Neutropenia .
Reading File
Finding Sources
Finding Sources
Searching PubMed
neutropenia management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive material to write a full, well-structured response on neutropenia.
Neutropenia
Definition
Neutropenia is defined as an absolute neutrophil count (ANC) below 1500/µL in White adults, and below ~1200-1300/µL in Black adults (a genetically lower normal baseline, not pathological). Agranulocytosis refers to severe neutropenia, typically ANC <500/µL, often with concomitant depletion of eosinophils and basophils.
ANC calculation:
ANC = (% neutrophils + % bands) × total WBC ÷ 100
Severity Classification
| Category | ANC | Infection Risk |
|---|---|---|
| Mild | 1000–1500/µL | Minimally increased |
| Moderate | 500–1000/µL | Moderately increased |
| Severe | <500/µL | Markedly increased |
| Agranulocytosis | <200/µL | Life-threatening |
Risk rises sharply below 500 cells/µL. Patients with chemotherapy-induced or marrow-failure neutropenia have far higher infection rates than those with chronic immune-mediated or constitutional neutropenia at equivalent ANC levels. - Goldman-Cecil Medicine, p. 1765
Pathophysiology
Neutropenia arises through four main mechanisms (Henry's Clinical Diagnosis, p. 2204):
- Decreased production - proliferation or maturation defects (e.g., chemotherapy, aplastic anemia, congenital disorders)
- Increased peripheral destruction - immune-mediated (antibodies against neutrophils) or consumption in overwhelming sepsis
- Altered distribution - shift from circulating pool to marginating pool (e.g., sepsis-induced complement activation causes increased margination)
- Combinations of the above
Bone Marrow Morphology (Robbins Basic Pathology)
- Compensatory hypercellularity when destruction exceeds production, or in ineffective granulopoiesis (e.g., megaloblastic anemia)
- Selective loss of granulocytic precursors with preserved erythroid and megakaryocytic elements - seen in drug-induced selective suppression
- Panhypocellularity with myelotoxic chemotherapy agents
Causes / Etiology
Congenital Neutropenias
| Condition | Mechanism/Gene | Key Features |
|---|---|---|
| Severe Congenital Neutropenia (Kostmann syndrome) | ELANE mutation (AD, ~50%); HAX-1 mutation (AR) | ANC typically <200/µL; promyelocyte/myelocyte arrest in marrow; risk of AML/MDS transformation |
| Cyclic Neutropenia | ELANE mutation (AD) | Episodic neutropenia every ~21 days, lasting 4-6 days; stomatitis, pharyngitis, cellulitis |
| Shwachman-Diamond syndrome | SBDS gene | Neutropenia + exocrine pancreatic insufficiency |
| Fanconi Anemia | DNA repair pathway genes | Aplastic anemia + congenital anomalies; chromosome breakage with DEB/MMC test |
| Chédiak-Higashi syndrome | LYST gene | Neutropenia + giant granules + partial albinism + immunodeficiency |
| Myelokathexis | CXCR4 (WHIM syndrome) | Hypersegmented, pyknotic neutrophils retained in marrow |
| Barth syndrome | Tafazzin (X-linked) | Neutropenia + cardiomyopathy + skeletal myopathy |
| Duffy-null associated neutrophil count (DANC) | Benign ethnic neutropenia | Common in African/Middle Eastern descent; lower baseline ANC, not clinically significant |
- Goldman-Cecil Medicine, p. 1767-1768
Acquired (Secondary) Neutropenias
Drug-induced (most common cause):
- Predictable, dose-dependent: antineoplastics, AZT, ganciclovir, TMP-SMX, chloramphenicol, allopurinol
- Idiosyncratic immune-mediated: clozapine, carbimazole/methimazole/PTU (antithyroids), quinidine, procainamide, sulfasalazine, levamisole (cocaine adulterant)
- Typically presents 1-2 weeks after drug initiation; recovery within 3-10 days of stopping. Mortality from drug-induced agranulocytosis is 2.5-10%. G-CSF speeds recovery.
Infection-related:
- Viral: varicella, measles, rubella, EBV, CMV, HIV, hepatitis A/B, parvovirus, influenza
- Atypical: M. tuberculosis, ehrlichiosis, rickettsia, tularemia, brucellosis
- Overwhelming sepsis: consumption of marrow neutrophil reserves + margination from complement activation (mainly in neonates and elderly)
Immune-mediated:
- Primary autoimmune neutropenia (infants/children - usually benign, self-resolving)
- Secondary: Felty syndrome (RA + splenomegaly + neutropenia), SLE, Sjögren syndrome
- Large granular lymphocyte (LGL) leukemia - cytotoxic T cells/NK cells suppress myelopoiesis
- Alloimmune neonatal neutropenia (maternal-fetal antigen incompatibility)
Bone marrow failure/replacement:
- Aplastic anemia, myelodysplastic syndrome (MDS), acute leukemia
- Marrow infiltration by metastatic carcinoma
- Radiation injury
Nutritional deficiencies:
- B12, folate (cause ineffective granulopoiesis - often pancytopenia)
- Copper deficiency
Margination and hypersplenism:
- Splenomegaly causes sequestration and accelerated neutrophil removal
Chronic idiopathic neutropenia in adults (CINA):
- Diagnosis of exclusion after excluding all above causes with bone marrow biopsy
Diagnostic Approach
The diagnostic flowchart below (from Goldman-Cecil Medicine) guides workup:
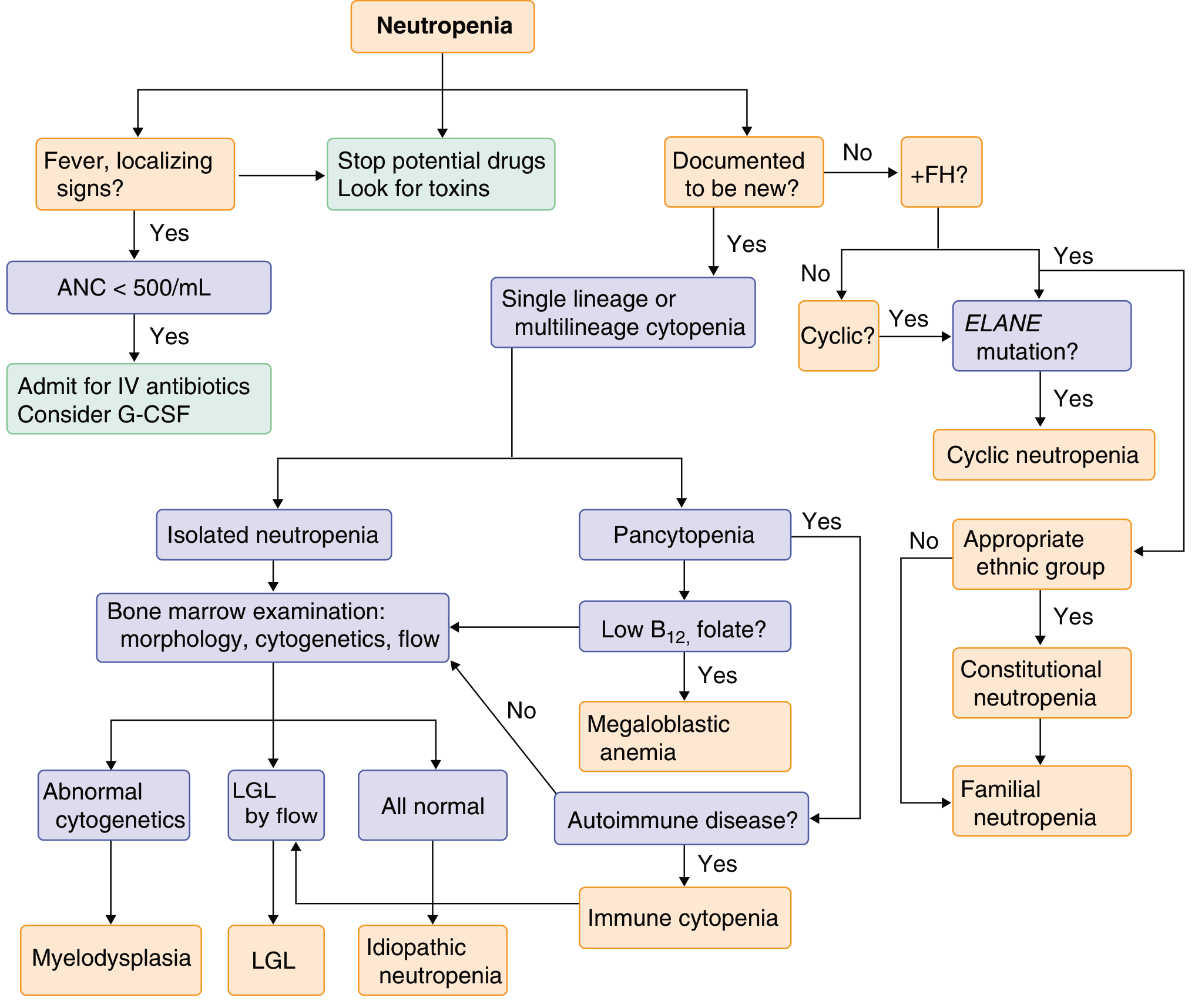
Step-by-step:
- Fever/localizing signs? - If ANC <500/µL: admit for IV antibiotics + consider G-CSF
- Stop potential drugs, look for toxins
- Is neutropenia new or chronic?
- New + family history → test for ELANE mutation → consider cyclic neutropenia or familial neutropenia
- If cyclic pattern on serial CBCs → cyclic neutropenia
- Single lineage vs multilineage?
- Pancytopenia → check B12/folate (megaloblastic anemia) → autoimmune disease? → bone marrow exam
- Isolated neutropenia → bone marrow exam: morphology, cytogenetics, flow cytometry
- Bone marrow findings:
- Abnormal cytogenetics → myelodysplasia
- LGL on flow → LGL leukemia
- All normal → chronic idiopathic neutropenia
In children with persistent, severe, or syndromic neutropenia, serial CBC (every 1-2 weeks for 6 weeks) can document cyclic pattern. Genetic testing is increasingly important.
Clinical Features
- Infections are the dominant manifestation - especially gram-positive and gram-negative bacteria, and fungi
- Classic sites: gingiva, buccal mucosa, pharynx, floor of mouth, skin, perianal region, lungs
- Ulcerating, necrotizing oral lesions ("agranulocytic angina") - contain large masses of organisms without pus (no neutrophils to form pus)
- Systemic: malaise, chills, fever
- Fever may be the ONLY sign of infection - normal inflammatory response (redness, swelling, purulence) is absent without neutrophils
- Hypothermia on presentation (<36.5°C) may indicate higher mortality than fever
Febrile Neutropenia - Emergency Management
Febrile neutropenia is a medical emergency. Defined as:
- Single temperature ≥ 38.3°C, OR
- Temperature ≥ 38.0°C sustained for ≥1 hour
- In a patient with ANC <500/µL (or ANC expected to drop below 500 within 48 hours)
20-30% of febrile neutropenic patients require hospitalization; ~10% do not survive to discharge. Common causes: pneumonia, anorectal lesion, skin infection, pharyngitis, UTI.
Evaluation
- At least 2 sets of blood cultures before starting antibiotics (one from each lumen of central lines; one peripheral)
- Cultures from suspected sites (sputum, urine, wound)
- CBC, BMP, LFTs, chest X-ray
- Avoid digital rectal exam and rectal temperatures (risk of bacteremia from disrupted rectal flora)
- CT if clinically indicated
Treatment
- Empiric broad-spectrum IV antibiotics within 30-60 minutes of presentation
- Monotherapy with an anti-pseudomonal beta-lactam is standard: piperacillin-tazobactam, cefepime, meropenem, or imipenem
- Pseudomonas aeruginosa is the key organism to always cover
- Add vancomycin if: catheter-related infection, skin/soft tissue infection, hemodynamic instability, MRSA colonization
- Add antifungal coverage if: fever persists >4-7 days despite antibiotics, or high-risk setting
- G-CSF may be added in high-risk cases (Goldman-Cecil Medicine, p. 1769-1770; Rosen's Emergency Medicine)
MASCC Risk Score
Used to identify low-risk patients who may be managed as outpatients with oral antibiotics (ciprofloxacin + amoxicillin-clavulanate).
Treatment of Non-Febrile Neutropenia
| Type | Treatment |
|---|---|
| Drug-induced | Stop offending agent; G-CSF speeds recovery |
| Chemotherapy-induced | Antibiotic prophylaxis (quinolone or TMP-SMX) if profound prolonged neutropenia expected; G-CSF prophylaxis if ≥20% risk of febrile neutropenia |
| Immune neutropenia | Steroids, antithymocyte globulin, cyclophosphamide; G-CSF (may trigger RA flare) |
| LGL syndrome | Low-dose methotrexate (10 mg/m² weekly), cyclosporine (2-10 mg/kg/day), or cyclophosphamide (50-100 mg/day) |
| Congenital/cyclic neutropenia | Chronic daily G-CSF subcutaneously (lowest effective dose, target ANC 300-500); cyclic neutropenia is NOT associated with increased leukemic risk |
| Severe congenital neutropenia | G-CSF at higher doses; monitor for AML/MDS transformation; SCT is curative for refractory/severe cases |
| CINA in adults | Reserve G-CSF for febrile episodes only (unless recurrent infections); low-bacterial diet is NOT evidence-based |
| B12/folate deficiency | Replacement therapy |
| Underlying autoimmune disease | Treat primary disease |
Stem cell transplantation is curative for congenital neutropenia and bone marrow failure syndromes (Fanconi anemia, etc.) but is reserved for severe, refractory cases. - Goldman-Cecil Medicine, p. 1770
Cyclic Neutropenia - Key Points
- Autosomal dominant, ELANE mutation
- ~21-day cycle; nadir lasts 4-6 days
- Stomatitis, pharyngitis, lymphadenitis, cellulitis during nadirs
- Risk of serious infections (Clostridium septicum bacteremia is classic)
- Managed with G-CSF; NOT associated with AML/MDS transformation (unlike severe congenital neutropenia)
- Goldman-Cecil Medicine, p. 1767
Key Points Summary
- ANC <500/µL: markedly increased infection risk; fever = emergency
- Drug-induced neutropenia is the most common cause overall
- Viral infections cause transient self-limited neutropenia
- Always check for Duffy-null genetic background in asymptomatic patients of African/Middle Eastern descent before labeling as neutropenic
- Fever may be the only sign of severe infection - empiric antibiotics must not be delayed
- G-CSF is the cornerstone of treatment for congenital and chemotherapy-related neutropenia
- No role for low-bacterial diet in neutropenic cancer patients
Sources: Goldman-Cecil Medicine International Edition, pp. 1765-1770 | Robbins & Kumar Basic Pathology, p. 2126-2134 | Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 2204-2228 | Rosen's Emergency Medicine, pp. 2481-2484 | Tintinalli's Emergency Medicine, p. 1292-1308 | Fishman's Pulmonary Diseases, Table 123-6
This is a shared conversation. Sign in to Orris to start your own chat.