAL CONTEXT AT THIS VISIT
- Confirming there are no red-flag neurological signs
- Treating ongoing concussion symptoms (headache, nausea, dizziness, fatigue, irritability)
- Screening for persistent post-concussion symptoms (1 in 3 children will have symptoms beyond 4 weeks)
- Guiding a safe graduated return to school and play
- Counselling parents clearly about concussion and post-concussion syndrome
OPD PRESCRIPTION
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
OPD PRESCRIPTION
Age: 5 years | Weight: ~18–20 kg (approx)
Diagnosis: Post-Concussion State (S09.90)
Day post-injury: >48 hours | CT Head: Normal
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Rx — Symptomatic (give only for active symptoms, not on a fixed schedule)
| # | Drug | Dose & Route | Frequency | Duration |
|---|---|---|---|---|
| 1 | Tab/Syrup Paracetamol | 15 mg/kg/dose oral | Every 6 hrs PRN (headache) | 5–7 days |
| 2 | Syrup Ibuprofen | 10 mg/kg/dose oral | Every 8 hrs PRN (with food) | 5 days |
| 3 | Syrup Ondansetron | 0.15 mg/kg/dose oral | Once PRN (only for vomiting/nausea) | Max 3 days |
| 4 | Syrup Melatonin (if sleep disturbed) | 0.5–1 mg oral | At bedtime | 2–4 weeks |
Do NOT prescribe: Opioids, benzodiazepines, antihistamines for sedation, or NSAIDs beyond 5 days. Ibuprofen overuse warning: If headache is occurring daily, stop ibuprofen after day 5 — analgesic overuse (>10 days/month) can perpetuate post-concussion headache.
Advice written on prescription
- Physical rest: Light activity only. No running, jumping, contact play, PE class until symptom-free
- Cognitive rest: Limit screen time to <1 hr/day; no homework if causing headache
- School: May return in 3–5 days if symptom-free; start with half-days
- Review: Return OPD in 7–10 days, or sooner if symptoms worsen
HOW TO EXPLAIN CONCUSSION TO PARENTS
What to say (plain language script you can use in clinic):
"Your child's brain is like a bowl of jelly inside a hard shell. When the head gets a hard knock, the jelly inside shakes and wobbles — even if the shell (skull) is not cracked and even if the X-ray or scan looks perfectly normal. This shaking temporarily disrupts the chemical signals in the brain — we call this a concussion. It is not a structural injury. Nothing is torn or bleeding. But the brain cells are temporarily working in a disturbed way and need time and rest to recover — exactly like a sprained ankle needs rest before you walk on it again."
Key points to reinforce:
| Point | What to tell parents |
|---|---|
| Normal CT does NOT mean nothing happened | "The scan shows no bleeding or fracture, which is excellent — but concussion is an invisible injury the scan cannot see" |
| Symptoms are real, not imaginary | "The headache, tiredness, and grumpiness your child has are real brain symptoms, not making it up or being naughty" |
| Recovery takes time | "Most children are fully better in 2–4 weeks. Some take longer — that is normal" |
| Rest is medicine | "The best treatment right now is rest — both body and brain rest. Pushing through makes it last longer" |
| School can wait briefly | "A few days off school now is far better than weeks off later if he/she goes back too soon" |
HOW TO EXPLAIN POST-CONCUSSION SYNDROME (PCS)
When to bring it up
- Symptoms already present for 2+ days
- ~1 in 3 children develop persistent symptoms beyond 4 weeks (Tintinalli's Emergency Medicine, Ch. 111)
- Early counselling prevents catastrophising and reduces anxiety-driven symptom amplification
Plain language explanation for parents:
"Most children fully recover within 2 to 4 weeks. However, in about 1 out of every 3 children, some symptoms like headaches, difficulty concentrating, tiredness, or mood changes continue for longer than a month. When that happens, we call it Post-Concussion Syndrome. It does NOT mean the brain is permanently damaged. It means the recovery is taking longer than usual. Think of it like a bad sprain that takes longer to heal in some people — the injury itself wasn't worse, the healing is just slower. We manage it the same way — with graded rest, gradual return, and targeted treatment for each symptom. With proper care, almost all children make a full recovery."
Symptoms of PCS to watch for (give this list to parents):
- Persistent or daily headache
- Dizziness, feeling off-balance
- Nausea, light-headedness
- Sensitivity to light or noise
- Poor concentration, "foggy" feeling
- Forgetting things easily
- Difficulty following instructions
- Drop in school performance
- Irritability, crying easily
- Anxiety, clinginess
- Low mood, withdrawn
- More emotional than usual
- Sleeping too much or too little
- Trouble falling asleep
Risk factors for prolonged recovery — warn parents if present:
- Previous concussions
- Pre-existing anxiety, ADHD, or learning difficulties
- Migraine history
- High symptom burden in first 24–48 hours
- Female gender (slightly higher risk)
- Returned to sport before symptoms fully cleared
FOLLOW-UP PLAN
| Visit | Timing | What to Check |
|---|---|---|
| Review 1 | Day 7–10 | Symptom score, school return progress, sleep |
| Review 2 | Day 28 | If any symptoms persist → formal PCS screening |
| Refer: Paediatric Neurology / Concussion Clinic | If symptoms >4 weeks | Multidisciplinary assessment — physiotherapy, neuropsychology, neuro-ophthalmology |
⚠ SECOND IMPACT SYNDROME — WARN PARENTS
"Your child must NOT return to any contact sports or rough play until he/she is completely symptom-free. If the brain receives a second injury before it has healed, a rare but dangerous condition called Second Impact Syndrome can occur, causing severe brain swelling. It has a 50% mortality rate. We will only clear your child for full sport after a stepwise return programme is completed."
Write a prescription if the patient is old female