I have everything I need. Now I'll write the full, student-friendly, deeply explained guide.
The Basal Ganglia - A Complete First-Principles Guide for Medical Students
PART 1: THE BIG PICTURE - What Are the Basal Ganglia and Why Do They Exist?
Before we name a single structure, let's understand the problem the basal ganglia solve.
The Problem
Your motor cortex (the part of your brain that sends "move!" signals to your muscles) is like a powerful car engine. But an engine without a gearbox, a brake, and a throttle is dangerous - it either runs flat out or stalls. The brain has the same challenge: how do you take a thought ("I want to pick up this cup") and turn it into a smooth, controlled, purposeful movement - while also suppressing all the other movements your muscles could be making at the same time?
That is exactly what the basal ganglia do. They act as the motor control supervisor - they don't create movement directly, they refine and filter movement signals coming from the cortex. They help you:
- Start the right movements
- Suppress unwanted or competing movements
- Scale the speed and force of movement appropriately
- Keep movements smooth and automatic once learned
Think of it like a music producer at a mixing board. The cortex is the raw music (loud, messy). The basal ganglia are the producer - turning certain tracks up, others down, so the final output is clean and coherent.
Critical first fact: The basal ganglia never directly talk to your muscles. They don't project to the spinal cord. They work entirely by modulating activity in the motor cortex through a relay station called the thalamus.
Beyond Movement
Here's something students often miss: the basal ganglia also handle cognition, emotion, and reward. Different parts of the same circuit process:
- Motor control (movement)
- Executive thinking (planning, decisions)
- Emotional responses
- Reward and motivation (including drug addiction)
This is why diseases of the basal ganglia (Parkinson's, Huntington's) don't just cause movement problems - they also cause depression, dementia, and personality changes. Same circuit, different channels.
PART 2: ANATOMY - Meet the Team
Term to know first - "Nucleus" (plural: nuclei): In neuroanatomy, a nucleus is a cluster of neuron cell bodies deep inside the brain (not the nucleus inside a cell). Think of it as a "neighborhood" of neurons grouped together because they work as a team.
Term to know - "Gray matter": Parts of the brain rich in neuron cell bodies look grayish. The basal ganglia are gray matter structures buried deep inside the white matter of the brain.
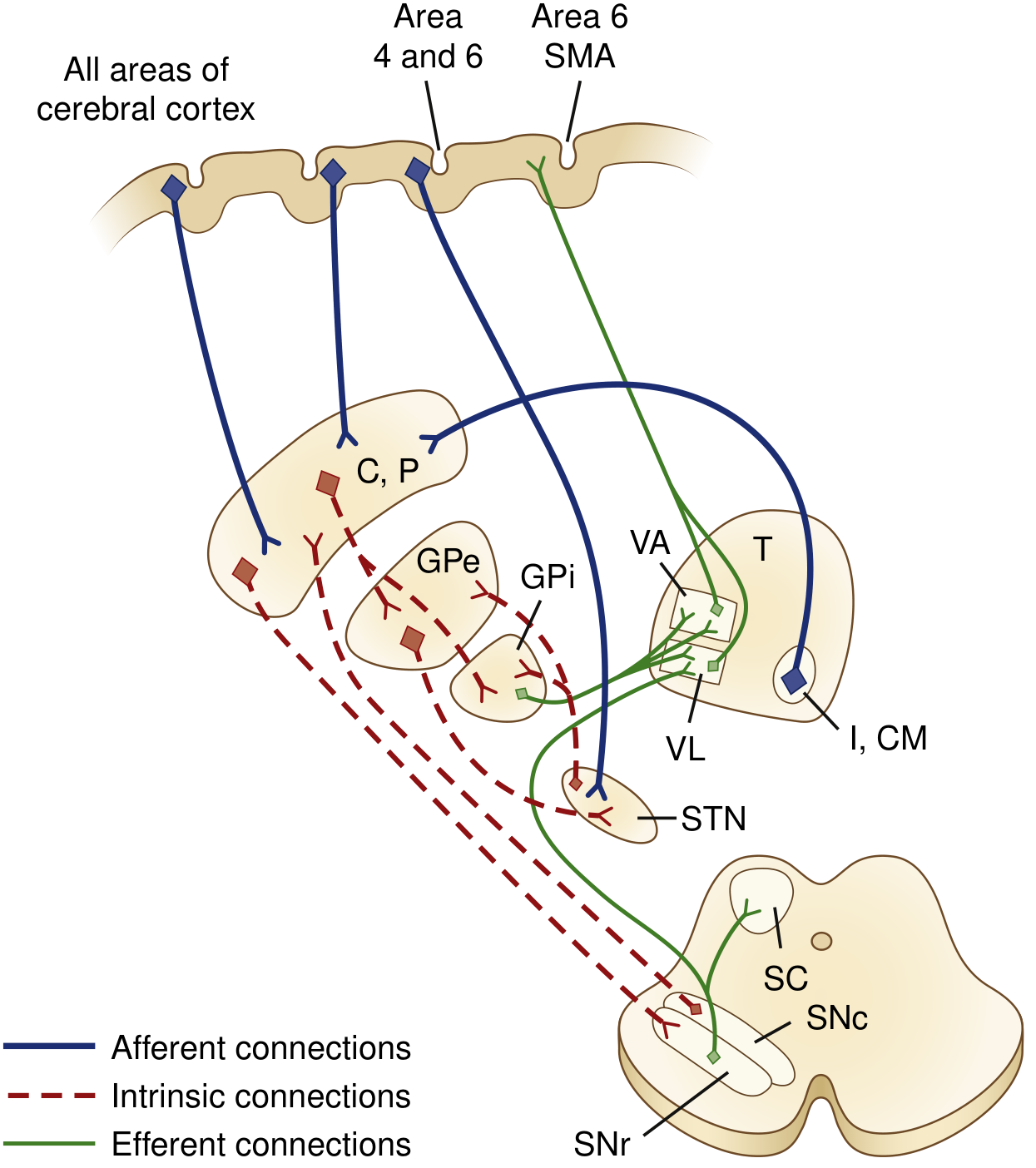
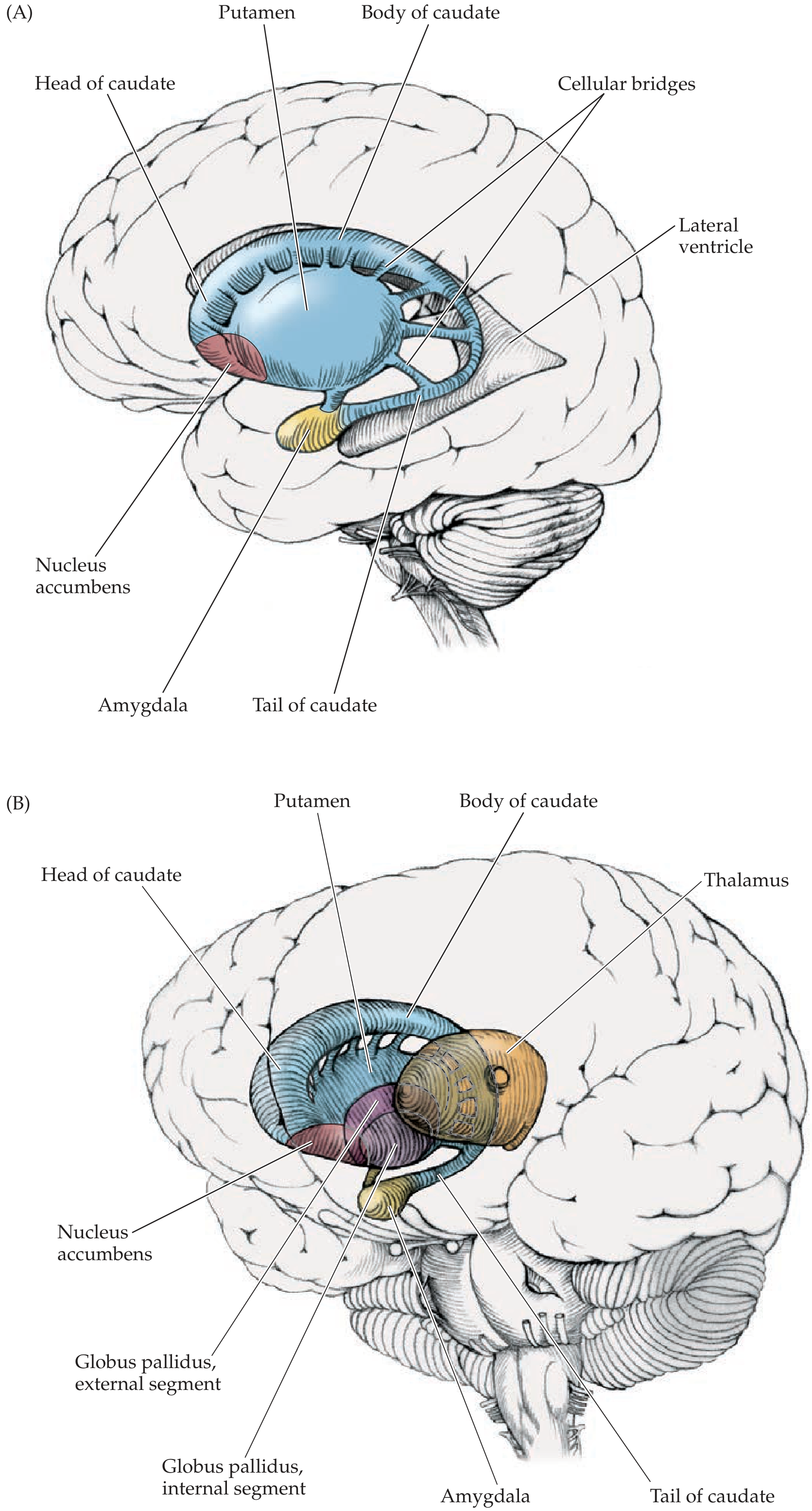
Here is your anatomy diagram showing the 3D positions:
Now let's meet each player:
Structure 1: The Striatum (= Caudate + Putamen)
What it is: The striatum is the MAIN ENTRANCE of the basal ganglia. Almost all information flowing into the basal ganglia from outside enters here. It is made of two structures that are basically the same tissue split apart by a bundle of nerve fibers (the internal capsule):
- Caudate nucleus - "Caudate" means "tail-bearing." It is a C-shaped structure that curves around the lateral ventricle (the fluid-filled space inside the brain), like a snake coiled around a pipe. It has a head, body, and tail.
- Putamen - Sits just lateral (to the side) of the globus pallidus. "Putamen" means "shell" in Latin.
Together, the caudate + putamen are called the striatum (from Latin "striped") because thin bridges of neurons connect them through the internal capsule, making them look striped in cross-section.
Analogy: If the basal ganglia were a company, the striatum is the front desk - all incoming messages (from the cortex) arrive here first.
What neurotransmitter does it use? The striatum sends its outputs using GABA (gamma-aminobutyric acid) - an inhibitory neurotransmitter. This means when striatal neurons fire, they suppress activity in wherever they project.
Quick definition - Inhibitory vs. Excitatory: Inhibitory signals tell the receiving neuron to slow down or stop firing. Excitatory signals tell it to fire more. This distinction is the single most important concept for understanding the whole basal ganglia circuit.
Functional divisions of the striatum:
| Region | Input from | Loop serves |
|---|
| Putamen | Motor cortex | Movement |
| Caudate head | Prefrontal cortex | Cognition, executive function |
| Ventral striatum (nucleus accumbens) | Limbic cortex, VTA | Reward, emotion, addiction |
Structure 2: The Globus Pallidus (GP)
Term - "Globus pallidus": Latin for "pale globe." It appears pale on brain sections because many myelinated fibers run through it.
The globus pallidus has two segments - think of them as two completely different employees who happen to share an office:
- Globus Pallidus externa (GPe) = the external or outer segment. This is an intrinsic relay station - it only talks to other parts within the basal ganglia.
- Globus Pallidus interna (GPi) = the internal or inner segment. This is one of the two main OUTPUT stations of the basal ganglia. It sends signals out of the basal ganglia to the thalamus.
Together, the putamen + globus pallidus = "Lenticular nucleus" (lentil-shaped). You'll see this term in anatomy and stroke descriptions.
Structure 3: The Subthalamic Nucleus (STN)
What it is: A small, lens-shaped cluster of neurons sitting at the junction between the cerebrum and the brainstem (hence "sub-thalamic" = below the thalamus).
What neurotransmitter does it use? Glutamate - excitatory. The STN is one of the few excitatory neurons within the basal ganglia circuit.
Why does it matter clinically? Because the STN is the target of deep brain stimulation (DBS) in Parkinson's disease, and because a lesion here causes hemiballismus (wild flinging movements). Both of those are high-yield exam facts.
Structure 4: The Substantia Nigra
Term - "Substantia nigra": Latin for "black substance." It literally appears black on gross brain sections because the dopamine-producing neurons in it contain neuromelanin, a dark pigment. If you look at a brainstem section and see a dark band, that's the substantia nigra.
It has two parts:
- Substantia nigra pars compacta (SNc) - the dopamine factory of the basal ganglia. These neurons synthesize dopamine and send it to the striatum via the nigrostriatal pathway. This is the part that degenerates in Parkinson's disease.
- Substantia nigra pars reticulata (SNr) - structurally and functionally identical to the GPi. It acts as a second OUTPUT station of the basal ganglia, particularly for eye movements (projects to superior colliculus).
Structure 5: The Nucleus Accumbens
The ventral (lower) part of the striatum. It is the brain's pleasure/reward center. It receives dopamine from the ventral tegmental area (VTA) via the mesolimbic pathway. Drugs of abuse (cocaine, heroin, alcohol) hijack this circuit by flooding it with dopamine.
The Thalamus (not technically "in" the BG, but essential to understand)
Term - "Thalamus": The brain's great relay station, sitting in the center. Almost all sensory and motor information passes through it on the way to the cortex.
The relevant thalamic nuclei for the basal ganglia are the VA (ventral anterior) and VL (ventrolateral) nuclei. They receive inhibitory GABA from GPi/SNr, and when allowed to escape that inhibition, they fire excitatory glutamate back to the motor cortex.
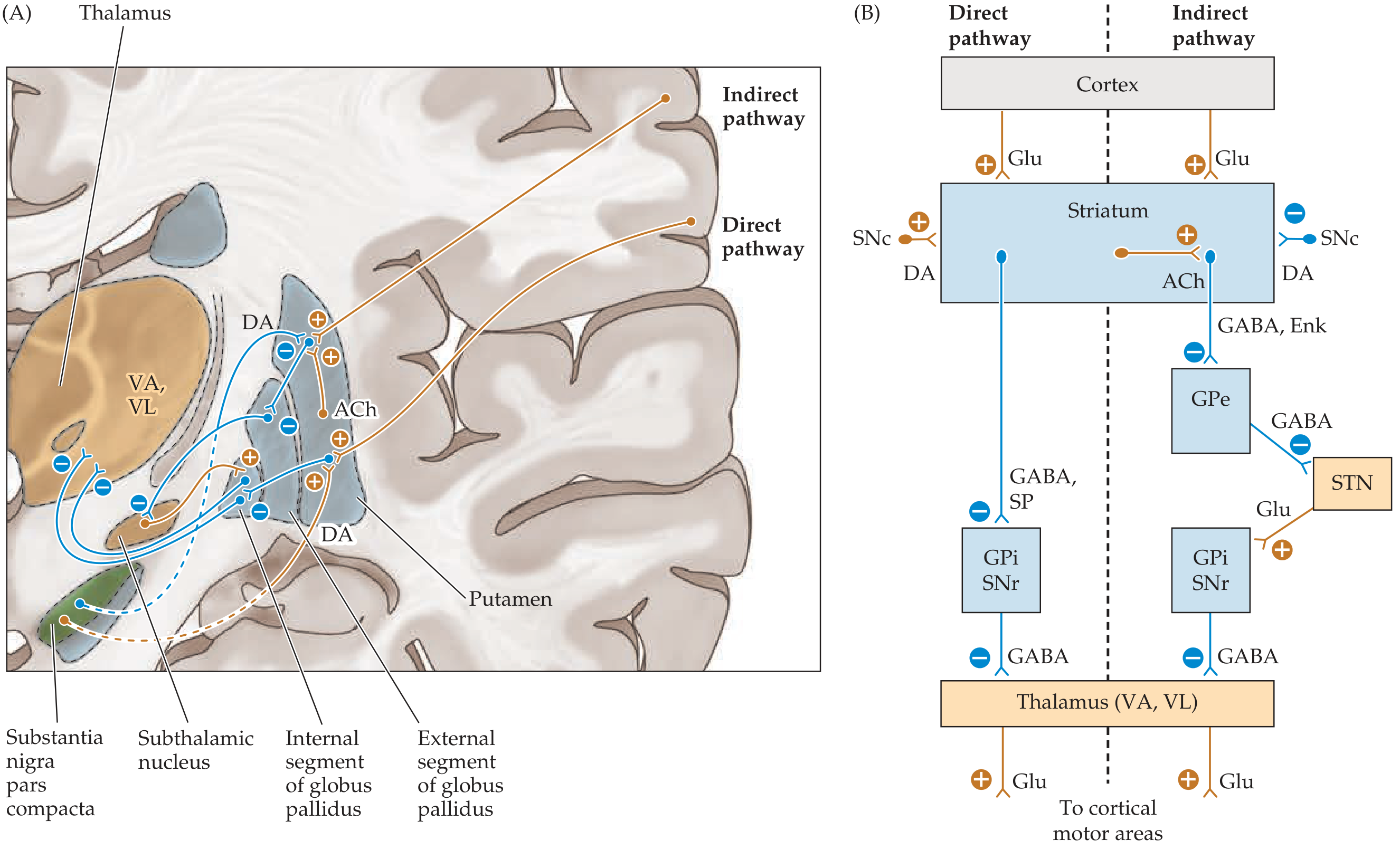
PART 3: THE CIRCUIT - How It All Connects
Here is the complete circuit diagram from your textbook:
The Overarching Logic: "Tonic Inhibition with Selective Release"
Here is the single most important concept in understanding the basal ganglia:
At baseline (at rest), the GPi/SNr fires CONSTANTLY and TONICALLY. This constant firing releases GABA onto the thalamus, keeping the thalamus suppressed - preventing unwanted movements.
When you want to make a voluntary movement, the basal ganglia must reduce this tonic inhibition - it must "let the thalamus off the leash" so it can activate the motor cortex.
Analogy: Imagine the thalamus is a dog that wants to run (= make a movement). The GPi/SNr is a leash constantly holding it back. The basal ganglia's job is to selectively loosen or tighten that leash at the right moment.
PART 4: THE TWO PATHWAYS IN DEPTH
There are two routes from the striatum to the GPi/SNr - the direct pathway (shortcut, excites movement) and the indirect pathway (detour, suppresses movement). They work like a gas pedal and a brake on the same car.
Pathway 1: The DIRECT Pathway - "The Gas Pedal" - Promotes Movement
Neurons involved: D1-receptor-bearing striatal neurons (they carry substance P and dynorphin alongside GABA)
Step-by-step, with cause-and-effect:
Step 1: The motor cortex fires glutamate (excitatory) → activates striatal neurons via D1 receptors
Step 2: Because the striatum is now active, it fires GABA (inhibitory) → directly onto GPi/SNr
Step 3: Because GPi/SNr is now inhibited, it fires LESS GABA onto the thalamus
Step 4: Because the thalamus is no longer being held back, it fires glutamate (excitatory) → activates motor cortex
Net result: MOVEMENT IS FACILITATED ✓
Using the math trick from textbooks: two inhibitory synapses in a row = net excitation. (-) × (-) = (+)
Cortex (+) → Striatum (-) → GPi/SNr (-) → Thalamus (+) → Cortex
Counting the signs: (+) × (-) × (-) × (+) = net POSITIVE = excitation of cortex = movement
Pathway 2: The INDIRECT Pathway - "The Brake" - Suppresses Movement
Neurons involved: D2-receptor-bearing striatal neurons (they carry enkephalin alongside GABA)
Step-by-step, with cause-and-effect:
Step 1: The motor cortex fires glutamate (excitatory) → activates striatal neurons via D2 receptors
Step 2: Because the striatum is now active, it fires GABA (inhibitory) → onto GPe
Step 3: Because GPe is now inhibited, it fires LESS GABA onto the STN (GPe's normal job is to inhibit STN)
Step 4: Because the STN is no longer being suppressed by GPe, it fires more glutamate (excitatory) → onto GPi/SNr
Step 5: Because GPi/SNr is now MORE active, it fires MORE GABA → onto the thalamus
Step 6: The thalamus is now MORE suppressed → less glutamate to motor cortex
Net result: MOVEMENT IS SUPPRESSED ✗
Cortex (+) → Striatum (-) → GPe (-) → STN (+) → GPi/SNr (-) → Thalamus (+) → Cortex
Counting: (+) × (-) × (-) × (+) × (-) × (+) = net NEGATIVE = inhibition of cortex = movement suppressed
Why Have Both Pathways?
Analogy: Think about focusing a spotlight on a stage. You need both:
- A bright light illuminating the target (direct pathway - activating the movement you want)
- Darkness around everything else (indirect pathway - suppressing all the other movements you DON'T want)
The basal ganglia use this combination to produce precise, focused movements while simultaneously suppressing competing motor programs. This is called "center-surround inhibition" - excite the desired movement, inhibit everything else.
PART 5: DOPAMINE - The Master Regulator
Now here is where it all comes together beautifully. The SNc sends dopamine to the striatum and modulates BOTH pathways at the same time - and the genius is that it affects them in opposite directions, but both changes result in more movement.
| Dopamine Effect | Receptor | Pathway | What Happens | Result |
|---|
| Dopamine → D1 receptor | D1 (Gs-coupled) | Direct pathway | Excites striatal neurons | ↑ Direct pathway → ↑ movement |
| Dopamine → D2 receptor | D2 (Gi-coupled) | Indirect pathway | Inhibits striatal neurons | ↓ Indirect pathway → ↑ movement |
Both effects push in the same direction: more dopamine = more movement.
Analogy: Dopamine is like a manager at work who both gives the "go" team a bonus (excites direct pathway) AND ties up the "stop" team in paperwork (inhibits indirect pathway). Either way, the end result is more work gets done (= more movement).
This is why losing dopamine (Parkinson's disease) causes decreased movement - you lose both the gas pedal AND lose the brake on the brake.
PART 6: PATHOPHYSIOLOGY - When Things Go Wrong
Now apply the circuit knowledge to diseases. This is where USMLE questions are born.
Disease 1: Parkinson's Disease
What is destroyed? SNc dopaminergic neurons. They degenerate, leaving dark empty spots in the substantia nigra (the "depigmentation" you see at autopsy - the black band becomes pale).
Why does this cause decreased movement?
Because dopamine is lost, the D1 receptors on direct pathway neurons don't get stimulated → direct pathway becomes underactive → GPi/SNr does not get inhibited properly → thalamus stays suppressed.
And at the same time: Because dopamine is lost, the D2 receptors on indirect pathway neurons don't get the inhibitory signal → indirect pathway becomes overactive → GPe gets over-inhibited → STN fires more → GPi/SNr gets over-excited → thalamus gets even MORE suppressed.
Therefore: Both the direct pathway failure AND the indirect pathway overactivity point to the same result - the thalamus cannot escape its inhibition, so the motor cortex cannot be activated properly.
Result: Bradykinesia (slow movement), akinesia (inability to initiate movement), rigidity, resting tremor.
Think of it as: the leash on the dog is pulled too tight from both ends.
↓ DA → ↓ Direct pathway → GPi/SNr over-fires
↓ DA → ↑ Indirect pathway → GPi/SNr over-fires
→ Thalamus chronically suppressed → ↓ cortical activation → HYPOKINESIA
Pathological hallmark: Lewy bodies - abnormal intracellular aggregates of alpha-synuclein protein inside surviving SNc neurons. On histology they appear as pink cytoplasmic inclusions with a pale halo.
Disease 2: Huntington's Disease
What is destroyed? Striatal neurons - specifically the indirect pathway neurons (D2, enkephalin-bearing) are lost FIRST. This is the key early-stage pathology.
Why does this cause INCREASED movement (chorea)?
Because indirect pathway striatal neurons are gone, GPe is no longer being inhibited → GPe becomes overactive → GPe over-inhibits STN → STN fires less → GPi/SNr gets less excitatory input → GPi/SNr fires less GABA → thalamus is no longer being held back → motor cortex is over-activated.
Therefore: Random, uncontrolled involuntary movements - chorea (from Greek "choros" = dance - writhing, dance-like movements).
↓ Striatal indirect neurons → GPe over-inhibits STN → ↓ STN → ↓ GPi/SNr → Thalamus unleashed → HYPERKINESIA
Think of it like: a lesion of the STN by another route. The net effect is the same - GPi/SNr is underactive, thalamus is unleashed.
Late stage of Huntington's: Eventually BOTH direct AND indirect pathway neurons die. When the direct pathway is also gone, the system loses all ability to activate movement. The patient becomes rigid and parkinsonian. This is why late-stage HD patients look like Parkinson's patients.
Genetics: Autosomal dominant, CAG trinucleotide repeat expansion in the huntingtin gene on chromosome 4p. Shows anticipation (repeat lengthens with each generation, disease worsens/earlier onset in children of affected parents).
MRI sign: Atrophy of the caudate nucleus head → loss of the normal caudate "bump" into the lateral ventricle → the lateral ventricle takes on a "box-car" shape (squared-off lateral ventricles).
Disease 3: Hemiballismus
What is destroyed/damaged? The subthalamic nucleus (STN) - usually from a contralateral lacunar infarct (small stroke), or in hyperglycemic states.
Why does this cause wild movements?
Because the STN is damaged, it cannot send its normal excitatory (glutamate) signal to the GPi/SNr → GPi/SNr fires less → thalamus is disinhibited → motor cortex is over-stimulated.
Therefore: Wild, large-amplitude, flinging (ballistic) movements of the contralateral proximal limbs.
Note: It's "hemi-" ballismus because only one STN is damaged → contralateral limb affected.
↓ STN (lesion) → ↓ GPi/SNr → ↑ Thalamus → ↑ Motor cortex → WILD FLINGING MOVEMENTS
PART 7: THE 5 PARALLEL LOOPS - Beyond Movement
The basal ganglia run five separate parallel channels, each using the same circuit logic but serving different functions:
| Loop | Striatal Region | Cortical Input | Output Back To | Function |
|---|
| Motor | Putamen | Primary motor + premotor cortex | Supplementary motor area | Voluntary movement |
| Oculomotor | Caudate body | Frontal eye fields | Frontal eye fields | Saccadic eye movements |
| Prefrontal | Caudate head (dorsal) | Dorsolateral prefrontal cortex | Prefrontal cortex | Executive function, working memory |
| Orbitofrontal | Caudate head (ventral) | Orbitofrontal cortex | Orbitofrontal cortex | Behavior, social judgment |
| Limbic | Nucleus accumbens | Limbic cortex, amygdala | Anterior cingulate | Emotion, motivation, reward |
Why this matters clinically:
- OCD = orbitofrontal-caudate circuit over-activity
- Depression in PD = limbic loop dopamine loss
- Cognitive decline in HD/PD = prefrontal loop involvement
- Drug addiction = limbic loop (nucleus accumbens) hijacked by drugs
PART 8: NEUROTRANSMITTER MAP
Every synapse in the basal ganglia uses either GABA (inhibitory), glutamate (excitatory), or dopamine (modulatory). Here it is organized:
| Connection | Neurotransmitter | Effect |
|---|
| Cortex → Striatum | Glutamate | Excitatory (+) |
| Cortex → STN | Glutamate | Excitatory (+) |
| Striatum → GPi (direct) | GABA + Substance P | Inhibitory (-) |
| Striatum → GPe (indirect) | GABA + Enkephalin | Inhibitory (-) |
| GPe → STN | GABA | Inhibitory (-) |
| STN → GPi/SNr | Glutamate | Excitatory (+) |
| GPi/SNr → Thalamus | GABA | Inhibitory (-) |
| Thalamus → Cortex | Glutamate | Excitatory (+) |
| SNc → Striatum (D1) | Dopamine | Excitatory (+) direct |
| SNc → Striatum (D2) | Dopamine | Inhibitory (-) indirect |
| Striatal interneurons | Acetylcholine | Excites indirect pathway |
PART 9: EXAM SECTION
HIGH-YIELD EXAM POINTS
- Striatum = INPUT nucleus. GPi + SNr = OUTPUT nuclei. Everything else is in between.
- Direct pathway = EXCITATORY net effect on motor cortex (promotes movement).
- Indirect pathway = INHIBITORY net effect on motor cortex (suppresses movement).
- Dopamine promotes movement via D1 (excites direct) AND D2 (inhibits indirect) - both push toward more movement.
- GPi/SNr fire TONICALLY at rest - this tonic GABA keeps the thalamus suppressed. Movement = releasing this brake.
- STN lesion → hemiballismus (contralateral). Cause: lacunar infarct, hyperosmolar hyperglycemia.
- SNc degeneration → Parkinson's (hypokinetic): TRAP - Tremor (resting), Rigidity, Akinesia/bradykinesia, Postural instability.
- Striatal indirect pathway neuron loss → Huntington's early (hyperkinetic/chorea). Late = both pathways → Parkinsonian.
- Huntington's genetics: AD, CAG repeat, chromosome 4p, anticipation, no cure. Tetrabenazine for chorea.
- Nucleus accumbens = reward, addiction (mesolimbic dopamine pathway from VTA).
- Basal ganglia disorders = contralateral symptoms (just like the corticospinal tract, the BG circuit is crossed).
- BG do NOT project to spinal cord. They modulate cortex via thalamus only.
- Carbidopa is given with L-DOPA to block peripheral decarboxylase (prevents L-DOPA from being converted to dopamine outside the brain before it crosses the BBB).
- Anticholinergics (trihexyphenidyl) help PD tremor by reducing ACh excitation of the overactive indirect pathway.
- Wilson's disease = copper in lenticular nucleus + liver (Chr 13, ATP7B). Low ceruloplasmin. Kayser-Fleischer rings.
COMMON MISCONCEPTIONS TO AVOID
Misconception 1: "Dopamine always inhibits"
- Wrong for basal ganglia. Dopamine EXCITES direct pathway (D1) and INHIBITS indirect pathway (D2). The net result of dopamine is pro-movement.
Misconception 2: "Huntington's is just a movement disorder"
- Wrong. Cognitive decline and psychiatric symptoms (depression, personality changes, psychosis) appear early and are often the presenting feature.
Misconception 3: "The basal ganglia control movement directly"
- Wrong. They never project to the spinal cord or muscles. They only modulate the motor cortex via the thalamus.
Misconception 4: "Parkinson's and Huntington's are opposites, so one is too much dopamine and the other is too little"
- Not exactly. Both can conceptually result in too little GPi/SNr inhibition (HD) or too much (PD), but the primary lesion in HD is striatal neuron loss, NOT a primary dopamine problem.
Misconception 5: "Late-stage Huntington's patients lose dopamine like Parkinson's"
- The Parkinsonian appearance in late HD is NOT from SNc degeneration. It is from loss of BOTH pathway striatal neurons, leading to GPi overactivity through a different mechanism.
Misconception 6: "The thalamus is part of the basal ganglia"
- The thalamus (VA/VL nuclei) is a relay station between the BG output and the cortex. It is not structurally part of the basal ganglia, even though it is part of the functional loop.
Misconception 7: "Hemiballismus is ipsilateral to the STN lesion"
- Wrong. Because the STN sends its output through GPi → thalamus → cortex → contralateral spinal cord, the movements are CONTRALATERAL to the STN lesion.
USMLE PEARLS - THE ONES THAT ACTUALLY SHOW UP
Pearl 1 - The "double negative" trick
When tracing the direct pathway, count how many inhibitory synapses: two minuses = plus (net excitation). For the indirect pathway: three minuses = minus (net inhibition). Never get confused by the pathway directions again.
Pearl 2 - Substance P vs. Enkephalin
- Direct pathway neurons co-express substance P (think "D for Direct, Dynorphin, D1")
- Indirect pathway neurons co-express enkephalin (think "E for Enkephalin, External GPe, D2")
A question may show histopathology of striatum with enkephalin-positive neuron loss → that's early Huntington's.
Pearl 3 - Hemiballismus in non-ketotic hyperglycemia
A diabetic patient with uncontrolled blood sugar who develops sudden unilateral flinging arm movements = hemiballismus from STN dysfunction due to metabolic derangement. T1 MRI shows hyperintensity in the basal ganglia/STN. This question appears regularly.
Pearl 4 - The DBS target
Deep brain stimulation in PD targets the STN (most common) or GPi. Why STN? Because in PD, the STN is overactive (because GPe cannot inhibit it due to overactive indirect pathway). Stimulating/inhibiting the STN reduces GPi overactivity → reduces thalamic suppression → improves movement.
Pearl 5 - Carbidopa mechanism
Carbidopa inhibits DOPA decarboxylase (= aromatic L-amino acid decarboxylase) in the periphery. It does NOT cross the BBB. Therefore it prevents peripheral conversion of L-DOPA to dopamine (which would cause nausea/hypotension) while allowing L-DOPA to cross the BBB and be converted centrally.
Pearl 6 - Tetrabenazine for Huntington's
Treats chorea by depleting vesicular monoamine stores (VMAT2 inhibitor) → less dopamine released in striatum. Side effects: depression (caution - HD patients already at high suicide risk), Parkinsonism.
Pearl 7 - Wilson's disease = lenticular nucleus + liver
"Lenticular" = putamen + globus pallidus. The copper depositing there causes movement disorder. Always check ceruloplasmin in young patients with movement disorder + liver disease + psychiatric symptoms.
Pearl 8 - The "boxcar" ventricles on MRI
When the caudate nucleus head atrophies in Huntington's disease, the normal convex bulge into the lateral ventricle disappears. The lateral ventricle loses its natural curvature and looks squared off (like a boxcar). This is a specific radiological sign of HD on MRI.
Pearl 9 - ACh in the striatum
Large aspiny (Tonically Active) interneurons in the striatum release ACh, which preferentially excites indirect pathway neurons. In PD, dopamine is lost BUT ACh is relatively preserved → ACh over-activates the indirect pathway. Anticholinergics (benztropine, trihexyphenidyl) restore the balance - particularly good for tremor (though NOT first-line in elderly due to cognitive side effects).
Pearl 10 - Anticipation in Huntington's
The CAG repeat in HD expands with each generation, especially when passed from the FATHER (paternal transmission causes more severe anticipation). Therefore, children of affected fathers tend to develop HD earlier and more severely than if the mother was the carrier.
Sources: Neuroanatomy through Clinical Cases 3e (Blumenfeld) | Costanzo Physiology 7e | Bradley & Daroff's Neurology in Clinical Practice