NSD IN DETAIL BASED ON WILLIAMS
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full, detailed answer on NSD based on Williams Obstetrics principles (as covered by Rosen's and standard textbook content).
Normal Spontaneous Delivery (NSD) - Based on Williams Obstetrics
Note: Williams Obstetrics is the canonical reference for NSD. The content below is drawn from Williams Obstetrics principles as reflected in Rosen's Emergency Medicine and Creasy & Resnik's Maternal-Fetal Medicine (both authoritative obstetric texts in the library), which extensively cite Williams.
Definition
Normal Spontaneous Delivery (NSD) is the vaginal delivery of a single, live, term fetus in vertex presentation without the aid of instruments (forceps or vacuum), and without operative intervention.
True Labor vs. False Labor
| Feature | True Labor | False Labor (Braxton Hicks) |
|---|---|---|
| Contractions | Regular, increasing in frequency & intensity | Irregular, do not escalate |
| Cervical change | Progressive effacement + dilation | No change |
| Pain location | Radiates from back to abdomen | Localized, variable |
| Effect of sedation | Not abolished | Usually abolished |
When in doubt, external electronic fetal monitoring (EFM) can confirm organized cyclic uterine contractions to rule out false labor.
The Stages of Labor
Stage 1 - Cervical Dilation
Divided into two phases:
Latent Phase:
- From onset of regular contractions to onset of active labor (approximately 6 cm dilation)
- Average duration: ~8 hours in nulliparous women, ~5 hours in multiparous women
- May be prolonged (>20 hours in nulliparas, >14 hours in multiparas)
Active Phase:
- From ~6 cm to full cervical dilation (10 cm)
- Faster rate of cervical change (Friedman's curve)
- Cervical dilation should progress at least 1 cm/hour in nulliparas, faster in multiparas
- Continuous external EFM throughout labor identifies fetal distress
Stage 2 - Expulsion (Delivery of the Fetus)
- Begins at full cervical dilation (10 cm) and ends with delivery of the baby
- Characterized by the urge to push/bear down with each contraction
- Median duration:
- Nulliparous: ~50 minutes
- Multiparous: ~20 minutes
- Prolonged second stage is associated with: postpartum hemorrhage, infection, severe vaginal lacerations
Stage 3 - Delivery of the Placenta
- From delivery of the baby to expulsion of the placenta
- Normally 5-30 minutes
- Active management (oxytocin + controlled cord traction) recommended
Stage 4 - The Immediate Postpartum Period
- First 1-2 hours after placental delivery
- Critical period for postpartum hemorrhage (PPH)
- Uterus must remain contracted; monitor vitals, blood loss, fundal height
Initial Assessment at Presentation
Key history and examination findings:
- Contraction frequency, duration, intensity
- Membrane status (ruptured or intact)
- Fetal movements
- Gestational age; last prenatal visit
- Gravida/para status
- Vaginal discharge or bleeding
- Urge to push (suggests advanced labor)
Vaginal Examination
Assess:
- Cervical dilation (0-10 cm)
- Effacement (percentage of cervical thinning)
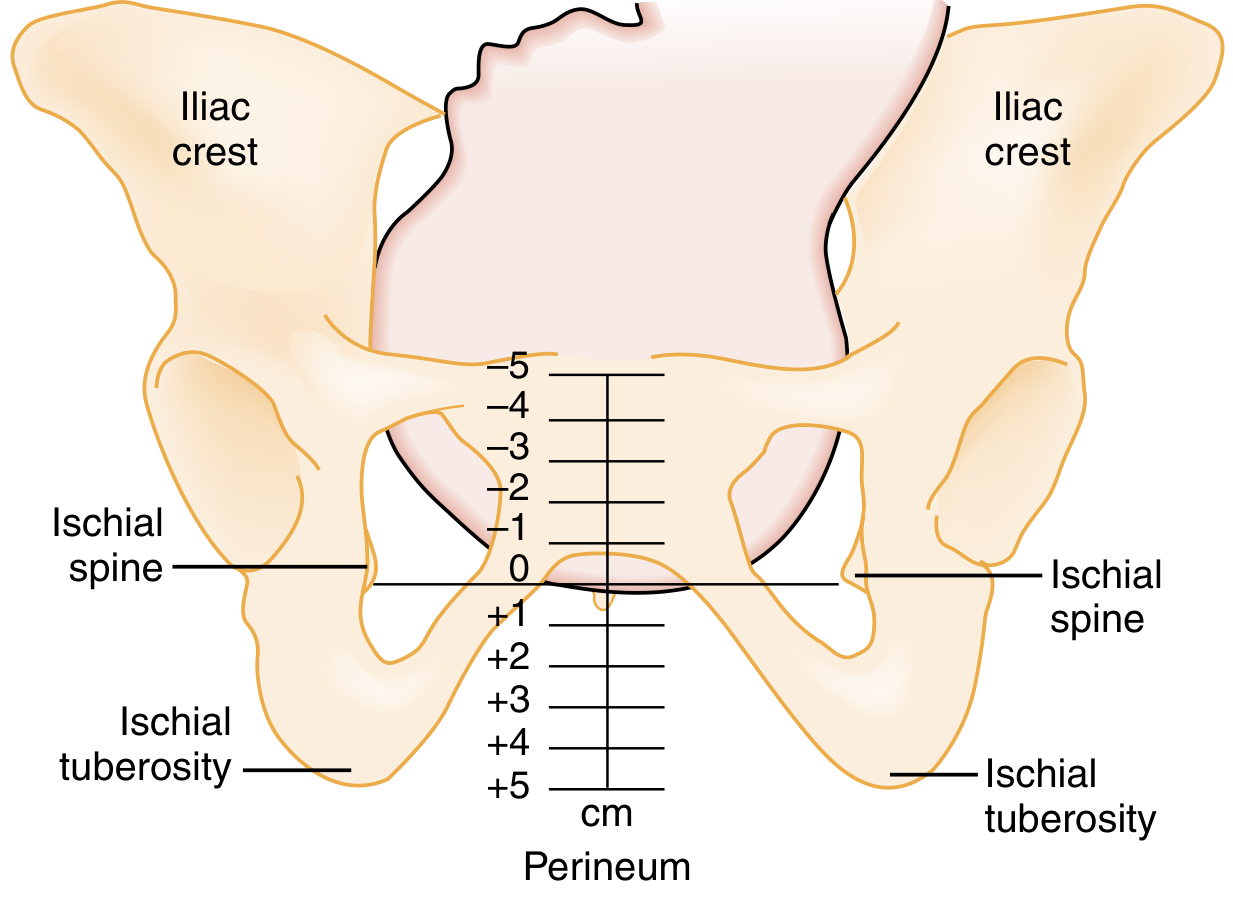
- Station (position of presenting part relative to ischial spines, -5 to +5)
- Presentation (vertex in 95% of labors)
- Position (occiput anterior, posterior, transverse)
- Membrane status
The ischial spines are at 0 station. Above is negative (-1 to -5); below is positive (+1 to +5). Crowning = presenting part visible at introitus.
If vaginal bleeding is present, defer digital examination until placenta previa is excluded by ultrasound.
Membrane Rupture Assessment
- Pooling of amniotic fluid in posterior fornix
- Ferning on microscope slide (sensitivity ~90%)
- Nitrazine paper turns blue (alkaline fluid, pH >6) - sensitivity ~90%
- False positives: blood, semen, cervical mucus, infection
Fetal Assessment During Labor
Electronic Fetal Monitoring (EFM)
Uterine activity: External pressure transducer records contraction frequency. Indirect measurement - correlates poorly with contraction strength.
Fetal Heart Rate (FHR) Components:
| Component | Normal | Significance |
|---|---|---|
| Baseline rate | 110-160 bpm | Average over 10-min period |
| Bradycardia | <110 bpm | Concerning - possible hypoxia |
| Tachycardia | >160 bpm | Hypoxia, infection, drugs |
| Variability | Present (beat-to-beat + long-term) | Indicator of fetal well-being |
| Accelerations | Present with fetal movement | Alert, mobile fetus |
Deceleration Patterns:
| Type | Timing | Cause | Significance |
|---|---|---|---|
| Early | Mirror contraction curve | Head compression (vagal) | Benign |
| Late | After peak of contraction (≥30 sec lag) | Uteroplacental insufficiency | Ominous |
| Variable | Abrupt onset, V-shaped | Cord compression | Concerning |
| Sinusoidal | Low baseline, minimal variability | Fetal hemorrhage, erythroblastosis, abruption | Pre-morbid/ominous |
Late decelerations with poor variability are the most dangerous combination. When fetal distress is identified, efforts to hasten delivery or emergency cesarean section should be instituted.
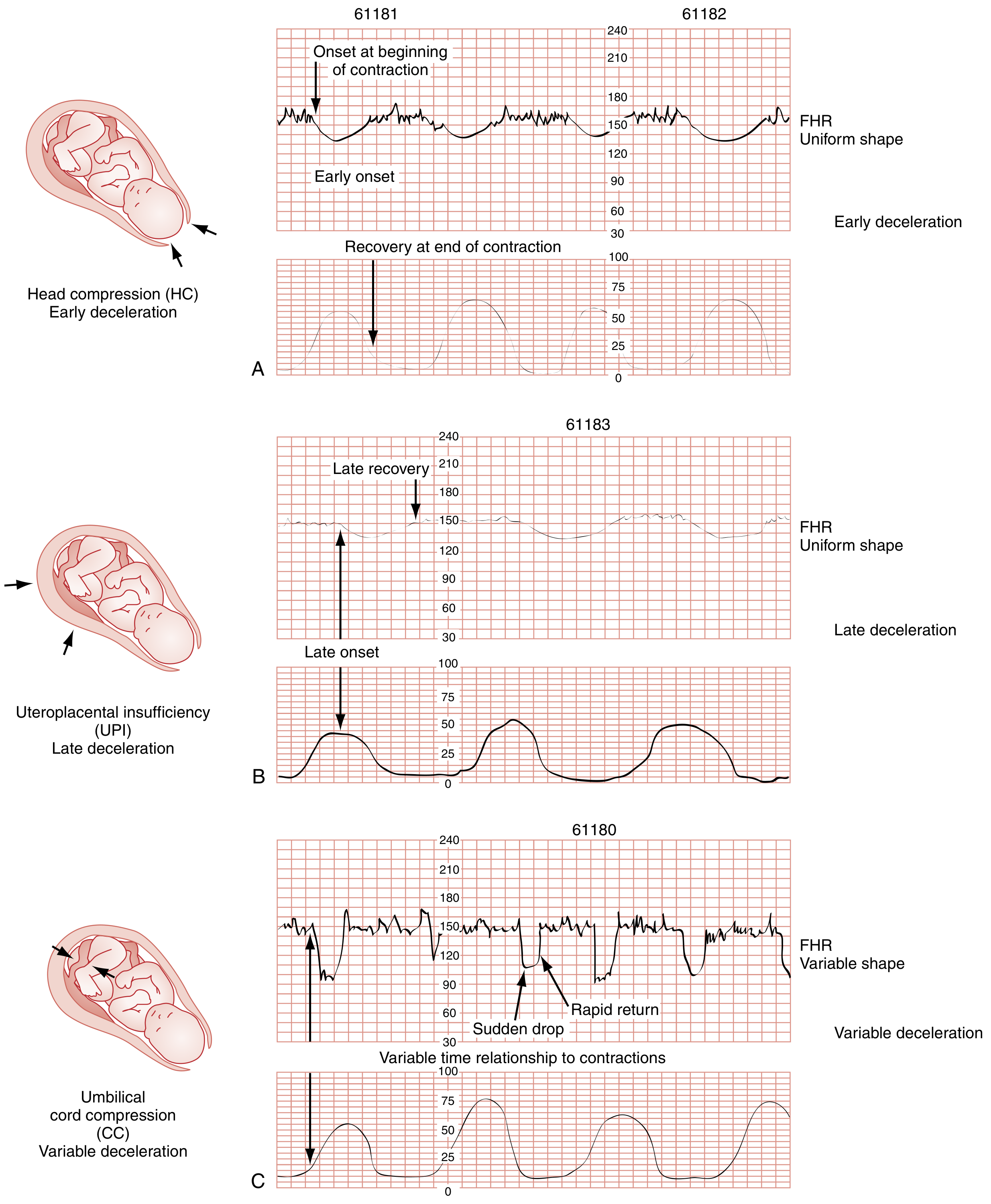
Fig: Deceleration patterns. (A) Early - head compression. (B) Late - uteroplacental insufficiency. (C) Variable - cord compression.
Ultrasonography in Labor
Provides: fetal viability, number of fetuses, lie, presentation, FHR, amniotic fluid index, placental location. Transvaginal US is relatively contraindicated with PROM or suspected placenta previa.
Obstetric Terminology
Lie
- Longitudinal: Long axis of fetus parallel to mother's spine (normal)
- Transverse: Perpendicular - cannot deliver vaginally
- Oblique: Intermediate
Presentation
- Vertex/cephalic (95%): Head presents first; occiput is the presenting part
- Breech (~3-4%): Buttocks/feet first
- Face, Brow, Shoulder: Abnormal - usually require intervention
Position
- Direction the occiput faces relative to maternal pelvis:
- Left Occiput Anterior (LOA): Most favorable for delivery
- Occiput Posterior (OP): May cause prolonged labor, more painful back labor
- Assessment: palpate fontanels - posterior fontanel has 3 suture lines; anterior fontanel has 4
Station
- Engagement = head at 0 station (at ischial spines)
- Crowning = head at perineum, visible at introitus without retraction between contractions
Leopold Maneuvers
Four-step systematic abdominal palpation to determine:
- First: What is in the fundus? (head = hard, ballottable; breech = soft, irregular)
- Second: Where is the fetal back? (smooth = back; irregular = extremities)
- Third: What is above the pelvic inlet? (presenting part)
- Fourth: Is the head flexed or deflexed? (cephalic prominence)

Cardinal Movements of Labor (Mechanisms of Labor)
In a vertex presentation, the fetus undergoes 7 cardinal movements to navigate the birth canal:
- Engagement - Biparietal diameter passes through pelvic inlet
- Descent - Progressive downward movement throughout labor
- Flexion - Head flexes, chin to chest (smallest diameter presents)
- Internal Rotation - Occiput rotates to lie under pubic symphysis (usually LOA → OA)
- Extension - Head extends as it passes under the pubic arch; face sweeps the perineum
- External Rotation (Restitution) - Head rotates back to align with fetal shoulders
- Expulsion - Delivery of shoulders (anterior first, then posterior) and body
Preparation for Delivery
Equipment to have ready:
- Radiant warmer, heated
- Towel, sterile scissors, umbilical clamps (x2)
- Bulb suction
- Airway equipment: oxygen, bag-mask device with appropriate-sized neonatal masks, ET intubation tools
- Vascular access equipment (IV)
- Oxytocin for third stage
Positioning:
- Dorsal lithotomy position (standard)
- Sims position (left lateral, knees drawn to chest, back to physician) - also acceptable, especially for precipitous delivery
Perineal preparation:
- Cleanse vulva and perineum with sterile water or saline
- Sterile examination to confirm presentation and labor progress
- Digital perineal stretching (especially posteriorly) may reduce tears and lacerations
Conducting the Delivery
Delivery of the Head
- Controlled, coordinated expulsion with maternal coaching ("push-push-push" with contractions, panting to slow passage)
- The most vulnerable moment is when the fetal head stretches and distends the perineum
- Instruct the mother to pant (not push) as the head crowns - slows passage, reduces lacerations
- Modified Ritgen Maneuver:
- Towel-draped, gloved hand placed posteriorly to support perineum and apply gentle upward pressure on fetal chin
- Second hand applies downward pressure on the occiput
- Guides head into slight extension so its smallest diameter (suboccipitobregmatic) passes through the pelvic outlet
- After head delivery: wipe nose and mouth; sweep any visible cord loops from around the neck
Check for Nuchal Cord
- After head delivery, check for cord around the neck
- If loose: slip over the head
- If tight: double-clamp and cut before delivery of body, or use somersault maneuver
Delivery of the Shoulders
- Gentle downward traction on the head to deliver the anterior shoulder under the pubic symphysis
- Gentle upward traction to deliver the posterior shoulder over the perineum
- Caution: excessive traction risks brachial plexus injury
Delivery of the Body
- Body and legs follow with gentle continuous traction
- Baby is delivered onto the mother's abdomen or into provider's hands
Episiotomy
- Surgical incision of the perineum to enlarge the vaginal opening
- Types: Median (midline) vs. Mediolateral
- Williams Obstetrics: Routine episiotomy is NOT recommended - evidence does not support its use for all deliveries
- Indications: fetal distress requiring urgent delivery, shoulder dystocia, operative delivery
- Median: easier to repair, less pain, but higher risk of extension to sphincter (3rd/4th degree tears)
- Mediolateral: more blood loss, harder to repair, but lower sphincter injury risk
Third Stage of Labor - Placental Delivery
Signs of Placental Separation:
- Gush of blood from vagina
- Lengthening of umbilical cord
- Uterus rises in abdomen and becomes globular and firm
- Fundus rises above umbilicus temporarily
Methods of Placental Delivery:
- Active management (WHO-recommended): Oxytocin 10 IU IM immediately after delivery of baby + controlled cord traction + uterine massage
- Reduces PPH risk by ~60%
Mechanisms:
- Schultze mechanism (~80%): Placenta separates centrally, presents shiny fetal surface first - usually less bleeding
- Duncan mechanism (~20%): Placenta separates peripherally, slides out sideways - more bleeding during separation
Retained Placenta:
- Defined as placenta not delivered within 30 minutes
- Requires manual removal
- Risk factors: accessory lobes, placenta accreta/increta/percreta
Immediate Neonatal Care
- Dry and stimulate the infant with a warm towel
- Suction mouth then nose with bulb syringe (if secretions present)
- Clamp and cut umbilical cord: first clamp ~3-4 cm from umbilicus, second clamp ~2 cm beyond; cut between them
- Delayed cord clamping (≥1 minute after birth): recommended by Williams/ACOG for term and preterm neonates - increases neonatal iron stores, reduces anemia
- Assign APGAR score at 1 minute and 5 minutes:
| Score | 0 | 1 | 2 |
|---|---|---|---|
| Appearance | Blue/pale all over | Blue extremities, pink body | Pink all over |
| Pulse | Absent | <100 bpm | ≥100 bpm |
| Grimace | No response | Grimace | Cry/cough/sneeze |
| Activity | Limp | Some flexion | Active motion |
| Respiration | Absent | Weak/irregular | Strong cry |
- Score 7-10: Normal
- Score 4-6: Moderate depression - stimulate, oxygen
- Score 0-3: Severe depression - full resuscitation
Fourth Stage - Immediate Postpartum (First 1-2 Hours)
The most critical period for postpartum hemorrhage (PPH):
- Normal blood loss: <500 mL vaginal delivery, <1000 mL cesarean
- PPH = blood loss >500 mL after vaginal delivery
Routine monitoring:
- Vital signs every 15 minutes for first hour
- Uterine fundus: firm, at or below umbilicus
- Uterine massage if uterus is boggy
- Inspect for perineal/vaginal lacerations and repair
- Bladder status (urinary retention common)
4 T's of PPH causes:
- Tone (uterine atony - most common, 70-80%)
- Tissue (retained placenta/clots)
- Trauma (lacerations, hematoma, uterine rupture)
- Thrombin (coagulopathy)
Perineal Lacerations (Obstetric Trauma)
| Degree | Structures Involved |
|---|---|
| 1st degree | Vaginal mucosa/fourchette only |
| 2nd degree | Perineal body muscles (not sphincter) |
| 3rd degree | External anal sphincter |
| 4th degree | Internal anal sphincter + rectal mucosa |
Repair begins once placenta is delivered and hemostasis is confirmed.
Complications to Know (Quick Reference)
| Complication | Key Feature | Management |
|---|---|---|
| Shoulder dystocia | Turtle sign after head delivery | McRoberts + suprapubic pressure; Rubin/Woods maneuvers |
| Umbilical cord prolapse | Cord precedes presenting part | Knee-chest/Trendelenburg; do NOT push; emergency C-section |
| Postpartum hemorrhage | >500 mL blood loss | Oxytocin, bimanual compression, transfusion |
| Uterine inversion | Fundus inverts into vagina | Manual replacement before oxytocin |
| Amniotic fluid embolism | Sudden collapse + DIC in labor | Supportive, ICU, FFP/platelets |
Summary: Key Williams Obstetrics Numbers
| Parameter | Value |
|---|---|
| Term gestation | 37-41+6 weeks |
| First stage (nullipara) | ~8 hours average |
| First stage (multipara) | ~5 hours average |
| Second stage (nullipara) | ~50 min median |
| Second stage (multipara) | ~20 min median |
| Third stage | 5-30 minutes |
| Fetal bradycardia | <110 bpm |
| Fetal tachycardia | >160 bpm |
| Normal FHR | 110-160 bpm |
| Engagement station | 0 (at ischial spines) |
| APGAR normal | 7-10 |
| PPH definition (vaginal) | >500 mL blood loss |
Sources: Rosen's Emergency Medicine (9th ed.) - Chapter 176: Labor and Delivery; Creasy & Resnik's Maternal-Fetal Medicine (8th ed.); Williams Obstetrics principles as cited throughout both texts.
This is a shared conversation. Sign in to Orris to start your own chat.