Explain stroke syndromes in great detail including images, tables, flowchart References - Tintinalli's 9th edition & Rosen's 10th edition
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Reading File
Stroke Syndromes - Comprehensive Review
Sources: Tintinalli's Emergency Medicine, 9th Ed. (Chapter 167, Steven Go) & Rosen's Emergency Medicine, 10th Ed. (Chapter 87, Linda Papa & William J. Meurer)
1. Epidemiology & Overview
- 795,000 strokes/year in the United States (one stroke every 40 seconds; one death every 4 minutes)
- 77% are first-ever strokes; 23% recurrent
- Ischemic strokes: 87% of all strokes
- Intracerebral hemorrhage (ICH): 10%
- Subarachnoid hemorrhage (SAH): 3%
- Age-adjusted stroke death rate fell 28.7% from 2004-2014 with improved stroke units, thrombolysis, and thrombectomy
(Tintinalli's, Ch. 167)
2. Vascular Anatomy - The Essential Framework
Figure 167-1. Cerebral Hemisphere, Lateral Aspect - MCA branches and cortical localization:
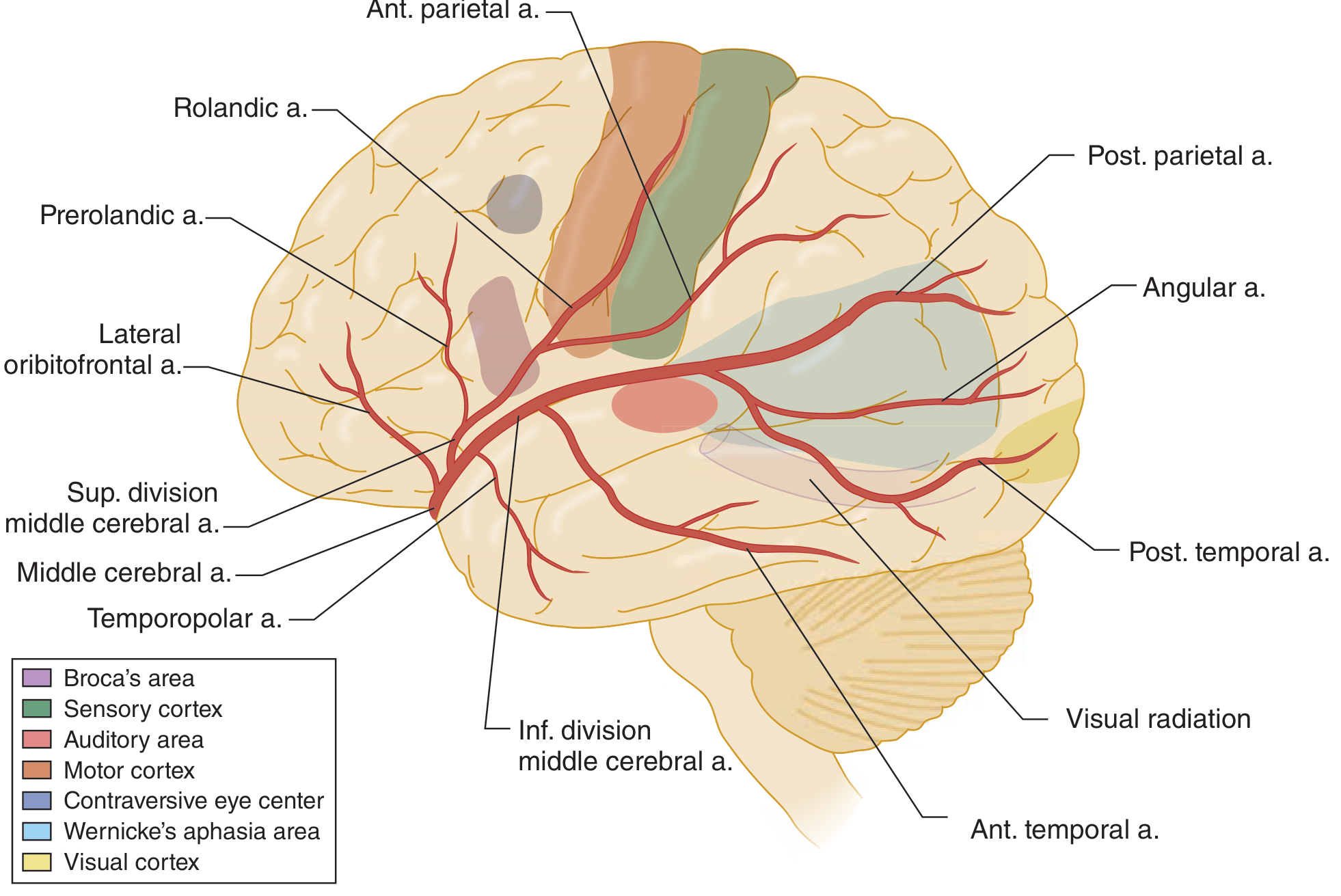
Figure 167-2. Cerebral Hemisphere, Medial Aspect - ACA and PCA distribution:
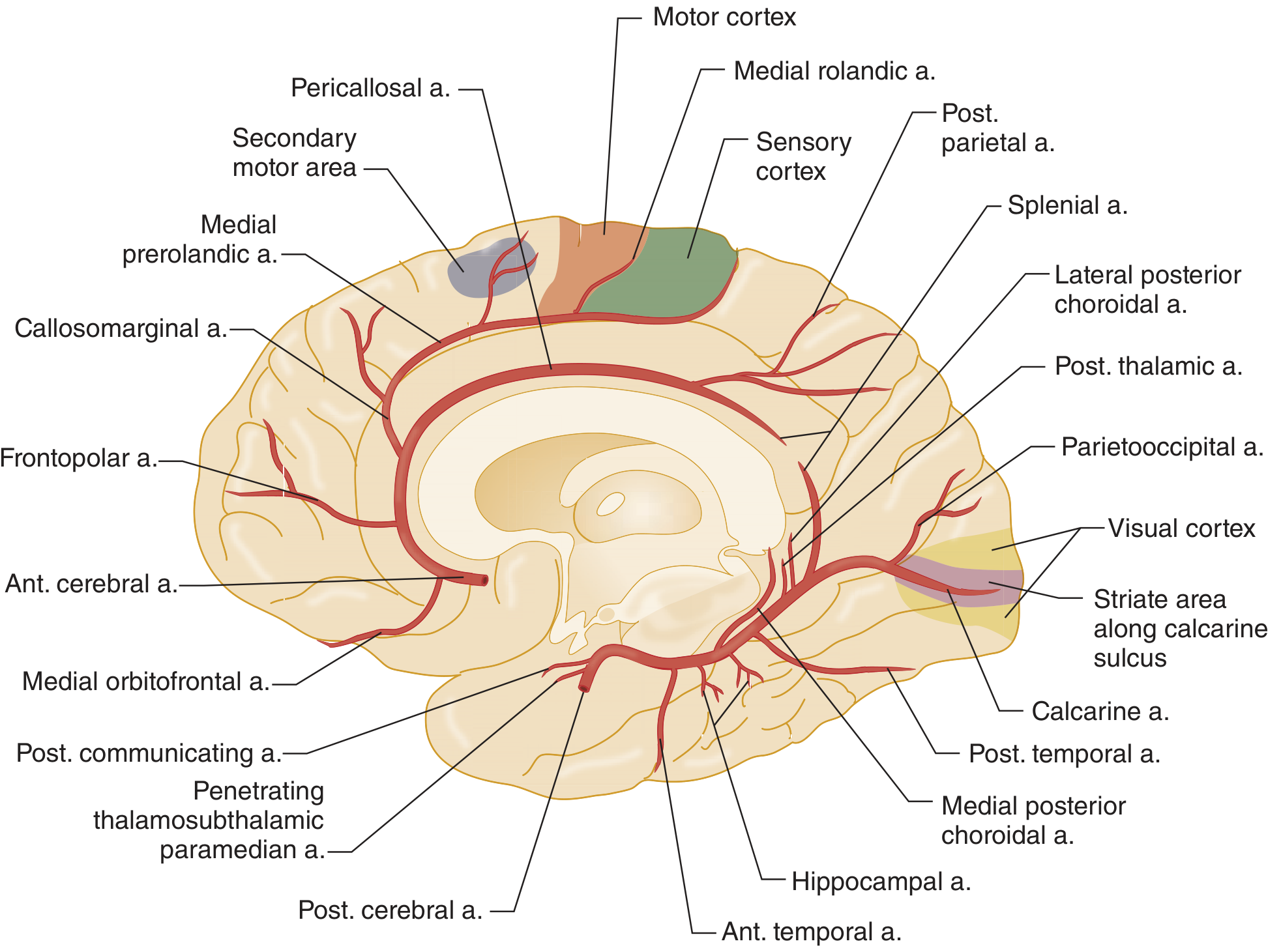
Table 1: Cerebrovascular Anatomy - Circulation, Arteries, and Brain Regions Supplied
| Circulation | Major Arteries | Major Regions Supplied |
|---|---|---|
| Anterior (Internal Carotid System) | Ophthalmic | Optic nerve and retina |
| Anterior Cerebral (ACA) | Frontal pole; Anteromedial cerebral cortex; Anterior corpus callosum | |
| Middle Cerebral (MCA) | Frontoparietal lobe; Anterotemporal lobe | |
| Posterior (Vertebral System) | Vertebral | Brainstem |
| PICA (Posteroinferior Cerebellar) | Cerebellum, lateral medulla | |
| Basilar | Thalamus, pons | |
| Posterior Cerebral (PCA) | Auditory/vestibular structures; Medial temporal lobe; Visual occipital cortex |
(Tintinalli's, Table 167-1)
3. Stroke Classification
Table 2: Stroke Classification
| Type | Subtype | Frequency | Key Mechanism |
|---|---|---|---|
| Ischemic | Thrombotic (large vessel) | ~33% of all strokes | Atherosclerotic plaque with clot at bifurcation |
| Thrombotic (lacunar/small vessel) | ~20% | Lipohyalinosis of small penetrating vessels; HTN/DM | |
| Cardioembolic | ~25% | Mural thrombus (AF is most common); artery-to-artery emboli | |
| Cryptogenic | >33% | No clear cause identified | |
| Hemorrhagic | Intracerebral hemorrhage (ICH) | 10% | Hypertensive vasculopathy; amyloid angiopathy |
| Subarachnoid hemorrhage (SAH) | 3% | Ruptured aneurysm/AVM |
(Tintinalli's Table 167-2; Rosen's Ch. 87)
4. ISCHEMIC STROKE SYNDROMES
Key principle (Rosen's): Anterior circulation strokes produce contralateral hemiparesis of face and body. Vertebrobasilar strokes produce ipsilateral cranial nerve deficits + contralateral hemiparesis ("crossed deficits").
4.1 Anterior Cerebral Artery (ACA) Infarction
Frequency: Uncommon - only 0.5% to 3% of all strokes
| Feature | Detail |
|---|---|
| Motor/Sensory | Contralateral lower extremity weakness > upper extremity; sparing of hands and face (leg >> arm) |
| Frontal lobe features | Altered mentation, impaired judgment and insight |
| Primitive reflexes | Grasp reflex, suck reflex present |
| Incontinence | Bowel and bladder incontinence |
| Language (left lesion) | Akinetic mutism, transcortical motor aphasia |
| Gait | Apraxia or clumsiness |
"Paralysis and hypoesthesia of the lower limb opposite the side of the lesion are characteristic. Leg weakness is more pronounced than arm weakness." - Rosen's Ch. 87
4.2 Middle Cerebral Artery (MCA) Infarction
Most commonly involved vessel in stroke. Clinical findings are highly variable depending on lesion location and hemisphere dominance (left hemisphere dominant in right-handed patients and ~80% of left-handers).
| Feature | Detail |
|---|---|
| Motor/Sensory | Contralateral hemiparesis + sensory loss; face and arm > leg |
| Hemianopsia | Contralateral homonymous hemianopsia |
| Gaze preference | Toward the side of the infarct (disruption of cortical lateral gaze center) |
| Dominant hemisphere (usually left) | Aphasia - expressive (Broca), receptive (Wernicke), or global |
| Non-dominant hemisphere (usually right) | Inattention, hemispatial neglect, extinction on double-simultaneous stimulation, dysarthria without aphasia, constructional apraxia |
Aphasia subtypes (MCA dominant hemisphere):
| Type | Area | Deficit |
|---|---|---|
| Broca's (Expressive) | Inferior frontal gyrus (Broca's area) | Cannot communicate verbally; understanding intact |
| Wernicke's (Receptive) | Posterior superior temporal gyrus | Cannot process/understand speech; fluent but meaningless speech |
| Global | Large MCA territory | Both expression and comprehension lost |
| Dysarthria | Motor deficit | Poor articulation but intact word choice; not cortical |
Aphasia localizes to the dominant cerebral cortex in MCA distribution. Dysarthria is a motor deficit. Dysphagia is difficulty swallowing - these three terms are commonly confused. - Rosen's Ch. 87
4.3 Posterior Cerebral Artery (PCA) Infarction - Distal Posterior Circulation
| Feature | Detail |
|---|---|
| Visual field | Contralateral homonymous hemianopsia (most specific sign); cortical blindness |
| Visual agnosia | Inability to recognize seen objects |
| Alexia without agraphia | Cannot read; can write (unique to PCA) |
| Color anomia | Inability to name colors |
| Memory | Recent memory loss (medial temporal involvement) |
| Oculomotor | Unilateral CN III palsy (ipsilateral) |
| Hemiballismus | Thalamic involvement |
| Motor | Typically minimal - patient may not realize stroke has occurred |
| Sensory | Light-touch and pinprick deficits |
"One of the more unique facets of this syndrome is that the patient may be unaware of any visual problem (visual neglect)." - Rosen's Ch. 87
PCA stroke: ipsilateral CN III palsy + contralateral homonymous hemianopsia - Rosen's Key Concepts
4.4 Basilar Artery Occlusion - Middle Posterior Circulation
| Feature | Detail |
|---|---|
| Presenting symptoms | Unilateral limb weakness, dizziness, dysarthria, diplopia, headache |
| Presenting signs | Unilateral limb weakness, CN VII signs, dysarthria, Babinski sign, oculomotor signs |
| Associated | Dysphagia, nausea/vomiting, Horner's syndrome |
| Locked-in syndrome | Bilateral pyramidal tract lesions in ventral pons - complete paralysis except upward gaze and blinking |
| Prognosis | High risk of death and poor outcomes |
4.5 Vertebrobasilar Infarction - Proximal Posterior Circulation
| Feature | Detail |
|---|---|
| Symptoms | Dizziness, nausea/vomiting, headache, dysphagia, unilateral limb weakness, CN V symptoms |
| Signs | Unilateral limb ataxia, nystagmus, gait ataxia, CN V signs, limb sensory deficit, Horner's syndrome |
4.6 Cerebellar Infarction
| Feature | Detail |
|---|---|
| Symptoms | Dizziness ± vertigo, nausea/vomiting, gait instability, headache, limb ataxia, dysarthria, dysmetria, nystagmus, hearing loss, intractable hiccups |
| Mental status | Alert to comatose |
| CT sensitivity | Up to 25% of noncontrasted head CTs can be normal - always get MRI-DWI if suspected |
| Danger | Rapid deterioration from cerebellar edema causing brainstem compression - watch for gaze palsy |
4.7 Wallenberg Syndrome (Lateral Medullary Syndrome)
Caused by occlusion of the posterior inferior cerebellar artery (PICA) or vertebral artery
| Feature | Side | Mechanism |
|---|---|---|
| Vertigo, nausea, vomiting, hiccups | - | Vestibular nucleus involvement |
| Horner syndrome (ptosis, miosis, anhidrosis) | Ipsilateral | Descending sympathetic tract |
| Facial numbness + loss of corneal reflex | Ipsilateral | CN V nucleus |
| Dysphagia + hoarseness | Ipsilateral | CN IX, X nucleus |
| Limb ataxia | Ipsilateral | Cerebellum/inferior cerebellar peduncle |
| Pain + temperature loss (body) | Contralateral | Spinothalamic tract |
| Motor | Spared | Corticospinal tract not involved (no hemiplegia) |
"Wallenberg syndrome causes vertigo, Horner syndrome, ipsilateral facial numbness, loss of corneal reflex, along with contralateral loss of pain and temperature." - Rosen's Key Concepts
4.8 Lacunar Infarction
- Infarction of small penetrating arteries (terminal small vessels)
- Strongly associated with chronic hypertension (80-90%) and diabetes
- Size: few mm to 2 cm
- Most common sites: basal ganglia, thalamus, pons, internal capsule
- Mechanism: lipohyalinosis (hypertensive vasculopathy) or small emboli
Classic Lacunar Syndromes:
| Syndrome | Location | Features |
|---|---|---|
| Pure motor hemiplegia | Internal capsule (posterior limb) or pons | Contralateral face, arm, leg weakness - NO sensory loss, NO cortical signs |
| Pure sensory stroke | Thalamus (VPL nucleus) | Contralateral hemisensory loss - NO motor |
| Sensorimotor stroke | Thalamocapsular junction | Combined motor + sensory without cortical features |
| Ataxic hemiparesis | Pons or internal capsule | Ipsilateral limb ataxia + contralateral hemiparesis |
| Dysarthria-clumsy hand | Pons or genu of internal capsule | Dysarthria + contralateral hand clumsiness |
Prognosis generally more favorable than other stroke syndromes. - Tintinalli's Ch. 167
4.9 Stroke in Young Adults (15-45 years old)
- 3-4% of all strokes occur in this age group
- Average age of first stroke is becoming younger
| Cause | Notes |
|---|---|
| Cervical artery dissection | Most common determined cause in young adults |
| Oral contraceptives / pregnancy | Hypercoagulable state |
| Antiphospholipid antibodies | Lupus anticoagulant, anticardiolipin Ab |
| Protein S/C deficiency | Thrombophilia |
| Sickle cell anemia | Sludging/thrombosis |
| Cocaine, amphetamines | Vasoconstrictors - both ischemic and hemorrhagic |
| Migraine (rare) | Prolonged vasoconstriction |
| Fibromuscular dysplasia | Cerebrovascular |
| Infectious vasculopathy | Varicella, fungal meningitis |
4.10 Carotid & Vertebral Artery Dissection
- Accounts for 2% of all strokes and up to 25% of strokes in young adults
- Trauma (even minor: chiropractic manipulation, sneezing, sport) in ~40% of cases
Carotid Artery Dissection:
- Headache: frontotemporal region; may mimic SAH ("thunderclap")
- Partial Horner's syndrome (miosis + ptosis) in ~25%
- Cranial nerve palsies in ~12%
- Leads to anterior circulation symptoms
Vertebral Artery Dissection:
- Dizziness/vertigo (58%), headache (51-65%), neck pain (46-66%)
- Headache typically occipital
- Symptoms: facial paresthesia, ataxia, limb weakness, dysarthria, hearing loss
- Leads to posterior circulation symptoms / Wallenberg syndrome
TIAs preceding stroke in dissection patients are often misdiagnosed. - Rosen's Key Concepts
5. HEMORRHAGIC STROKE SYNDROMES
5.1 Intracerebral Hemorrhage (ICH)
- 10-15% of all acute strokes; ~65,000 patients/year
- 30-day mortality: up to 50% (half die in first 2 days)
- Only 1 in 5 survivors are living independently at 6 months
Two major causes:
- Hypertensive vasculopathy - lipohyalinosis of deep penetrating arteries; deep locations
- Cerebral amyloid angiopathy - amyloid deposition in vessel walls; lobar, in elderly
Table 3: Common Sites of Hypertensive ICH (Box 87.1 - Rosen's)
| Location | Frequency | Typical Presentation |
|---|---|---|
| Putamen | 44% | Contralateral motor/sensory deficit |
| Other cortical areas | 25% | Variable |
| Thalamus | 13% | Limb pain, speech difficulty |
| Cerebellum | 9% | Uncoordinated movements of trunk and limbs |
| Pons | 9% | Numbness, weakness, ataxia, dizziness |
Spontaneous ICH may be clinically indistinguishable from ischemic infarction. CT is mandatory to differentiate. - Tintinalli's Ch. 167
Distinguishing ICH clinically: Headache, nausea, and vomiting often precede the neurologic deficit, and the condition may rapidly deteriorate.
5.2 Subarachnoid Hemorrhage (SAH)
- Characterized by sudden severe occipital or nuchal headache
- "Thunderclap" headache - worst headache of life, maximal at onset
- Associated with Valsalva activities (defecation, sex, weight lifting, coughing)
- Preretinal hemorrhage on fundoscopy is a hallmark finding
6. Stroke Mimics
Table 4: Stroke Mimics and Distinguishing Features (Tintinalli's Table 167-5)
| Mimic | Distinguishing Features |
|---|---|
| Todd's paralysis (post-ictal) | Transient paralysis after seizure; disappears quickly |
| Syncope | No persistent neurologic symptoms |
| Meningitis/Encephalitis | Fever; detected on lumbar puncture |
| Complicated migraine | History of similar episodes, preceding aura |
| Brain tumor/Abscess | Focal findings; detectable by imaging |
| Epidural/Subdural hematoma | History of trauma, anticoagulant use |
| Hypoglycemia | Bedside glucose corrects deficits |
| Hyponatremia | Diuretic use, excess free water intake |
| Hypertensive encephalopathy | Global dysfunction; gradual onset; cerebral edema |
| Wernicke's encephalopathy | Alcoholism/malnutrition; ataxia + ophthalmoplegia + confusion |
| Labyrinthitis | Purely vestibular symptoms; no other focal findings |
| Bell's palsy | Isolated peripheral CN VII (forehead involved) |
| Meniere's disease | Recurrent episodes; tinnitus; deafness |
| Multiple sclerosis | Gradual onset; multifocal history |
| Conversion disorder | No CN findings; non-anatomic distribution; inconsistent exam |
| Drug toxicity (phenytoin, carbamazepine) | Ataxia, vertigo, elevated blood levels |
7. Clinical Features - Examination Approach
Anterior vs. Posterior Circulation Strokes
| Feature | Anterior Circulation | Posterior Circulation |
|---|---|---|
| Consciousness | Usually preserved (unless bilateral or prior stroke) | Can have loss of consciousness |
| Nausea/Vomiting | Uncommon | Common (CTZ in brainstem) |
| Cranial nerve deficits | Rare (CN VII central only) | Common (CN III-XII) |
| Laterality of deficits | Same side of body | Crossed (ipsilateral CN + contralateral motor/sensory) |
| Visual symptoms | Monocular visual loss (ophthalmic a.) | Bilateral field defects, diplopia, nystagmus |
| Progression | Progresses in first 24 hrs | May progress up to 3 days |
| NIHSS weighting | Weighted toward detection | Under-detected (CN deficits score fewer points) |
(Tintinalli's Ch. 167; Rosen's Ch. 87)
Key Physical Examination Points (Rosen's)
- Gaze preference - suggests cortical or brainstem involvement (toward the lesion in cortical strokes)
- Central vs. peripheral CN VII weakness - peripheral lesion: cannot wrinkle forehead; central: forehead spared
- Pronator drift - sensitive sign of contralateral motor weakness
- Double simultaneous extinction - tests sensory neglect; patient feels each side alone but not both together
- Graphesthesia - number scratched on forearm; tests parietal lobe cortical sensation
- Gait testing - critical but commonly omitted; detects subtle ataxia and focal cerebellar lesions
8. Anterior vs. Posterior Circulation: Summary Comparison
Table 5: Clinical Features by Vascular Territory
| Artery | Territory | Classic Deficits | Key Distinguishing Feature |
|---|---|---|---|
| ACA | Frontal/medial | Contralateral leg > arm weakness; frontal signs; incontinence | Leg weakness > arm |
| MCA | Lateral cortex | Contralateral face + arm > leg; aphasia (dominant); neglect (non-dominant) | Face + arm > leg; aphasia vs. neglect |
| PCA | Occipital/temporal | Contralateral homonymous hemianopsia; CN III palsy; visual agnosia; alexia | Visual field loss; minimal motor |
| Basilar | Pons/midbrain | Bilateral long tract signs; CN deficits; coma; locked-in syndrome | Bilateral + CN + LOC |
| PICA/Vertebral (Wallenberg) | Lateral medulla | Ipsilateral: Horner, facial numbness, ataxia; Contralateral: pain/temp loss; No hemiplegia | CROSSED deficits; NO hemiplegia |
| Lacunar | Deep (BG, thalamus, capsule, pons) | Pure motor or pure sensory; no cortical signs | Pure deficits; no cortical features |
| Cerebellar | Cerebellum | Ataxia, dysmetria, nystagmus, vertigo; CT often normal | CT unreliable - use MRI-DWI |
9. Stroke Progression Patterns
| Pattern | Timing | Mechanism |
|---|---|---|
| Stroke in evolution | Minutes to hours | ~20% anterior; ~40% posterior circulation strokes progress |
| Anterior progression | Up to 24 hours | Thrombus propagation |
| Posterior progression | Up to 3 days | Thrombus propagation in vertebrobasilar system |
| Complete stroke | Deficit maximal at onset | Embolic typically |
| TIA | Complete resolution; no infarction on DWI | Transient ischemia without tissue infarction |
10. Stroke Diagnostic Flowchart
SUSPECTED STROKE
│
▼
ABC + Vital Signs + Bedside glucose
(Treat hypoglycemia immediately)
│
▼
Activate Stroke Team (immediately upon arrival)
│
▼
Focused History: Last known well time, symptom onset,
medications (anticoagulants), recent procedures/trauma
│
▼
Neurological Exam: NIHSS score
│
├─── Posterior signs (CN deficits, ataxia,
│ crossed findings, vertigo, diplopia)?
│ └── Consider vertebrobasilar syndrome
│ → MRI-DWI preferred over CT
│
▼
Non-contrast CT Head (within 20 min of arrival)
│
├── Hemorrhage on CT?
│ YES → Hemorrhagic Stroke
│ ├── ICH: BP control, reverse anticoagulation
│ │ (PCC > FFP for warfarin; Vit K)
│ └── SAH: Neurosurgical consult
│
└── No hemorrhage on CT?
│
▼
Ischemic Stroke
│
▼
Within 4.5 hours of symptom onset?
AND eligible for tPA?
│
YES │ NO
│ └── General supportive care
│ Antiplatelet therapy
│ BP permissive unless >220/120
▼
IV Alteplase (tPA)
0.9 mg/kg (max 10 mg IV bolus + 90% over 60 min)
Door-to-needle: ≤60 min (target ≤45 min)
│
▼
Emergent Large Vessel Occlusion (LVO)?
CT Angiography
│
▼
Mechanical Thrombectomy (if LVO confirmed)
Up to 24 hrs in selected patients (DAWN/DEFUSE3)
│
▼
Admit to Stroke Unit / ICU
(Tintinalli's Table 167-8; Rosen's Ch. 87)
11. Key Time Targets (AHA/ASA - Tintinalli's Table 167-8)
| Intervention | Time Goal from ED Arrival |
|---|---|
| Activation of stroke team | Immediately upon arrival |
| Start of brain imaging | ≤ 20 minutes |
| Administration of IV thrombolytics | ≤ 60 minutes (secondary goal ≤ 45 minutes) |
12. NIHSS - National Institutes of Health Stroke Scale
- Score range: 0-42 (0 = normal; higher = more severe)
- Rapid (5-10 minutes); high interrater reliability
- Important caveat: Weighted toward anterior circulation strokes - posterior strokes (CN deficits, ataxia) receive fewer points; ataxia scored as absent if weakness is present
- Also has a bias toward detecting left hemisphere strokes
13. Prognosis & Complications
Factors worsening acute stroke prognosis (Rosen's):
- Fever
- Hypotension
- Hypoxia
- Hypoglycemia or Hyperglycemia
ICH-specific risks (Rosen's):
- IV tPA: symptomatic intracranial hemorrhage in 2-7%; asymptomatic hemorrhage in 30-45% (>10 cerebral microbleeds)
- Risk lowest with: low NIHSS, no hypertension, no diabetes, age < 70 years
Quick Reference: Wallenberg Syndrome Summary
| Side | Finding |
|---|---|
| Ipsilateral | Horner's syndrome (ptosis, miosis, anhidrosis) |
| Ipsilateral | Facial numbness + loss of corneal reflex (CN V nucleus) |
| Ipsilateral | Dysphagia + hoarseness (CN IX, X) |
| Ipsilateral | Limb ataxia (cerebellar peduncle) |
| Contralateral | Loss of pain and temperature on body (spinothalamic tract) |
| Both | Vertigo, nausea, vomiting, hiccups |
| Absent | Hemiplegia (corticospinal tract spared) |
Key Concepts Summary (Rosen's Chapter 87)
- Anterior circulation strokes → contralateral hemiparesis of face and body
- Vertebrobasilar strokes → ipsilateral CN deficits + contralateral hemiparesis (crossed deficits)
- PCA stroke → ipsilateral CN III palsy + contralateral homonymous hemianopsia
- Wallenberg syndrome → vertigo + Horner's + ipsilateral facial numbness + corneal reflex loss + contralateral pain/temperature loss
- Cervical artery dissection is the leading determined cause of stroke in young patients; TIAs often misdiagnosed
- IV tPA dose: 0.9 mg/kg (10% bolus + 90% over 1 hour); window = 4.5 hours
- Avoid overly aggressive BP management in acute ischemic stroke
- ICH reversal: prefer PCC over FFP (faster INR correction, lower infection risk, lower volume)
- Fever, hypotension, hypoxia, and glucose abnormalities worsen prognosis
References: Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th Edition, Chapter 167 (Steven Go). Rosen's Emergency Medicine: Concepts and Clinical Practice, 10th Edition, Chapter 87 (Linda Papa & William J. Meurer).
Explain full chapter Stroke syndromes in Great detail including images, tables, flowchart, management, trials References - Tintinalli's 9th edition & Rosen's 10th edition
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
STROKE SYNDROMES
Complete Chapter Review
References: Tintinalli's Emergency Medicine, 9th Ed. (Chapter 167 - Steven Go) | Rosen's Emergency Medicine, 10th Ed. (Chapter 87 - Linda Papa & William J. Meurer)
SECTION 1: EPIDEMIOLOGY
- 795,000 strokes/year in the United States - one stroke every 40 seconds; one death every 4 minutes
- 77% are first-ever strokes; 23% recurrent events
- Estimated cost: $33.9 billion in total expenditures (2012-2013)
- Age-adjusted stroke death rate fell 28.7% from 2004-2014 due to stroke units, thrombolysis, and endovascular thrombectomy
- About 240,000 TIAs/year in the United States
Stroke Type Distribution:
- Ischemic: 87% of all strokes
- ICH: 10%
- SAH: 3%
(Tintinalli's Ch. 167)
SECTION 2: PATHOPHYSIOLOGY & ANATOMY
Stroke = any disease process that interrupts blood flow to the brain. Injury is from:
- Loss of oxygen and glucose - failure of high-energy phosphate production
- Mediators of secondary cellular injury - glutamate excitotoxicity, free radicals
- Edema and mass effect - exacerbate initial insult
Neurons die within minutes of complete cessation of perfusion - this is why rapid reperfusion is the treatment cornerstone.
The Ischemic Penumbra
The area of irreversible infarct (core) is surrounded by ischemic tissue (penumbra) that may be salvageable. CT perfusion and DWI-MRI/FLAIR are used to measure the penumbra, especially for patients outside standard time windows.
Vascular Anatomy
Fig. 167-1: Cerebral Hemisphere, Lateral Aspect - MCA Distribution
Fig. 167-2: Cerebral Hemisphere, Medial Aspect - ACA and PCA Distribution
Table 1: Cerebrovascular Anatomy - Circulation, Arteries & Brain Regions
| Circulation | Major Artery | Brain Regions Supplied |
|---|---|---|
| Anterior (Internal Carotid System) | Ophthalmic | Optic nerve, retina |
| Anterior Cerebral (ACA) | Frontal pole; Anteromedial cortex; Anterior corpus callosum | |
| Middle Cerebral (MCA) | Frontoparietal lobe; Anterotemporal lobe; Deep white matter via lenticulostriate branches | |
| Posterior (Vertebral-Basilar System) | Vertebral | Lateral medulla, cerebellum |
| PICA | Dorsolateral medulla, inferior cerebellum | |
| Basilar | Pons, midbrain, superior cerebellum | |
| Posterior Cerebral (PCA) | Thalamus; Medial temporal lobe; Occipital lobe; Visual cortex |
(Tintinalli's Table 167-1)
SECTION 3: STROKE CLASSIFICATION
Table 2: Complete Stroke Classification (Tintinalli's Table 167-2)
| Type | Mechanism | Major Causes | Clinical Notes |
|---|---|---|---|
| Thrombotic | Narrowing/clot at damaged arterial lumen | Atherosclerosis; Vasculitis; Arterial dissection; Polycythemia; Hypercoagulable states; Infections (HIV, syphilis, TB, aspergillosis) | Gradual onset; wax and wane; common cause of TIA |
| Embolic | Normal lumen obstructed by remote material | Valvular vegetations; Mural thrombi (AF); Paradoxical emboli; Cardiac tumors (myxoma); Artery-to-artery; Fat emboli; IV drug use; Septic emboli | Typically sudden onset; 20% of ischemic strokes |
| Hypoperfusion | Low-flow state, watershed hypoperfusion | Cardiac failure with systemic hypotension | Watershed/border-zone pattern; wax and wane with hemodynamics |
| ICH | Intraparenchymal bleed from weakened arterioles | HTN; Amyloid angiopathy; AVM; Cocaine; Anticoagulants; Tumor; Venous sinus thrombosis | 10% of all strokes; highest morbidity/mortality |
| SAH | Subarachnoid space bleeding | Ruptured saccular aneurysm; Trauma; AVM | 3% of all strokes; thunderclap headache |
SECTION 4: CLINICAL FEATURES
History - Key Distinguishing Features
| Presentation | Suggested Type |
|---|---|
| Sudden onset at maximal severity | Embolic or hemorrhagic |
| Stuttering or waxing and waning deficit | Thrombotic or hypoperfusion |
| Thunderclap headache + Valsalva activity | Ruptured aneurysm / SAH |
| Recent neck trauma or manipulation | Cervical artery dissection |
| AF, valvular replacement, recent MI | Cardioembolic |
| Same vascular distribution TIA | Thrombotic vascular disease |
| TIAs in different distributions | Embolic source |
| Hypertension + diabetes onset | Lacunar or ICH |
Table 3: Stroke Symptoms - Traditional vs. Non-Traditional (Tintinalli's Table 167-4)
| Traditional Symptoms | Non-Traditional Symptoms |
|---|---|
| Sudden numbness or weakness (face, arm, leg) - usually unilateral | Impaired consciousness or syncope |
| Sudden aphasia | Generalized weakness |
| Sudden dysarthria | Altered mental status |
| Sudden memory deficit / spatial disorientation | Dysphagia |
| Sudden visual deficit or diplopia | Shortness of breath |
| Sudden dizziness, gait disturbance, ataxia | Sudden pain in face, chest, arms, legs |
| Sudden severe headache with no known cause | Seizure; Falls; Sudden hiccups; Nausea; Fatigue; Palpitations |
Women tend to report more severe but diffuse nontraditional symptoms compared to men. - Tintinalli's Ch. 167
SECTION 5: ISCHEMIC STROKE SYNDROMES
Fundamental rule: Anterior circulation = contralateral hemiparesis face + body. Vertebrobasilar = ipsilateral CN deficits + contralateral motor/sensory (crossed deficits).
5.1 Anterior Cerebral Artery (ACA) Infarction
Frequency: 0.5%-3% of all strokes
| Feature | Detail |
|---|---|
| Motor/Sensory | Contralateral leg > arm; sparing of face and hand |
| Frontal lobe features | Altered mentation, impaired judgment and insight |
| Primitive reflexes | Grasp reflex, suck reflex |
| Incontinence | Bowel and bladder |
| Language (left lesion) | Akinetic mutism; transcortical motor aphasia |
| Gait | Apraxia; clumsiness |
5.2 Middle Cerebral Artery (MCA) Infarction
Most commonly involved vessel in stroke. Dominance: left hemisphere in right-handers and ~80% of left-handers.
| Feature | Detail |
|---|---|
| Motor/Sensory | Contralateral hemiparesis + hemisensory loss; face + arm > leg |
| Visual | Contralateral homonymous hemianopsia |
| Gaze preference | Toward the side of infarct (disruption of cortical lateral gaze center) |
| Dominant hemisphere (left) | Aphasia - Broca, Wernicke, or global |
| Non-dominant hemisphere (right) | Inattention; hemispatial neglect; extinction on double simultaneous stimulation; constructional apraxia |
Aphasia in Detail (MCA / Dominant Hemisphere):
| Type | Location | Production | Comprehension | Repetition |
|---|---|---|---|---|
| Broca's (expressive) | Inferior frontal gyrus | Non-fluent; effortful | Relatively intact | Impaired |
| Wernicke's (receptive) | Posterior superior temporal | Fluent but meaningless | Severely impaired | Impaired |
| Global | Large MCA territory | Non-fluent | Severely impaired | Impaired |
| Dysarthria (not cortical) | Motor mouth/tongue | Poor articulation; intact word choice | Normal | Intact |
Aphasia localizes to the dominant cerebral cortex in MCA distribution. Dysarthria is a purely motor speech deficit. Dysphagia is difficulty swallowing - all three are frequently confused. - Rosen's Ch. 87
5.3 Posterior Cerebral Artery (PCA) Infarction
(Distal Posterior Circulation)
| Feature | Detail |
|---|---|
| Visual field | Contralateral homonymous hemianopsia (most specific sign); cortical blindness |
| Visual agnosia | Inability to recognize seen objects |
| Alexia without agraphia | Cannot read; CAN write (unique PCA finding) |
| Color anomia | Inability to name colors |
| Memory | Recent memory loss (medial temporal involvement) |
| Oculomotor | Ipsilateral CN III palsy |
| Hemiballismus | Thalamic involvement |
| Motor | Minimal - patient may not realize a stroke has occurred |
| Neglect | Patient may be unaware of visual problem (visual neglect) |
PCA stroke: ipsilateral CN III palsy + contralateral homonymous hemianopsia. - Rosen's Key Concepts
5.4 Basilar Artery Occlusion
(Middle Posterior Circulation)
| Feature | Detail |
|---|---|
| Presenting symptoms | Unilateral limb weakness, dizziness, dysarthria, diplopia, headache |
| Presenting signs | CN VII signs, Babinski sign, oculomotor signs, dysarthria |
| Associated | Dysphagia, nausea/vomiting, Horner's syndrome |
| Rare - Locked-in Syndrome | Bilateral pyramidal tract lesions in ventral pons; complete paralysis except upward gaze + blinking |
| Prognosis | High mortality; among the worst prognosis of any stroke |
5.5 Vertebrobasilar Infarction
(Proximal Posterior Circulation)
| Feature | Detail |
|---|---|
| Symptoms | Dizziness, nausea/vomiting, headache, dysphagia, unilateral limb weakness, CN V symptoms |
| Signs | Unilateral limb ataxia, nystagmus, gait ataxia, Horner's syndrome, CN V signs, limb sensory deficit |
5.6 Wallenberg Syndrome (Lateral Medullary Syndrome)
Vessel: PICA occlusion or vertebral artery occlusion. Classic example of crossed deficit.
| Side | Finding | Tract/Structure |
|---|---|---|
| Ipsilateral | Horner's syndrome (ptosis + miosis + anhidrosis) | Descending hypothalamo-spinal sympathetic tract |
| Ipsilateral | Facial numbness + loss of corneal reflex | Nucleus + spinal tract of CN V |
| Ipsilateral | Dysphagia + hoarseness | Nucleus ambiguus (CN IX, X) |
| Ipsilateral | Limb ataxia | Inferior cerebellar peduncle / cerebellum |
| Contralateral | Loss of pain + temperature on body | Spinothalamic tract |
| Bilateral | Vertigo, nausea, vomiting, hiccups | Vestibular nuclei; CTZ in brainstem |
| Absent | Hemiplegia | Corticospinal tract is SPARED |
"Wallenberg syndrome causes vertigo, Horner syndrome, ipsilateral facial numbness, loss of corneal reflex, along with contralateral loss of pain and temperature." - Rosen's Key Concepts
5.7 Cerebellar Infarction
| Feature | Detail |
|---|---|
| Symptoms | Dizziness ± vertigo, nausea/vomiting, gait instability, headache, limb ataxia, dysarthria, dysmetria, nystagmus, hearing loss, intractable hiccups |
| Mental status | Alert to comatose |
| CT caveat | Up to 25% of noncontrasted CTs are normal - always get MRI-DWI if suspected |
| Danger | Cerebellar edema → brainstem compression → rapid deterioration; watch for gaze palsy |
5.8 Lacunar Infarction
Mechanism: Infarction of small penetrating arteries (terminal vessels 80-900 µm). Associated with chronic hypertension (80-90% of patients) and diabetes. Lipohyalinosis is the primary process. Size: few mm to 2 cm.
Common locations: Basal ganglia, thalamus, pons, internal capsule.
Classic Lacunar Syndromes:
| Syndrome | Location | Key Features |
|---|---|---|
| Pure Motor Hemiplegia | Posterior limb internal capsule or pons | Contralateral face + arm + leg weakness; NO sensory loss, NO cortical signs |
| Pure Sensory Stroke | Thalamus (VPL) | Contralateral hemisensory loss only |
| Sensorimotor Stroke | Thalamocapsular junction | Motor + sensory, no cortical features |
| Ataxic Hemiparesis | Pons or internal capsule | Ipsilateral limb ataxia + contralateral hemiparesis |
| Dysarthria-Clumsy Hand | Pons or genu of internal capsule | Dysarthria + contralateral hand clumsiness |
Prognosis generally more favorable than other stroke syndromes. - Tintinalli's Ch. 167
5.9 Stroke in Young Adults (15-45 years)
- 3%-4% of all strokes; average age of first stroke getting younger
- Must search for less common, often reversible, causes
| Cause | Notes |
|---|---|
| Cervical artery dissection | Leading determined cause in young adults; 20% of strokes in this group |
| Oral contraceptives / Pregnancy | Hypercoagulable / prothrombotic state |
| Antiphospholipid antibodies | Lupus anticoagulant, anticardiolipin antibodies |
| Protein S or C deficiency | Hereditary thrombophilia |
| Sickle cell disease, polycythemia | Sludging and thrombosis |
| Mitral valve prolapse, RHD | Cardioembolic - young adults |
| Cocaine, amphetamines, heroin | Vasoconstrictors; both ischemic + hemorrhagic |
| Migrainous stroke | Infarction during typical migraine |
| HIV (CD4 <200) | Rate ratio 2.5 for ischemic stroke |
| Fibromuscular dysplasia | Cerebrovascular dysplasia |
| Cancer history | Hypercoagulable; direct invasion |
5.10 Carotid and Vertebral Artery Dissection
- 2% of all strokes; up to 20-25% of strokes in young adults
- Neck trauma in ~40% (often minor: chiropractic manipulation, sneezing, sports)
- First symptom: unilateral headache (68%), neck pain (39%), face pain (10%)
- Median delay from neck pain to neurologic symptoms: 4 days; from headache: 15 hours
Carotid Artery Dissection:
- Frontotemporal headache; may mimic SAH (thunderclap quality)
- Partial Horner's syndrome (miosis + ptosis) in ~25%; rarely, full Horner's
- Cranial nerve palsies in ~12%
- Anterior circulation symptoms; can lead to retinal infarction
Vertebral Artery Dissection:
- Occipital headache (51-65%); neck pain (46-66%); dizziness/vertigo (58%)
- Posterior circulation symptoms: facial paresthesia, ataxia, limb weakness, hearing loss
- May cause Wallenberg syndrome
Diagnosis: CT/CTA or MRI/MRA have similar performance; choice by availability/stability.
TIAs preceding stroke in cervical dissection are often misdiagnosed. - Rosen's Key Concepts
SECTION 6: HEMORRHAGIC STROKE SYNDROMES
6.1 Intracerebral Hemorrhage (ICH)
- 10%-15% of all strokes; ~65,000 patients/year
- 30-day mortality: up to 50%; half die in first 2 days
- Only 1 in 5 survivors are living independently at 6 months
- ~40% show significant hemorrhage expansion in the first few hours
Two primary causes:
- Hypertensive vasculopathy - lipohyalinosis of deep penetrating vessels; deep ICH
- Cerebral amyloid angiopathy - amyloid in vessel walls; lobar ICH; elderly patients
Table 4: Sites of Hypertensive ICH and Presentations (Rosen's Box 87.1)
| Location | Frequency | Typical Presentation |
|---|---|---|
| Putamen | 44% | Contralateral motor + sensory deficit |
| Other cortical areas | 25% | Variable (lobar) |
| Thalamus | 13% | Limb pain, speech difficulty |
| Cerebellum | 9% | Uncoordinated movements of trunk and limbs |
| Pons | 9% | Numbness, weakness, ataxia, dizziness |
ICH may be clinically indistinguishable from ischemic stroke. CT is mandatory to differentiate the two. - Tintinalli's Ch. 167
Clinical features suggesting ICH: Headache, nausea, and vomiting preceding the neurologic deficit; rapid deterioration.
ICH Score (Prognostic Tool) - Rosen's Table 87.3
| Component | Score |
|---|---|
| GCS 3-4 | +2 |
| GCS 5-12 | +1 |
| GCS 13-15 | 0 |
| ICH volume ≥30 mL | +1 |
| Infratentorial origin | +1 |
| Age ≥80 years | +1 |
| Intraventricular hemorrhage | +1 |
Higher score = higher 30-day mortality.
6.2 Subarachnoid Hemorrhage (SAH)
- Thunderclap headache: "worst headache of my life," maximal at onset
- Often associated with Valsalva activities: defecation, sexual activity, weight lifting, coughing
- Severe occipital or nuchal headache that is sudden
- Preretinal (subhyaloid) hemorrhage on fundoscopy is pathognomonic
- Meningismus may develop within hours
SECTION 7: STROKE MIMICS
Table 5: Stroke Mimics and Distinguishing Features (Tintinalli's Table 167-5)
| Mimic | Key Distinguishing Features |
|---|---|
| Todd's paralysis (post-ictal) | Transient paralysis after seizure; disappears quickly; seizure may be caused by CVA |
| Syncope | No persistent neurologic symptoms |
| Meningitis/Encephalitis | Fever; CSF changes on LP |
| Complicated migraine | History of similar episodes; preceding aura; headache |
| Brain tumor/Abscess | Focal neurologic findings; detectable by imaging; fever for abscess |
| Epidural/Subdural hematoma | Trauma history; anticoagulant use; bleeding disorder |
| SAH | Thunderclap headache (note: SAH is itself a hemorrhagic stroke) |
| Hypoglycemia | Bedside glucose; diabetes history; corrects with dextrose |
| Hyponatremia | Diuretic use; excessive free water; labs |
| Hypertensive encephalopathy | Gradual onset; global dysfunction; cerebral edema; improves with BP control |
| Hyperosmolar coma | Extremely high glucose; diabetes history |
| Wernicke's encephalopathy | Alcoholism/malnutrition; classic triad: ataxia + ophthalmoplegia + confusion |
| Labyrinthitis | Purely vestibular symptoms; no other focal findings |
| Bell's palsy | Isolated peripheral CN VII (forehead INVOLVED - cannot wrinkle) |
| Meniere's disease | Recurrent episodes; tinnitus; progressive deafness |
| Multiple sclerosis | Gradual onset; multifocal history; young patient |
| Conversion disorder | No CN findings; non-anatomic distribution; inconsistent exam |
| Drug toxicity (phenytoin, carbamazepine, lithium) | Toxidromes; elevated drug levels; ataxia/vertigo |
| CVST | Headache, seizures, papilledema; venous phase on CTA or MRV |
SECTION 8: PREHOSPITAL STROKE SCALES
Table 6: Prehospital Stroke Scales (Tintinalli's Table 167-3)
| Scale | Components | Positive if... |
|---|---|---|
| Cincinnati Prehospital Stroke Scale (CPSS) | Facial droop; Arm drift; Speech abnormality | Any 1 of 3 present: sensitivity 59%, specificity 89% |
| Los Angeles Prehospital Stroke Screen (LAPSS) | Age >45; No prior seizure; Not wheelchair-bound; BG 50-400; Asymmetric face/grip/arm strength | All screening items + 1 neurologic finding |
| Melbourne Ambulance Stroke Screen (MASS) | Age ≥45; No seizure; Not bedridden; BG 50-400; + facial droop/grip weakness/arm drift/abnormal speech | All 4 criteria + any 1 neurologic sign: sensitivity 90% |
SECTION 9: NIHSS - National Institutes of Health Stroke Scale
- Score range: 0-42 (0 = normal; higher = more severe)
- Duration: 5-10 minutes; high interrater reliability
- 15-item, 11-category neurologic evaluation
- Caveat 1: Weighted toward anterior circulation strokes - posterior strokes (CN deficits, ataxia) get fewer points; ataxia scored absent if weakness present
- Caveat 2: Bias toward detecting left hemisphere strokes
| NIHSS Score Range | Stroke Severity |
|---|---|
| 0 | Normal |
| 1-4 | Minor |
| 5-15 | Moderate |
| 16-20 | Moderate-severe |
| 21-42 | Severe |
SECTION 10: DIAGNOSTIC EVALUATION
Neuroimaging
Non-contrast CT (NCCT) Head:
- First-line imaging; must be done within 20 minutes of ED arrival
- Differentiates ischemic stroke from ICH and mass lesions
- Ischemic stroke: gross changes NOT seen for 6-12 hours
- Subtle early ischemic changes seen in up to 67% within first 3 hours:
- Hyperdense artery sign (acute thrombus in vessel)
- Sulcal effacement
- Loss of insular ribbon
- Loss of gray-white interface
- Mass effect; acute hypodensity
CT Angiography (CTA):
- High-quality images of large vessels; detects LVO (large vessel occlusion)
- Identifies secondary causes of ICH: aneurysm, AVM, fistula
- Spot sign on CTA = contrast extravasation in ICH → high risk of hemorrhage expansion
MRI:
- DWI (Diffusion-Weighted Imaging): Detects ischemia within minutes of onset
- FLAIR: Detects parenchymal edema; typically becomes positive 4-6 hours after onset
- DWI-FLAIR mismatch = ischemia on DWI but FLAIR negative = suggests stroke onset within 4.5 hours (useful for wake-up strokes)
DWI and FLAIR Images - Wake-Up Stroke Identification (Rosen's Fig. 87.5):
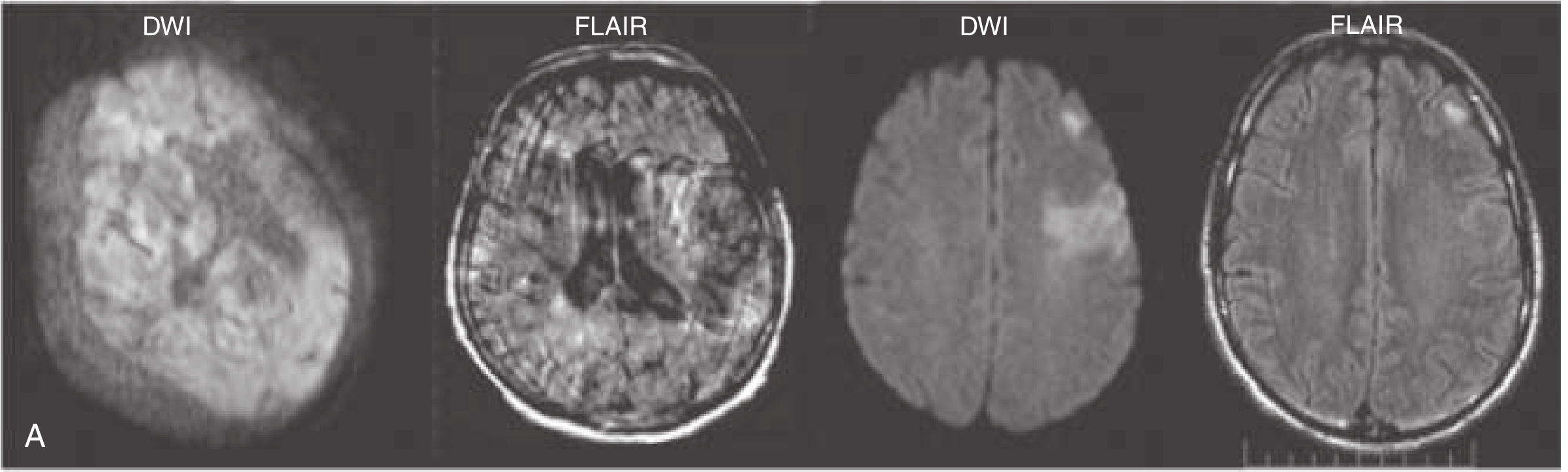
FLAIR-negative (DWI-FLAIR mismatch) = lesion on DWI but not FLAIR = stroke likely within 4.5 hours; FLAIR-positive = lesion on both = stroke likely older than 4.5 hours
MRI sensitivity: Detects posterior fossa strokes that CT misses; essential for suspected cerebellar infarction.
ASPECTS Score (Alberta Stroke Program Early CT Score)
- 10-point scale assessing early ischemic changes in MCA territory on NCCT
- Score ≥6 = relatively preserved brain tissue = favorable for intervention
- Score <6 = extensive early ischemic changes = less benefit from thrombectomy
Laboratory Studies
Required before thrombolytics: bedside glucose only (do not delay tPA for other labs unless anticoagulant use suspected or thrombocytopenia history)
- CBC, BMP, coagulation studies, type and screen
- ECG (AF, MI, arrhythmias)
- If ICH: drug screen (cocaine), look for coagulopathy
SECTION 11: TIME TARGETS
Table 7: NINDS Stroke Evaluation Targets (Rosen's Table 87.4 / Tintinalli's Table 167-8)
| Management Component | Target Time Frame |
|---|---|
| Door to doctor | 10 min |
| Door to stroke team notification | 15 min |
| Door to CT scan initiation | 25 min |
| Door to CT scan interpretation | 45 min |
| Door to IV tPA administration | ≤60 min (goal ≤45 min) |
| Door to monitored bed | 3 hours |
| Access to neurosurgery | 2 hours |
SECTION 12: MANAGEMENT
12.1 General Supportive Care (All Stroke Patients)
Table 8: Core ED Interventions for Suspected Acute Stroke (Tintinalli's Table 167-7)
| Intervention | Rationale |
|---|---|
| ABC assessment | Immediate life threats first; active airway management if needed |
| IV access | Required for possible thrombolytics; do NOT delay imaging for access |
| Pulse oximetry | Detect hypoxia |
| Oxygen: only if SpO₂ <94% | Routine O₂ not indicated; hyperbaric O₂ no benefit |
| Cardiac monitoring | AF (most common cardioembolic cause); arrhythmias predict mortality |
| Bedside glucose | Rule out hypoglycemia immediately; treat BG <60 with IV dextrose |
| Swallowing assessment | Withhold oral meds/fluids/food until assessed; aspiration risk |
| Avoid dextrose-containing IVF | Hyperglycemia worsens ischemic deficit |
| Correct dehydration | Increases blood viscosity; but do NOT over-hydrate |
| Fever: identify cause + treat | Fever associated with ↑ morbidity/mortality; treat source + acetaminophen |
| Stroke unit admission | Associated with decreased complications, length of stay, improved function |
Glycemic control: Target blood glucose 140-180 mg/dL. Treat hypoglycemia (<60 mg/dL) with IV dextrose. Tight control (<140) not proven beneficial and risks hypoglycemia.
12.2 Blood Pressure Management
A. Acute Ischemic Stroke - NOT receiving tPA:
- Do NOT treat unless SBP >220 mmHg or DBP >120 mmHg
- The elevated BP is a compensatory response (Cushing's) maintaining cerebral perfusion
- Exception: Treat if concurrent AMI, aortic dissection, hypertensive encephalopathy, severe CHF
B. Eligible for IV tPA (pre-treatment):
- Must achieve SBP <185 mmHg AND DBP <110 mmHg before giving tPA
- If BP does not decline to this level → DO NOT administer rtPA
Table 9: BP Management Algorithms (Tintinalli's Tables 167-9 & 167-10 / Rosen's Box 87.2)
| Scenario | BP Threshold | Agents |
|---|---|---|
| Pre-tPA (to reach <185/110) | SBP >185 or DBP >110 | Labetalol 10-20 mg IV x 1-2; OR Nicardipine 5 mg/h, titrate to 15 mg/h; OR Clevidipine 1-2 mg/h, double q2-5 min (max 21 mg/h) |
| During tPA (SBP 180-230 or DBP 105-120) | SBP 180-230 or DBP 105-120 | Labetalol 10 mg IV q10-20 min (max 300 mg) OR infusion 2-8 mg/min |
| During tPA (refractory/severe) | SBP >230 or DBP >140 | Nicardipine infusion OR sodium nitroprusside (0.5-10 mcg/kg/min); monitor arterially |
| BP monitoring after tPA | — | Every 15 min x 2h → every 30 min x 6h → every 60 min x 16h |
12.3 Reperfusion Therapy - IV Thrombolytics
Key Trials for IV Alteplase
Table 10: Major Clinical Trials for IV tPA in Acute Ischemic Stroke
| Trial | Year | n | Time Window | Key Finding |
|---|---|---|---|---|
| NINDS | 1995 | 624 | 0-3h | tPA 0.9 mg/kg vs. placebo: 13% absolute improvement in functional outcome at 3 months; sICH 6.4% vs. 0.6%; NO difference in mortality at 3 months. BASIS for FDA approval. |
| ECASS I | 1995 | 620 | 0-6h | tPA 1.1 mg/kg; primary endpoint not met; ↑ parenchymal hemorrhage rate |
| ECASS II | 1998 | 800 | 0-6h | tPA 0.9 mg/kg; no significant benefit; parenchymal hemorrhage 8.8% vs. 3.4% |
| ECASS III | 2008 | 821 | 3-4.5h | tPA vs. placebo: mRS 0-1 at 90 days 52.4% vs. 45.2% (OR 1.34; P=0.04); sICH 2.4% vs. 0.2%; expanded window to 3-4.5 hours |
| IST-3 | 2012 | 3035 | 0-6h | Largest RCT; 72% received tPA after 3h; NO significant difference in primary outcome at 6 months; favorable secondary ordinal shift in disability; sICH 7% vs. 1% |
| WAKE-UP | 2018 | ~503 | Unknown onset | MRI-guided (DWI-FLAIR mismatch); tPA vs. placebo in wake-up stroke; favorable outcome 53.3% vs. 41.8% (OR 1.61; P=0.02); sICH 2% vs. 0.4%; stopped early due to funding |
| ENCHANTED | 2016 | 3300 | 0-4.5h | Low-dose alteplase (0.6 mg/kg) non-inferior to standard dose (0.9 mg/kg) for death/disability at 90 days; significantly fewer sICH; (63% Asian population; low dose is standard in Japan but NOT current AHA guideline) |
| Cochrane Meta-analysis | 2014 | 10,187 | 0-6h | Treated patients less likely to be dead or dependent; benefit regardless of ↑ sICH and early deaths; early treatment better than late |
Alteplase Dosing
- Dose: 0.9 mg/kg IV (maximum 90 mg total)
- Administration: 10% of total dose as IV bolus over 1 minute; remaining 90% infused over 60 minutes
- Do NOT use abbreviations (rtPA, tPA); use full name "alteplase" to avoid medication errors
Tenecteplase (TNK)
- Single IV bolus (0.25 mg/kg; max 25 mg)
- EXTEND-IA TNK trial and others: similar functional outcome, sICH, and mortality vs. alteplase at 90 days
- Higher reperfusion rates before thrombectomy vs. alteplase in LVO patients
- Moderate-to-high quality evidence supports use; AHA/ASA now recommends as alternative
AHA/ASA Inclusion Criteria for IV Alteplase (Tintinalli Table 167-11 / Rosen's Table 87.5)
Within 3 hours - INCLUSION:
- Age ≥18 (no upper age limit)
- Diagnosis of acute ischemic stroke with measurable neurologic deficit
- Time of onset clearly established <3h (or last known well time)
3-4.5 hours - ADDITIONAL RESTRICTIONS:
- Age ≤80 (per older criteria; see Note below)
- No history of BOTH diabetes mellitus AND prior stroke
- NIHSS ≤25
- No oral anticoagulants
- No imaging evidence of ischemia >1/3 of MCA territory
EXCLUSION CRITERIA:
- Last known well >4.5 hours (or unknown onset without imaging selection)
- Acute intracranial hemorrhage or history of prior ICH
- Evidence of SAH
- Recent brain imaging showing extensive clear hypodensity (obvious early ischemia)
- Recent ischemic stroke or severe head trauma within 3 months
- Acute posttraumatic brain infarction
- Intracranial or intraspinal surgery within 21 days
- GI or GU bleeding within 3 months
- Active arterial puncture at non-compressible site within 7 days
- SBP persistently >185 mmHg or DBP >110 mmHg despite treatment
- Platelet count <100,000/mm³
- INR >1.7 or aPTT >40s or PT >15s
- Blood glucose <50 mg/dL (normalize first)
- Current use of GP IIb/IIIa inhibitors
- Known or suspected aortic arch dissection
- Intra-axial or extra-axial neoplasm (some exceptions)
SELECTED SPECIAL SCENARIOS:
| Condition | Guidance |
|---|---|
| Recent MI | Not a contraindication; STEMI involving left anterior, right, or inferior myocardium - can still give tPA |
| Pregnancy | May be considered for moderate-to-severe stroke |
| Seizure at onset | Not a contraindication IF residual deficit is from stroke, not postictal |
| Unruptured aneurysm <10 mm | Not a contraindication |
| Antiplatelet therapy | Give tPA - benefit outweighs small ↑ sICH risk |
| Direct oral anticoagulants (DOAC) | Do NOT give tPA unless appropriate coag labs normal OR last dose >48h (with normal renal function) |
| LMWH | Do NOT give tPA if full treatment dose given within 24h |
Post-tPA Complications
- Symptomatic ICH: 2%-7%; greatest risk with most severe strokes
- Asymptomatic ICH: 30%-45% (>10 cerebral microbleeds)
- Cerebral microbleeds (CMBs): If >10 on prior MRI, risk of sICH = 30%-47%; benefits of tPA uncertain
- PH2 hemorrhage (>30% of infarcted tissue + mass effect): ~50% mortality
Risk factors for sICH after tPA: Older age, high NIHSS, hypertension, hyperglycemia, diabetes, CHF, renal impairment, AF, antiplatelet use, leukoaraiosis, visible infarct on imaging
12.4 Endovascular Therapy - Mechanical Thrombectomy
AHA/ASA Indications for Stent Retriever Thrombectomy (0-6 hours) - Tintinalli Table 167-13
ALL 7 criteria must be met:
- Prestroke mRS 0-1 (no significant prior disability)
- Acute ischemic stroke receiving IV rtPA within 4.5h OR not eligible for rtPA
- Causative occlusion of ICA or proximal MCA (M1)
- Age ≥18
- NIHSS ≥6
- ASPECTS ≥6
- Treatment (groin puncture) initiable within 6 hours of symptom onset
Positive Thrombectomy Trials (0-6 hours)
| Trial | Year | Key Finding |
|---|---|---|
| MR CLEAN | 2015 | Thrombectomy vs. standard; absolute difference in functional independence 13.5%; first positive modern thrombectomy RCT |
| ESCAPE | 2015 | Stopped early; 90-day mRS 0-2: 53% vs. 29%; mortality 10% vs. 19% |
| EXTEND-IA | 2015 | Stopped early; 90-day functional independence 71% vs. 40% |
| SWIFT PRIME | 2015 | Stopped early; 90-day mRS 0-2: 60% vs. 35% |
| REVASCAT | 2015 | mRS 0-2 at 90 days: 43.7% vs. 28.2% |
| THRACE | 2016 | mRS 0-2: 53% vs. 42%; reinforced 0-5h window |
These 6 trials together represent a practice-changing moment in stroke treatment.
Extended Window Thrombectomy Trials (6-24 hours)
| Trial | Window | n | Key Finding |
|---|---|---|---|
| DAWN | 6-24h | 206 | Thrombectomy vs. standard; 90-day mRS 0-2: 49% vs. 13% (adjusted difference 33%); posterior probability >0.999; stopped early |
| DEFUSE 3 | 6-16h | 182 | Thrombectomy vs. standard; 90-day mRS 0-2: 45% vs. 17%; OR 2.77; stopped early |
Both DAWN and DEFUSE 3 used perfusion imaging to identify salvageable tissue (penumbra mismatch). AHA/ASA recommends extended window thrombectomy ONLY if strict inclusion/exclusion criteria of DAWN or DEFUSE 3 are met.
Timing effects: Each 1-hour delay to reperfusion → less functional independence; benefit becomes nonsignificant after 7 hours in pooled analysis.
Combined tPA + Thrombectomy: Dual therapy (tPA + thrombectomy) → higher 3-month functional independence + lower mortality vs. thrombectomy alone. Thrombectomy should NOT be delayed to assess tPA response.
12.5 Antiplatelet Therapy
Aspirin (160-300 mg oral or rectal):
- Recommended within 24-48 hours of ischemic stroke onset
- Combined International Stroke Trial (IST, n=19,435) + Chinese Acute Stroke Trial (CAST, n=20,665): significant reduction in mortality and morbidity at 4 weeks and 6 months
- DO NOT give within 24 hours of tPA
Dual Antiplatelet (Aspirin + Clopidogrel):
- POINT trial and CHANCE trial: for minor stroke or high-risk TIA, dual antiplatelet for 21 days reduces early recurrent stroke but ↑ bleeding risk
- NOT for moderate-severe stroke; most benefit in lacunar or minor stroke
ABCD2 Score for TIA Risk Stratification:
- Previously recommended by guidelines; current ACEP 2016 policy states ABCD2 should NOT be used alone to identify TIA patients safe for discharge (inadequate LR+ and LR-)
12.6 Anticoagulation
- Acute anticoagulation (heparin) in acute ischemic stroke: NOT recommended routinely
- Benefits do NOT outweigh risk of symptomatic ICH in acute stroke
- Exception: specific situations (stroke with concurrent AMI, dissection) - consult stroke specialist
12.7 Other Ischemic Stroke Management
Temperature control:
- Fever (>38°C) significantly worsens outcome
- Identify and treat source; acetaminophen for antipyresis
- Avoid ibuprofen (no temperature lowering + bleeding risk)
- Physical cooling is second-line only
- Hypothermia induction: no benefit; increased infection risk
Carotid Endarterectomy:
- For high-grade ICA lesions after TIA: best performed within 2 weeks of TIA (surgical benefit greatest)
- CREST trial: Carotid stenting vs. endarterectomy - similar functional outcomes up to 10 years
- Stenting preferred in: age <70, high surgical risk
SECTION 13: HEMORRHAGIC STROKE MANAGEMENT
13.1 ICH Management Principles
Initial goals:
- Prevent hemorrhage expansion (~20%-30% expand in first hours)
- Prevent secondary brain injury: airway + breathing + circulation
- Airway management: balance between aspiration prevention vs. loss of serial neurological exam
13.2 Blood Pressure in ICH
INTERACT2 Trial (2013): n=2839; SBP 150-220 mmHg; randomized to intensive target (SBP <140 mmHg within 1 hour) vs. standard (SBP <180 mmHg):
- Intensive lowering did NOT significantly reduce death or severe disability
- BUT improved functional outcomes at 90 days
ATACH 2 Trial: IV nicardipine within 3 hours; SBP 110-139 vs. 140-179 mmHg target:
- No difference in death/disability
- ↑ Renal adverse events in intensive group (9.0% vs. 4.0%)
Current recommendation: Target SBP <140-160 mmHg (AHA/ASA); agents: IV labetalol, nicardipine, clevidipine.
13.3 Anticoagulation Reversal
Table 11: Anticoagulation Reversal in ICH
| Agent | Reversal |
|---|---|
| Warfarin | Vitamin K (phytonadione) IV + PCC (Prothrombin Complex Concentrate) preferred over FFP; PCC: faster INR correction, lower infection risk, lower volume |
| Warfarin (if PCC unavailable) | FFP + Vitamin K |
| Dabigatran (direct thrombin inhibitor) | Idarucizumab (Praxbind) - specific reversal |
| Rivaroxaban, Apixaban (Factor Xa inhibitors) | Andexanet alfa - specific reversal; or 4-factor PCC |
| Heparin | Protamine sulfate |
| LMWH | Protamine sulfate (partial reversal) |
| Aspirin/ADP inhibitors | Consider desmopressin (ddAVP) 0.4 mcg/kg IV if proceeding to neurosurgery; platelet transfusion for neurosurgical procedures |
PCC preferred over FFP: faster INR correction, lower infection risk, lower administered volume. - Rosen's Key Concepts
Tranexamic acid (TICH2 trial, n=2325): 2g IV within 8 hours - no improvement in 90-day functional status vs. placebo; some reduction in hematoma expansion and early death.
13.4 ICP Management in ICH
- Indications for ICP monitoring: GCS ≤8; clinical transtentorial herniation; intraventricular hemorrhage or hydrocephalus
- External ventricular drain: for hydrocephalus, especially IVH blocking 3rd/4th ventricles
- Target CPP: 50-70 mmHg
- Medical therapy:
- Mannitol (0.25-1 g/kg IV): osmotic agent; safe but limited outcome improvement
- Hypertonic saline (HTS) 3% or 23.4%: more effective than mannitol (meta-analysis); 23.4% HTS for herniation reversal
- Elevate head of bed 30°; maintain normothermia; avoid hypotonic fluids
CLEAR III Trial: Alteplase irrigation of external ventricular drain vs. saline in IVH - NO improvement in functional outcomes at mRS 3 cutoff.
13.5 Seizures in ICH
- Up to 16% risk of clinical seizures within 1 week (majority at onset)
- No prophylactic antiseizure medication recommended
- Treat clinical seizures with anticonvulsants
- Continuous EEG monitoring for ICH patients with mental status out of proportion to brain injury
- Levetiracetam 1000-1500 mg IV for electrographic seizures
13.6 Surgical Management of ICH
General rule: Standard open craniotomy for spontaneous ICH has NOT been proven to improve outcomes.
STICH I (2005): Early surgical hematoma evacuation vs. conservative management - no benefit for routine surgery; subgroup trend for benefit in superficial lobar hemorrhage
STICH II (2013): Superficial lobar ICH (within 1 cm of cortex); surgery vs. conservative - no significant benefit in primary outcome
ENRICH Trial (ongoing/early results): Minimally invasive parafascicular surgery (MIPS) within 24h; early results: 52% functional independence at follow-up; no mortality in 39-patient cohort
Cerebellar hemorrhage: If >3 cm OR with brainstem compression OR hydrocephalus → NEUROSURGICAL CONSULTATION; posterior fossa decompression may be lifesaving
Decompressive craniectomy (SWITCH trial, ongoing): For basal ganglia/thalamic ICH with GCS 8-13, NIHSS 10-30, hematoma 30-100 mL
Early DNR orders: Current AHA/ASA guidelines recommend aggressive early care and to postpone new DNR orders until at least day 2 of treatment (early DNR associated with self-fulfilling prophecy)
SECTION 14: TIA MANAGEMENT
Updated Definition (AHA): "A transient episode of neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction" - tissue-based, NOT time-based.
- ~240,000 TIAs/year; ~10% stroke risk within 3 months; 50% of those in first 2 days
- Patients with DWI-negative TIA have much lower recurrence risk
Dual Antiplatelet for Minor Stroke/High-Risk TIA:
- Aspirin + Clopidogrel for 21 days (POINT trial, CHANCE trial)
- Then transition to single antiplatelet
ABCD2 Score: Age, BP, Clinical features, Duration, Diabetes - NOT sufficient alone to risk-stratify for safe discharge (ACEP 2016 Clinical Policy).
Disposition: Most TIA patients without contraindications should be hospitalized or in an expedited 24-hour TIA clinic pathway.
SECTION 15: CEREBELLAR/BRAINSTEM STROKE TREATMENT
Special management considerations:
- MRI-DWI mandatory (CT has up to 25% false-negative rate for posterior fossa)
- Close monitoring for rapid deterioration from edema and brainstem compression
- Serial exams: watch for gaze palsy, worsening ataxia, deteriorating consciousness
- Neurosurgical consultation if cerebellar hemorrhage or large cerebellar infarct
- Posterior fossa decompression may be lifesaving for large cerebellar stroke with edema
SECTION 16: STROKE IN SPECIAL POPULATIONS
Stroke with Concurrent AMI
- Aspirin appropriate for both; consult cardiology before tPA
- Recent STEMI involving left anterior, right, or inferior myocardium is NOT a contraindication to tPA
Stroke with Coagulopathy
- Consult hematology + stroke neurology
- Admit to comprehensive stroke center
Young Adults (18-50 years)
- Younger victims have MORE FAVORABLE morbidity/mortality after IV thrombolysis, thrombectomy, and decompressive surgery for large MCA strokes
- Treat aggressively
- Increasing incidence linked to: ↑ hyperlipidemia, diabetes, obesity, recreational drug use
MASTER FLOWCHART: ACUTE STROKE MANAGEMENT IN THE ED
PATIENT ARRIVES WITH SUSPECTED STROKE
│
▼
┌─────────────────────────────────────┐
│ IMMEDIATE ACTIONS (0-5 min) │
│ • ABC + Vital Signs │
│ • Bedside glucose (treat <60 dextrose)│
│ • IV access + cardiac monitor + SpO₂│
│ • ACTIVATE STROKE TEAM NOW │
│ • Last known well TIME documented │
└─────────────────────────────────────┘
│
▼
┌─────────────────────────────────────┐
│ HISTORY & EXAM (5-15 min) │
│ • Time of onset (last known well) │
│ • Medications (anticoagulants?) │
│ • NIHSS score │
│ • Posterior vs. anterior signs? │
└─────────────────────────────────────┘
│
▼
┌─────────────────────────────────────┐
│ NCCT HEAD (within 20 min) │
└─────────────────────────────────────┘
│
┌─────────────┴──────────────┐
│ │
▼ ▼
HEMORRHAGE NO HEMORRHAGE
│ │
│ ▼
│ ISCHEMIC STROKE
│ │
│ ┌─────────────┴───────────────┐
│ │ │
│ ▼ ▼
│ Within 4.5 hours? Beyond 4.5 hours
│ AND eligible? OR unknown onset
│ │ │
│ YES │ NO │
│ │ └──────────────────┐ │
│ │ BP <185/110? │ │
│ │ YES │ │
│ ▼ │ │
│ IV ALTEPLASE │ │
│ 0.9 mg/kg (max 90mg) │ │
│ Bolus 10% over 1 min │ │
│ + infusion 90% over 60 min │ │
│ │ │ │
│ └──────────┬───────────┘ │
│ │ │
│ CTA HEAD/NECK │
│ (LVO screen) │
│ │ │
│ LVO present? (ICA or M1) │
│ NIHSS ≥6, ASPECTS ≥6 │
│ │ │
│ YES │ NO │
│ ▼ │ ▼ │
│ MECHANICAL │ SUPPORTIVE │
│ THROMBECTOMY │ CARE │
│ (0-6h standard │ + Aspirin │
│ 6-24h if DAWN/ │ in 24-48h │
│ DEFUSE3 criteria│ │
│ met) │ │
│ │ │
│ PERFUSION IMAGING: │
│ DWI-FLAIR mismatch? │
│ → May extend tPA window │
│ for wake-up stroke │
│ │
▼
HEMORRHAGIC STROKE
│
├── ICH
│ • Reverse anticoagulation
│ │ (Warfarin: PCC + Vit K; DOAC: specific reversal)
│ • BP: target SBP <140-160 mmHg
│ │ (Nicardipine or Labetalol IV)
│ • ICP management if indicated
│ │ (HOB 30°; Mannitol or HTS 3%)
│ • Seizure treatment (no prophylaxis)
│ • Cerebellar hemorrhage >3cm
│ │ or brainstem compression → Neurosurgery
│ • NO early DNR (wait ≥day 2)
│ • Admit ICU / Stroke Unit
│
└── SAH
• Neurosurgical consultation STAT
• Nimodipine (vasospasm prevention)
• Avoid anticoagulants/antiplatelets
• BP control; aneurysm securing
MASTER COMPARISON TABLE: All Major Stroke Syndromes
Table 12: Comprehensive Stroke Syndrome Summary
| Artery | Territory | Classic Deficits | Ipsilateral Findings | Contralateral Findings | Distinguishing Feature |
|---|---|---|---|---|---|
| ACA | Frontal/medial cortex | Frontal syndrome | — | Leg weakness > arm; leg sensory loss | Leg >> arm |
| MCA | Lateral cortex | Hemiparesis + sensory | — | Face + arm > leg; hemianopsia | Aphasia (dominant) or Neglect (non-dominant) |
| PCA | Occipital + thalamus | Visual + memory | CN III palsy | Homonymous hemianopsia | Minimal motor; alexia without agraphia |
| Basilar | Pons + midbrain | Bilateral | Multiple CN palsies | Bilateral motor | Locked-in syndrome; coma |
| PICA/Vertebral (Wallenberg) | Lateral medulla | Crossed deficits | Horner's; facial numbness; ataxia; dysphonia | Pain + temperature loss on body | NO hemiplegia |
| Lacunar | BG/thalamus/pons/capsule | Pure motor or sensory | None | Contralateral pure deficit | No cortical signs |
| Cerebellar | Cerebellum | Ipsilateral ataxia | Ipsilateral dysmetria; ataxia | — | CT often normal; MRI required |
PROGNOSTIC FACTORS
Factors Worsening Acute Stroke Prognosis (Rosen's Key Concepts)
| Factor | Why It Worsens Outcome |
|---|---|
| Fever | ↑ Inflammatory response; ↑ metabolic demand; free radical production |
| Hypotension | Reduces cerebral perfusion; expands penumbra |
| Hypoxia | Directly extends ischemic injury |
| Hypoglycemia | Starves neurons; worsens ischemic injury |
| Hyperglycemia | Associated with worse outcomes; mechanisms include ↑ lactic acidosis |
Factors Worsening sICH Risk After tPA
| Risk Factor | Evidence Level |
|---|---|
| Older age | Strong |
| Higher NIHSS (severe stroke) | Strong |
| Hypertension | Strong |
| Hyperglycemia | Moderate |
| Diabetes mellitus | Moderate |
| Atrial fibrillation | Moderate |
| Prior antiplatelet use | Moderate |
| Leukoaraiosis on imaging | Moderate |
| Cerebral microbleeds >10 | Strong (30-47% sICH risk) |
ANTERIOR vs. POSTERIOR CIRCULATION: FINAL COMPARISON
| Feature | Anterior Circulation | Posterior Circulation |
|---|---|---|
| Consciousness | Usually preserved | Can be lost (reticular activating system) |
| Nausea/vomiting | Uncommon | Common (CTZ in brainstem) |
| Cranial nerve deficits | Rare (CN VII central) | Very common (CN III-XII) |
| Deficit laterality | Same side of body | Crossed (ipsilateral CN + contralateral body) |
| Visual symptoms | Monocular loss (ophthalmic a.) | Bilateral field defects; diplopia; nystagmus |
| Progression | Up to 24 hours | Up to 3 days |
| NIHSS detection | Well detected | Under-detected |
| CT reliability | High sensitivity | Up to 25% false-negative (posterior fossa) |
Sources: Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th Ed., Chapter 167 (Steven Go, pp. 1159-1178). Rosen's Emergency Medicine: Concepts and Clinical Practice, 10th Ed., Chapter 87 (Linda Papa & William J. Meurer, pp. 1424-1443).
This is a shared conversation. Sign in to Orris to start your own chat.