FootDrop*-AnatomicalBasis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple textbooks. Here is the complete, structured answer:
Foot Drop - Anatomical Basis
Definition
Foot drop (drop foot) is the inability to dorsiflex the foot at the ankle, causing the foot and toes to drag along the ground during the swing phase of walking. The patient compensates with a characteristic steppage (equine) gait - exaggerated hip and knee flexion to lift the foot clear of the ground.
Neuroanatomical Pathway
Root Level: L4-L5
The muscles responsible for ankle dorsiflexion are innervated primarily at the L4 and L5 spinal levels. Injury to the L5 root (most commonly from a prolapsed L4/5 disc) can produce foot drop.
The Sciatic Nerve
The sciatic nerve carries both the tibial and common peroneal (fibular) components down the posterior thigh. The peroneal (fibular) fascicles run superficially within the sciatic nerve, making them selectively vulnerable to stretch or partial lesions even before the formal bifurcation.
The sciatic nerve consistently divides in the lower third of the thigh into:
- Tibial nerve (medial component)
- Common fibular (peroneal) nerve (lateral component)
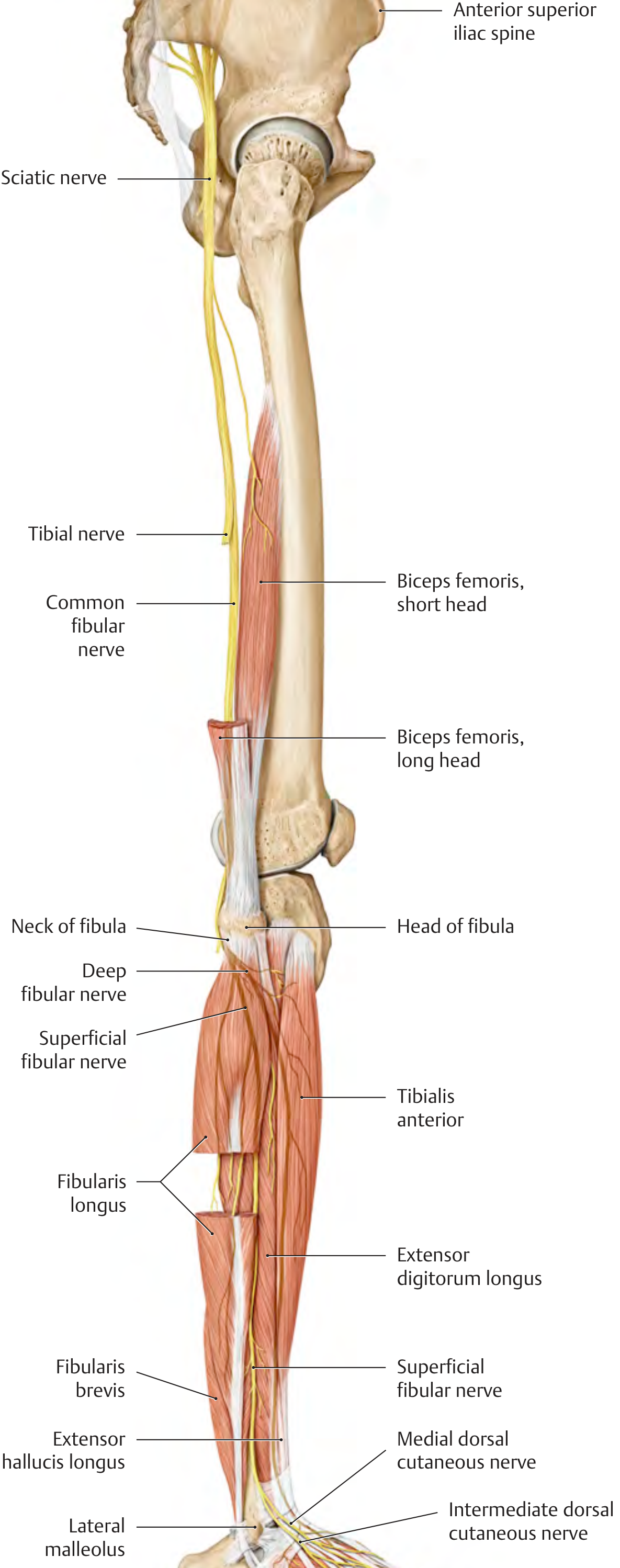
The Common Peroneal (Fibular) Nerve - The Key Structure
Course
The common peroneal nerve follows the medial border of the biceps femoris tendon through the popliteal fossa, giving off:
- Lateral sural cutaneous nerve - joins the medial sural branch to form the sural nerve
- Lateral cutaneous nerve of the calf - skin over upper lateral leg
It then rounds the head of the fibula and enters the substance of the peroneus longus muscle ("fibular tunnel"), where it divides into its two terminal branches.
The Point of Vulnerability
The nerve is most exposed and most vulnerable at the neck of the fibula. Here it is:
- Subcutaneous with no muscular protection
- Held against the fibular neck by fibrous bands at the entry of the peroneus longus
- Subject to direct compression, traction, or ischemia
"The majority of peroneal palsies occur at the level of the fibular head, where the nerve is quite superficial and susceptible to injury." - Localization in Clinical Neurology, 8e
Terminal Branches and Their Muscle Targets
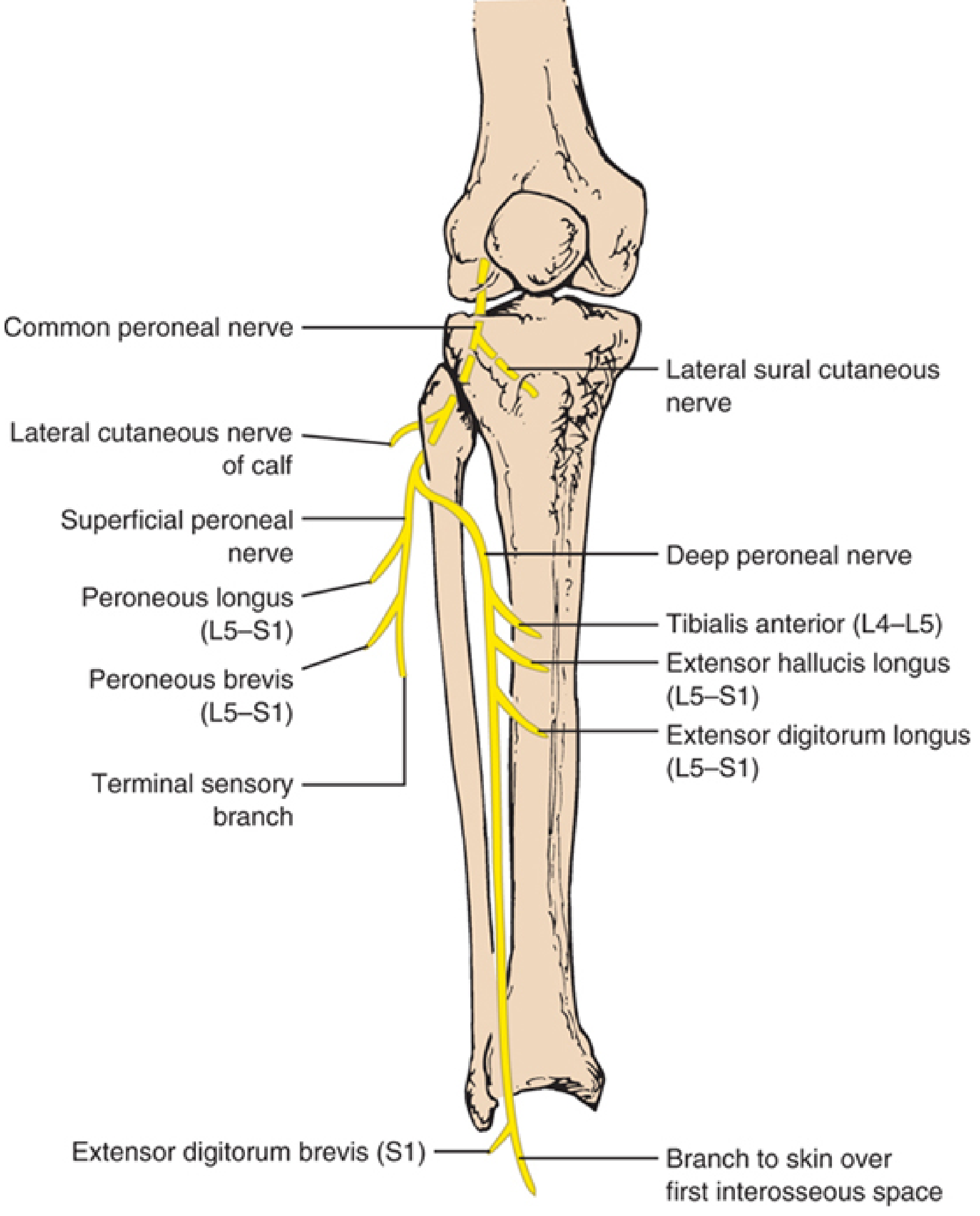
1. Deep Peroneal (Anterior Tibial) Nerve
Traverses the lateral then anterior compartment and supplies:
| Muscle | Root | Action |
|---|---|---|
| Tibialis anterior | L4-L5 | Dorsiflexion + inversion |
| Extensor hallucis longus | L5-S1 | Great toe extension + dorsiflexion |
| Extensor digitorum longus | L5-S1 | Toe extension + dorsiflexion |
| Extensor digitorum brevis | L5-S1 | Toe extension |
The terminal sensory branch supplies only a small area: skin of the first interosseous web space (between 1st and 2nd toes).
2. Superficial Peroneal Nerve
Supplies the lateral compartment:
- Peroneus longus (L5-S1) - plantar flexion + eversion
- Peroneus brevis (L5-S1) - plantar flexion + eversion
Its sensory terminal branch covers the lateral distal leg and dorsum of the foot and toes (except the first web space).
Why Foot Drop Occurs
A lesion of the common peroneal nerve at the fibular neck (before its division) causes:
- Weakness/paralysis of all dorsiflexors (tibialis anterior, EHL, EDL) → foot drop
- Weakness of evertors (peroneus longus and brevis) → foot tends to invert
- Sensory loss over the lateral distal leg and dorsum of the foot
- Steppage gait: the patient raises the knee high with each step to prevent the toe scraping the ground
"If the nerve is damaged at the level of the fibular neck before dividing into its two terminal branches, the result is weakness or paralysis of the anterior and lateral compartment muscles, resulting in foot drop with some inversion." - THIEME Atlas of Anatomy, General Anatomy & Musculoskeletal System
Anatomical Causes of Vulnerability at the Fibular Head
| Mechanism | Examples |
|---|---|
| External compression | Leg crossing, prolonged squatting, casts, stockings, anesthesia positioning |
| Trauma/stretch | Fibular fracture, knee dislocation, forced inversion (punter's palsy), postarthroplasty |
| Surgical/iatrogenic | Lithotomy position, lateral decubitus positioning, knee arthroscopy |
| Intraneural ganglion | Synovial fluid dissects from superior tibiofibular joint along articular branch (accounts for up to 50% of idiopathic cases) |
| Wasting | Weight loss, anorexia nervosa, bedridden patients (slimmer's paralysis) |
| Postpartum | Stirrup compression or hand pressure during pushing |
Level-Dependent Clinical Patterns
| Level of Lesion | Motor Loss | Sensory Loss | Special Feature |
|---|---|---|---|
| L5 root | Dorsiflexion + eversion + inversion (tibialis posterior) + hip abduction (gluteus medius) | Anterior leg, dorsum of foot, extending near knee | Tibialis posterior weakness distinguishes it from peroneal palsy |
| Sciatic nerve (peroneal fascicles) | Same as common peroneal | Same as common peroneal | Short head of biceps femoris also weak (EMG key) |
| Common peroneal at fibular neck | Dorsiflexion + eversion; inversion spared | Lateral leg + dorsum of foot | Most common; inversion intact because tibialis posterior (tibial nerve) is intact |
| Deep peroneal only | Dorsiflexion only; eversion spared | First web space only | Compartment syndrome, anterior tarsal tunnel syndrome |
| Superficial peroneal only | Eversion only | Lateral leg + dorsum of foot (not web space) | No gait disturbance unless severe |
The Key Clinical Differentiator: Peroneal Nerve vs. L5 Radiculopathy
"Weakness in dorsiflexion and eversion of the foot is referable either to the peroneal nerve or to the L5 nerve root; however, if there is weakness of inversion of the foot, innervated by the tibial nerve, the fault must be with the L5 root, not with the peroneal nerve. Conversely, if inversion is spared in a foot drop, the lesion is in the peroneal nerve." - Adams and Victor's Principles of Neurology, 12th Edition
Additionally, in L5 radiculopathy, the sensory loss extends nearly to the knee on the anterior foreleg, while in peroneal neuropathy it ends only a limited distance above the ankle.
Additional Anatomical Notes
- In 20-28% of individuals, an accessory deep peroneal nerve arises from the superficial peroneal nerve and wraps around the lateral malleolus to supply part of extensor digitorum brevis - this must be considered during electrodiagnostic testing
- In some peroneal neuropathies, the extensor hallucis longus is selectively most affected (producing "big toe drop") due to the specific fascicular arrangement within the common peroneal nerve
- The tibialis anterior tendon rupture is a non-neurogenic mimic of foot drop - distinguished by a palpable tendon defect, absence of toe extensor weakness, and normal EMG
Sources:
- Localization in Clinical Neurology, 8e, pp. 145-156 (Common Peroneal Nerve and Lesions)
- THIEME Atlas of Anatomy, General Anatomy & Musculoskeletal System, p. 565 (Fibular nerve course and foot drop)
- Adams and Victor's Principles of Neurology, 12th Ed., Peripheral Nerve Localization
- Bradley and Daroff's Neurology in Clinical Practice, Common Fibular Neuropathy
- Imaging Anatomy: Bones, Joints, Vessels and Nerves, Peroneal Nerve
This is a shared conversation. Sign in to Orris to start your own chat.