Now I have all the content needed. Let me compile the comprehensive 10-mark answer:
SHOULDER ARTHROSCOPY
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Miller's Review of Orthopaedics 9th Ed | Thieme Atlas of General Anatomy and Musculoskeletal System
DEFINITION
Shoulder arthroscopy is a minimally invasive surgical technique using a small-diameter telescope (arthroscope) inserted through small portals to visualize, diagnose, and treat pathology within the glenohumeral joint and subacromial space. Initially purely diagnostic, it has evolved to become the primary therapeutic approach for most shoulder conditions, replacing open surgery in most scenarios. The only procedure not yet achievable arthroscopically is endoprosthesis.
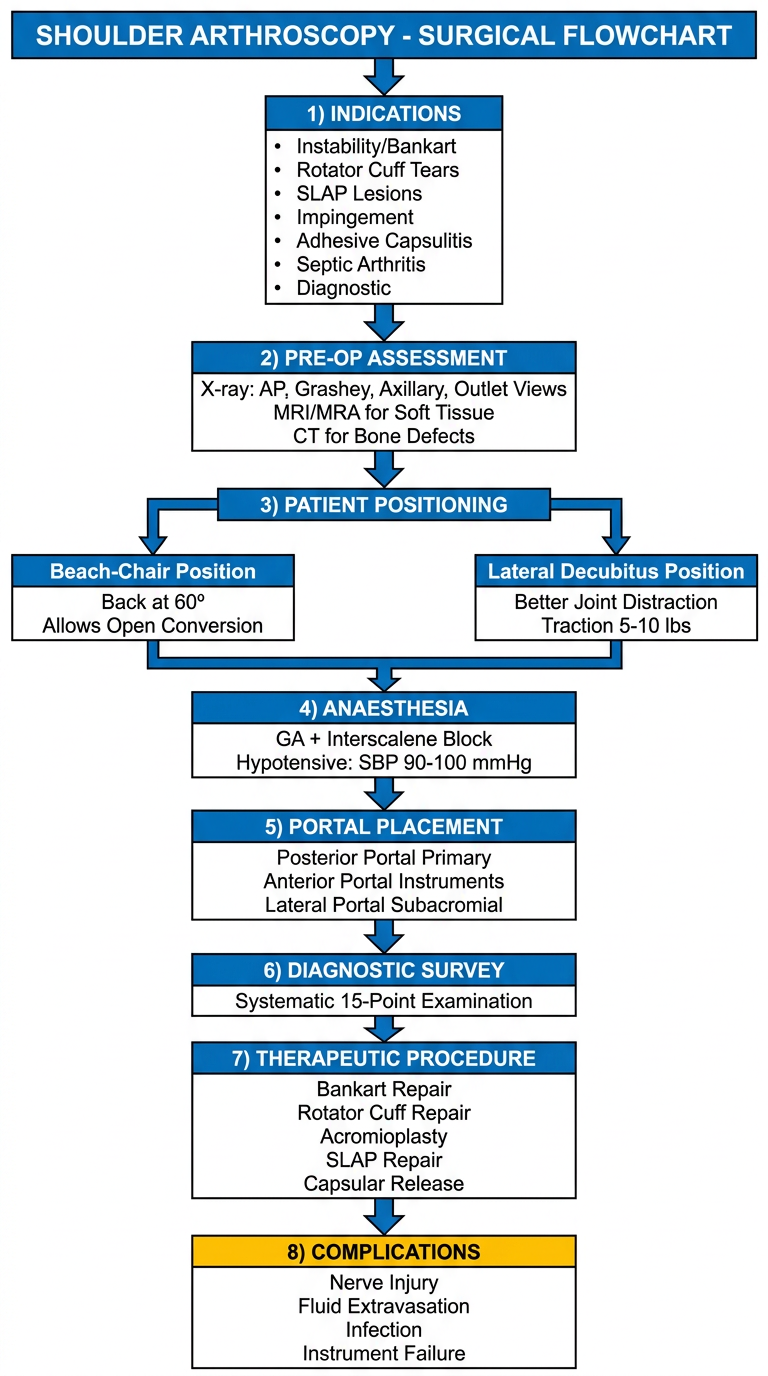
INDICATIONS
Conditions are classified into three broad groups (Thieme Atlas):
1. Instability Lesions
- Labral lesions (Bankart lesion - anteroinferior labral tear)
- Osteochondral lesions (Hill-Sachs lesion - posterior humeral head impaction fracture)
- HAGL (Humeral Avulsion of Glenohumeral Ligament)
- SLAP (Superior Labrum Anterior to Posterior) tears
- Multidirectional instability
2. Degenerative / Traumatic Conditions
- Partial or complete rotator cuff rupture (repair or debridement)
- Subacromial impingement syndrome (acromioplasty, bursectomy)
- Calcific tendinitis (tendinosis calcarea)
- Biceps tendon pathology (tenotomy / tenodesis)
- Acromioclavicular joint pathology
3. Inflammatory Conditions
- Synovitis / synovialitis
- Adhesive capsulitis (frozen shoulder) - capsular release
- Septic arthritis - irrigation and debridement
- Loose body removal
PRE-OPERATIVE ASSESSMENT
Radiographs required (Campbell's):
- AP view with arm in external rotation
- True AP (Grashey view) with arm in internal rotation
- Scapular outlet view
- Axillary lateral view
- Special: West Point, Bergeneau, Stryker notch views (for bony defects in instability)
Advanced imaging:
- MRI: Evaluates soft-tissue structures, best for rotator cuff pathology
- MRA (Magnetic Resonance Arthrography): Best for capsulolabral pathology, SLAP tears, HAGL lesions
- 3D CT: Quantifies bony defects (glenoid bone loss, Hill-Sachs) and guides decision-making
PATIENT POSITIONING & ANAESTHESIA
Two standard positions are used:
1. Beach-Chair Position (Semi-Fowler)
- Patient sits upright with back flexed at 60°
- Shoulder overhangs the edge of the table
- Advantages:
- Allows full arm rotation and abduction during surgery
- No repositioning needed if conversion to open required
- Easier orientation (normal anatomical position)
- Arm traction weights can be applied for joint distraction
- Disadvantage: Slightly less joint distraction than lateral decubitus
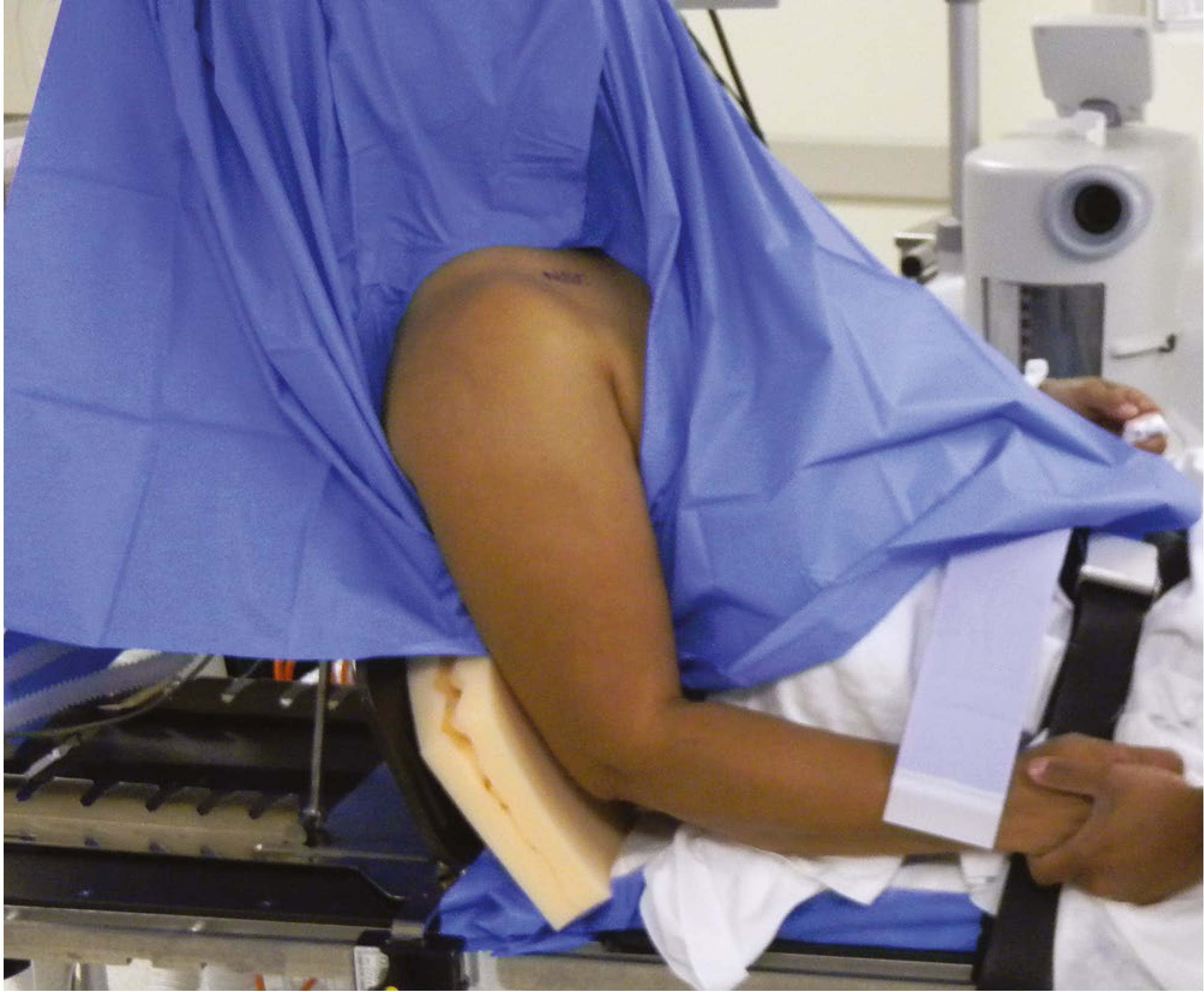
2. Lateral Decubitus Position
- Patient placed on their side with the operative shoulder up
- Arm placed in traction (5-10 lbs) at 45° abduction and 15° forward flexion
- Advantages: Superior glenohumeral joint distraction, excellent inferior recess access
- Disadvantage: Repositioning required if open conversion needed; higher brachial plexus stretch risk
Anaesthesia: General anaesthesia combined with interscalene brachial plexus block. Hypotensive anaesthesia (systolic BP 90-100 mmHg) is the most effective means of hemostasis. A systolic-to-pump pressure gradient of ~40 mmHg should be maintained.
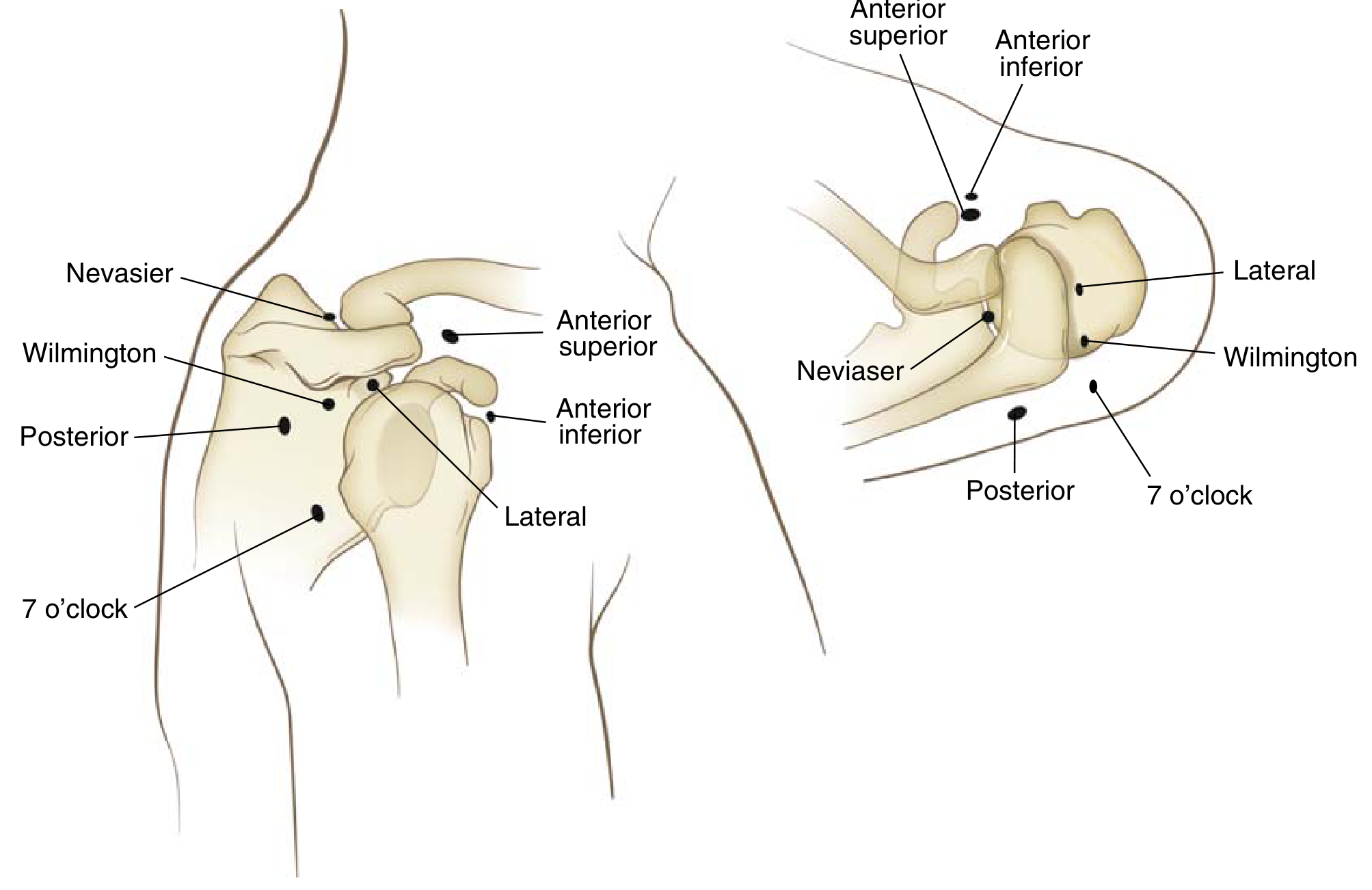
ARTHROSCOPIC PORTALS
Standard Portals (Miller's Review)
| Portal | Location | Primary Use |
|---|
| Posterior | 2 cm distal + medial to posterolateral acromial border (posterior "soft spot") | PRIMARY VIEWING portal; camera |
| Anterior | Just anterior to AC joint; lateral to coracoid tip, above subscapularis | Working/instrument portal |
| Lateral | 1-2 cm distal to lateral acromial edge | Subacromial space access |
Additional Portals
| Portal | Location | Use |
|---|
| Neviaser (supraspinatus) | Through supraspinatus fossa, superior | Anterior glenoid visualization, SLAP repair |
| Anterolateral / Wilmington | Just anterior to posterolateral corner (PLC) of acromion | SLAP repair, rotator cuff repair |
| Anteroinferior (5 o'clock) | 5 o'clock position on glenoid face | Bankart repair, anterior stabilization |
| Posteroinferior (7 o'clock) | 7 o'clock position | Posterior stabilization procedures |
Neurovascular Hazards at Each Portal (Miller's Review)
- Posterior portal: Axillary nerve (inferior), suprascapular nerve, suprascapular artery
- Anterior portals: Cephalic vein, axillary artery, axillary nerve
- Superior portals: Suprascapular artery, suprascapular nerve
- The axillary nerve is approximately 12 mm distal to the 6 o'clock position of the glenoid
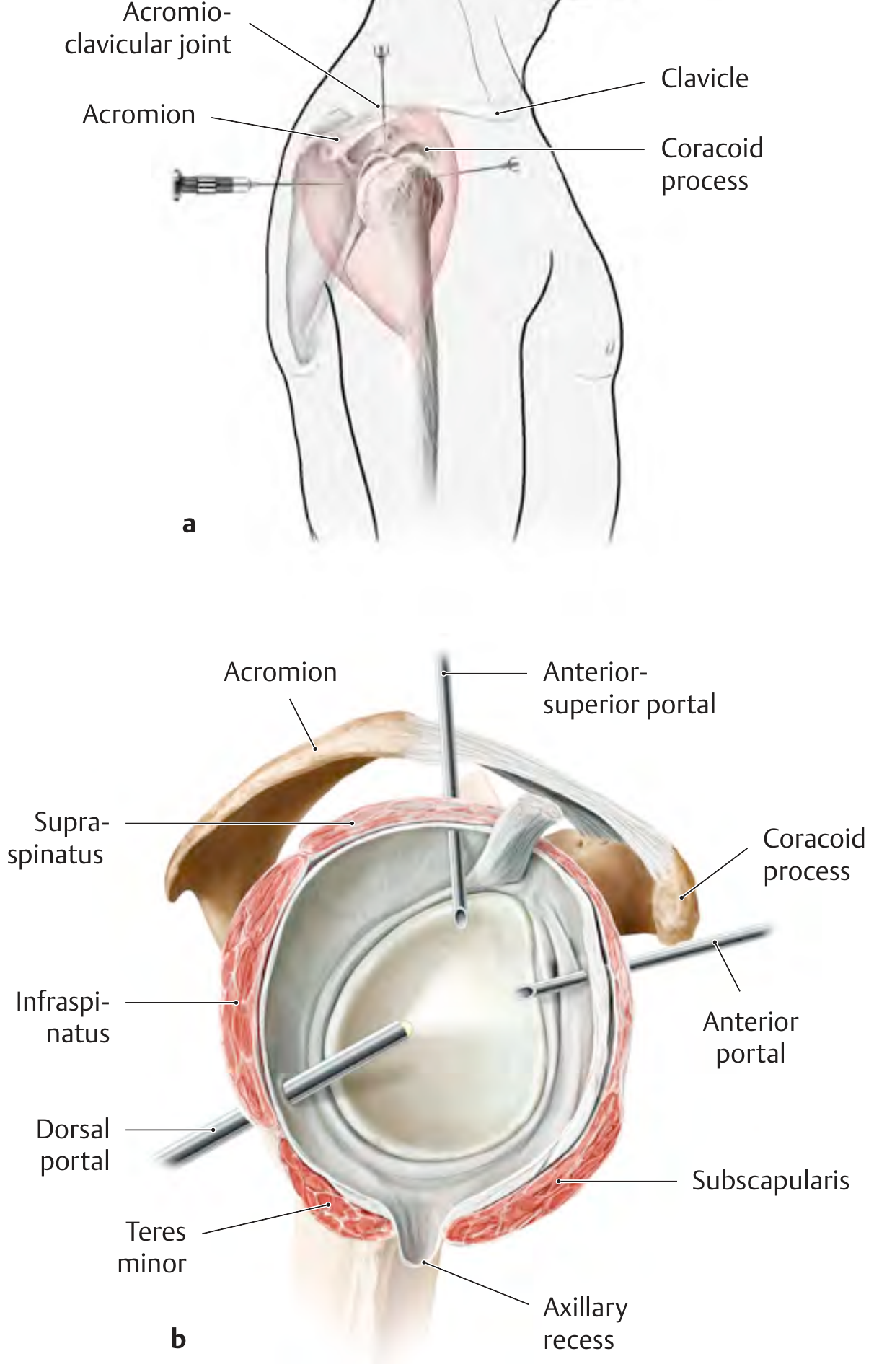
TECHNIQUE (Campbell's Technique 57.1)
Step-by-step procedure:
-
Joint insufflation: Insert 18-gauge spinal needle through posterior soft spot, directed toward coracoid tip. Inject 30-40 mL saline for joint distention - this distracts the humeral head from glenoid, making trocar entry safer and reducing chondral injury risk.
-
Posterior portal creation: Incise skin only (No. 11 blade, epidermis + dermis only - avoid deep deltoid penetration to prevent bleeding). Insert cannula + blunt trocar directed anteromedially toward coracoid.
-
Trocar navigation: Palpate bony scapular neck and glenoid with the blunt tip. Slide trocar laterally to locate the glenoid rim (felt as a small ridge). Entry site just lateral to this ridge ensures passage through muscular rotator cuff, not the tendinous portions.
-
Local anaesthetic injection: 20 mL diluted epinephrine (1:100,000) injected into portal sites and subacromial space to minimize bleeding. Verify no vessel is being injected before injection.
-
Arthroscope insertion: 30°-angled arthroscope introduced through posterior (dorsal) portal. Joint is washed with irrigant fluid.
-
Diagnostic survey: Systematic evaluation of all intraarticular structures (see below).
-
Anterior portal creation: Using inside-out or outside-in technique under direct vision, create anterior working portal for instruments.
-
Therapeutic procedure: Based on findings.
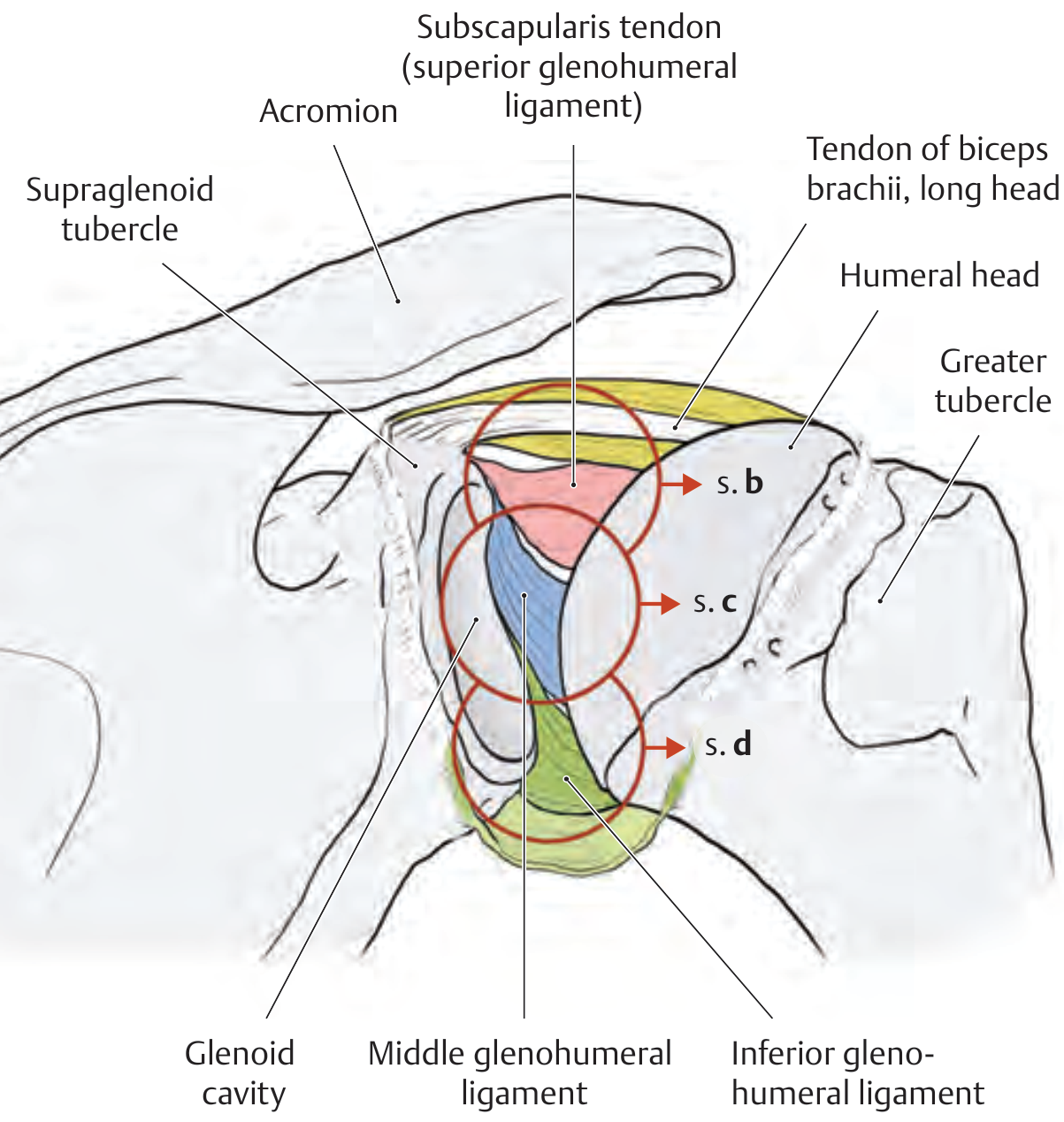
ARTHROSCOPIC ANATOMY & DIAGNOSTIC SURVEY
A standardized diagnostic survey should evaluate:
Intra-articular structures visible:
- Articular surface of humeral head (Hill-Sachs, chondral damage)
- Glenoid fossa articular surface (chondral lesions)
- Superior labrum and biceps anchor (SLAP lesions)
- Anterior labrum and inferior glenohumeral ligament (Bankart lesion)
- Posterior labrum and capsule
- Middle glenohumeral ligament (Buford complex)
- Subscapularis tendon (partial tears, HAGL)
- Rotator interval
- Supraspinatus and infraspinatus footprints (rotator cuff tears)
- Synovium, axillary recess
Subacromial space survey (via lateral portal):
- Bursal surface of rotator cuff
- Coracoacromial ligament
- Undersurface of acromion (acromial morphology - Types I, II, III)
- AC joint
CONTROL OF BLEEDING / FLUID MANAGEMENT
Hemostasis methods (Campbell's):
- Add 1 mL of 1:1000 epinephrine per 3000 mL irrigant bag (if no cardiac contraindications)
- Hypotensive anaesthesia: SBP 90-100 mmHg is most effective
- Maintain systolic-to-pump pressure gradient of ~40 mmHg
Fluid extravasation:
- More problematic in shoulder than knee arthroscopy (increased depth of tissues)
- Monitor for neck/airway swelling
- Preserve muscle fascial layers to prevent extravasation
- Use lowest effective pump pressure
FLOWCHART
COMMON PROCEDURES PERFORMED
| Procedure | Indication |
|---|
| Bankart repair (suture anchors) | Anterior shoulder instability, recurrent dislocation |
| Rotator cuff repair (single/double row) | Full or partial thickness rotator cuff tears |
| Acromioplasty + bursectomy | Subacromial impingement |
| SLAP repair | Superior labrum anterior-posterior tears |
| Capsular release | Adhesive capsulitis (frozen shoulder) |
| Biceps tenotomy/tenodesis | Biceps tendon pathology |
| Bankart + Remplissage | Large Hill-Sachs lesion with instability |
| Loose body removal | OA, synovial chondromatosis |
| Irrigation + debridement | Septic arthritis |
COMPLICATIONS
General Complications
| Complication | Details |
|---|
| Neurological (most common) | Transient paresthesia: 10-30% incidence; usually from excessive traction on shoulder. Axillary nerve, suprascapular nerve most at risk. Majority are isolated sensory (branch to teres minor - hardest to detect clinically) |
| Fluid extravasation | Can cause airway compromise from neck swelling; monitor continuously |
| Infection | Septic arthritis post-arthroscopy (rare) |
| Instrument failure | Broken instruments, shaver damage |
| Iatrogenic chondral injury | During portal creation or scope manipulation |
| Thromboembolic | DVT/PE (rare compared to lower extremity) |
Portal-Specific Risks
- Posterior portal: Suprascapular nerve (too medial) + axillary nerve (too inferior/lateral)
- Anterior portals: Cephalic vein, axillary artery
- Superior/Neviaser portal: Suprascapular artery and nerve
Risk minimized by: Adequate visualization through hemostasis, avoiding chondral abrasion, maintaining adequate flow with thermal devices, preserving muscle fascial layers.
ADVANTAGES OF ARTHROSCOPY OVER OPEN SURGERY
| Feature | Arthroscopy | Open Surgery |
|---|
| Incision size | Stab incisions (5-10 mm) | Large |
| Visualization | Excellent, magnified, all recesses | Limited |
| Hospital stay | Day case / overnight | 2-4 days |
| Recovery | Faster | Slower |
| Post-op pain | Less | More |
| Dynamic assessment | Yes (capsule/ligament) | No |
| Infection risk | Lower | Higher |
| Conversion possible | Yes (beach-chair) | N/A |
SUMMARY MNEMONICS
Portals: "PALS"
- Posterior (primary viewing)
- Anterior (instruments)
- Lateral (subacromial)
- Special (Neviaser, Wilmington, 5 o'clock, 7 o'clock)
Indications: "IDA"
- Instability (Bankart, SLAP, MDI)
- Degenerative (rotator cuff, impingement, calcific tendinitis)
- Adhesive + inflammatory (capsulitis, synovitis, septic)
Complications: "FNIIT"
- Fluid extravasation
- Neuropathy (axillary, suprascapular)
- Infection
- Iatrogenic chondral injury
- Thromboembolism
References: Campbell's Operative Orthopaedics 15th Ed 2026, pp. 3151-3155; Miller's Review of Orthopaedics 9th Ed; Thieme Atlas of General Anatomy and Musculoskeletal System, pp. 290-291