my professor asked me to study about solitary pulmonary nodule - from its past to its future .. everything. i have a case in my ward and i must present this topic tomorrow .. it will be like a rapid fire in a round table conference. explain everything to me in detail so that i can answer stuff even before a queation comes out of their mouths.. make me so knowledgable that i ask questions to which my professors would answer taht theyll stufy about it
Reading File
Finding Sources
Finding Sources
Searching PubMed
"solitary pulmonary nodule" management guidelines
Searching the Web
solitary pulmonary nodule Fleischner Society 2017 guidelines management complete review
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed. Let me compile the master reference guide.
SOLITARY PULMONARY NODULE (SPN) - The Complete Master Guide
Sources: Harrison's 22e (2025), Fishman's Pulmonary Diseases, Murray & Nadel's Respiratory Medicine, Goldman-Cecil Medicine, Schwartz's Surgery, Fleischner Society 2017, ACR 2026, AATS 2024
1. DEFINITION - GET THIS EXACT
A solitary pulmonary nodule (SPN) is:
- A single, round or oval radiographic opacity in the lung parenchyma
- ≤3 cm in diameter (lesions >3 cm are called "pulmonary masses" and carry a much higher malignancy risk)
- Completely surrounded by normal aerated lung
- No associated mediastinal adenopathy, atelectasis, or pleural effusion
Professor-level nuance: The word "solitary" was coined in the CXR era. With CT, up to 50% of what appears solitary on CXR actually has companion sub-centimeter nodules. The term "solitary" strictly requires CT confirmation. In the Early Lung Cancer Action project, ~7% of healthy volunteers had 1-3 nodules, and 25% had up to 6. So always say "as evaluated by CT."
2. HISTORICAL EVOLUTION - "THE PAST"
The "Coin Lesion" Era (1940s-1960s)
- The SPN was originally called a "coin lesion" when first described on plain CXR
- Initial case series showed high malignancy rates (up to 40%) among resected nodules - but these were surgical series bias (only the suspicious ones got operated)
- Most pre-CT nodules were >10 mm and "presumed cancer until proven otherwise," leading to massive over-surgery of benign lesions
- The link between smoking and lung cancer in the mid-1960s sparked the first screening programs with CXR
CT Revolution (1980s)
- Chest CT in the 1980s became widespread and "accidentally launched an epidemic of incidental findings" - Fishman's
- CT use increased ~8% per year between 1996-2010; by 2008 there were 23 chest CTs per 1000 enrollees per year
- One landmark study: in >28% of diagnostic chest CTs, at least one nodule measuring 4-30 mm was found
- This meant clinicians suddenly had millions of small nodules they had no framework to handle
NLST and Screening Era (2000s-2010s)
- The National Lung Screening Trial (NLST) proved low-dose CT (LDCT) reduces lung cancer mortality
- It simultaneously created the "nodule epidemic" - on baseline screening, 20-50% of subjects had at least one nodule
- But only 3-12% of screen-detected nodules on the first round were malignant - 90-95% were false positives
- This created massive anxiety, unnecessary procedures, and drove the creation of formal management guidelines
In the US: ~1 million new SPNs detected per year currently
3. EPIDEMIOLOGY & SIGNIFICANCE
| Fact | Number |
|---|---|
| SPNs detected/year in the US | ~1 million |
| That are malignant | ~40-50% (in symptomatic/high-risk populations) |
| Malignant SPNs - adenocarcinoma | 47% |
| Malignant SPNs - squamous cell | 22% |
| Malignant SPNs - small cell | 4% |
| Benign SPNs - infectious granulomas | ~80% of all benign |
| Cancer risk, nodule <6 mm | <1% |
| Cancer risk, nodule 6-8 mm | 1-2% |
In regions with endemic granulomatous disease (TB, histoplasmosis, coccidioidomycosis), malignancy rates are much lower - one Illinois study found only 16% malignancy, with 75% being granulomas mostly from histoplasmosis.
4. CLASSIFICATION BY DENSITY (CT Attenuation) - CRITICAL
This is the modern CT-based framework that drives ALL management:
A. Solid Nodule
- Completely masks underlying lung parenchyma
- Classic presentation; most common type
- Management follows size-based Fleischner criteria
B. Ground-Glass Opacity/Nodule (GGO/GGN) - Nonsolid
- Hazy increased attenuation that does NOT obscure underlying bronchi/vessels
- Lung parenchyma still visible through it
- More likely to be indolent - longer volume doubling times
- Histologic spectrum: Atypical Adenomatous Hyperplasia (AAH) → Adenocarcinoma in Situ (AIS) → Minimally Invasive Adenocarcinoma (MIA) → Invasive Adenocarcinoma
- AAH: usually <5 mm, minimally hazy
- AIS: slightly more opaque than AAH, typically nonsolid on thin-section CT
- MIA: mainly solid with a small (<5 mm) central solid component
C. Part-Solid (Semisolid) Nodule
- Both ground-glass AND solid components
- Solid component represents the invasive portion
- HIGHEST risk of malignancy among all three types
- 40-50% of part-solid subcentimeter lesions are malignant vs. only 15% of subcentimeter solid or nonsolid nodules
- Management driven by the SIZE OF THE SOLID COMPONENT
Pearl for professors: Ask them - "If I find a 12 mm part-solid nodule with a 4 mm solid component and a 12 mm part-solid nodule with an 8 mm solid component - are they managed the same?" Answer: No. The solid component size drives the management algorithm.
5. DIFFERENTIAL DIAGNOSIS - BROAD BUT SYSTEMATIC
Malignant Causes
- Primary lung cancer (most important - adenocarcinoma > squamous > small cell > large cell)
- Carcinoid tumor (typical and atypical; often central, highly vascular)
- Pulmonary metastasis from: breast, colon, kidney, melanoma, sarcoma, germ cell tumors
Key point: A new single pulmonary nodule in a patient with prior malignancy. Likelihood of it being a NEW primary lung cancer (not metastasis) is highest with prior: uterine (74%), bladder (89%), lung (92%), and head & neck (94%) carcinomas.
Benign Causes
Infectious Granulomas (80% of benign):
- Tuberculosis
- Histoplasmosis (endemic - Ohio/Mississippi valley)
- Coccidioidomycosis (endemic - American Southwest)
- Dirofilariasis (dog heartworm - underdiagnosed!)
- Mycetoma, Echinococcal cyst, Ascariasis
Non-infectious Granulomas:
- Sarcoidosis (not always accompanied by hilar adenopathy)
- Rheumatoid arthritis (necrobiotic nodules - can coexist with subcutaneous nodules)
- Granulomatosis with Polyangiitis/GPA (Wegener's) - often cavitary, multiple, ± renal/sinus disease
- Inflammatory Bowel Disease
Other Benign:
- Pulmonary hamartoma (2nd most common single benign cause, ~10%) - "popcorn" calcification, fat density (-40 to -120 HU), diagnostic on CT in ~50%
- Rounded pneumonia
- Pseudotumor (fluid in interlobar fissure - disappears with diuresis!)
- AVM (arteriovenous malformation)
- Pulmonary sequestration
- Intrapulmonary lymph node (perifissural location, lentiform shape)
- Inflammatory myofibroblastic tumor
6. RADIOLOGY - THE CORE SKILL
CXR First, Then CT
The CXR below shows a classic coin lesion (left hilar area, ~1 cm nodule):
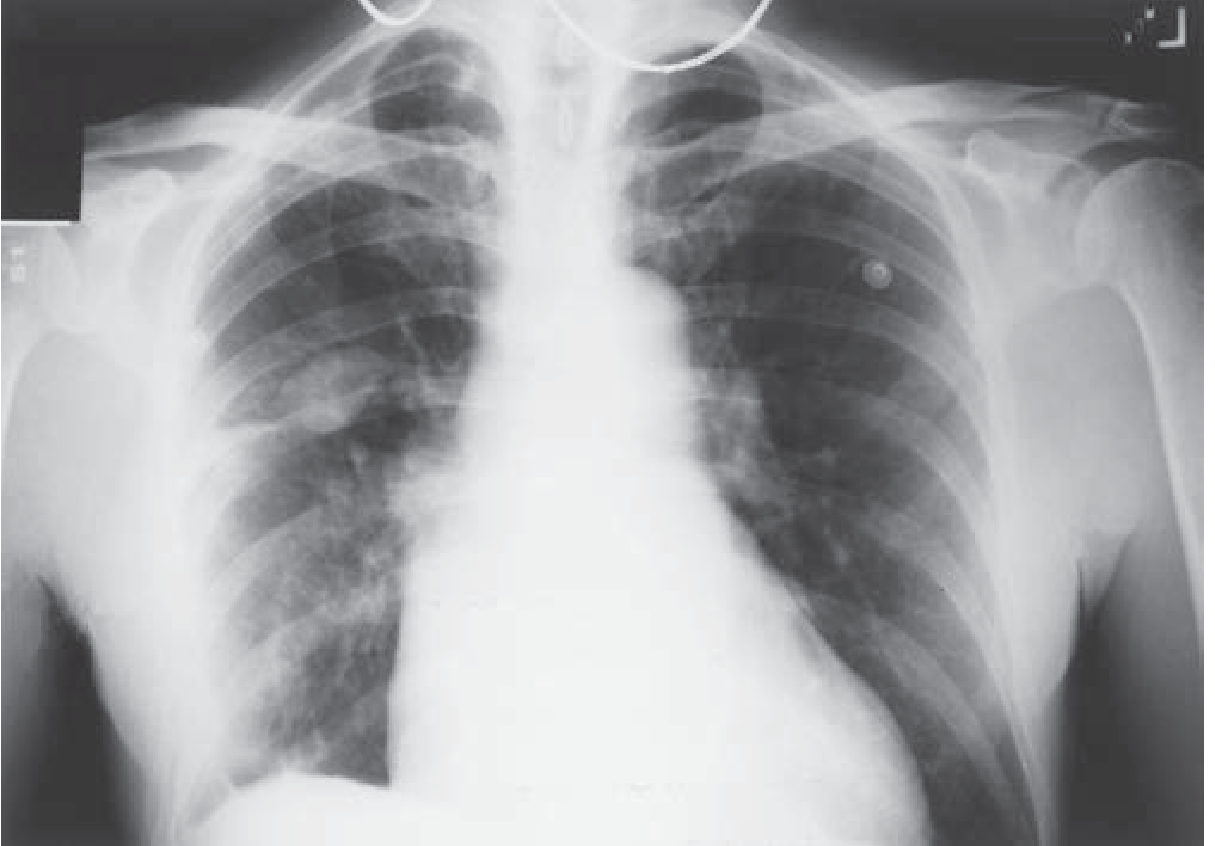
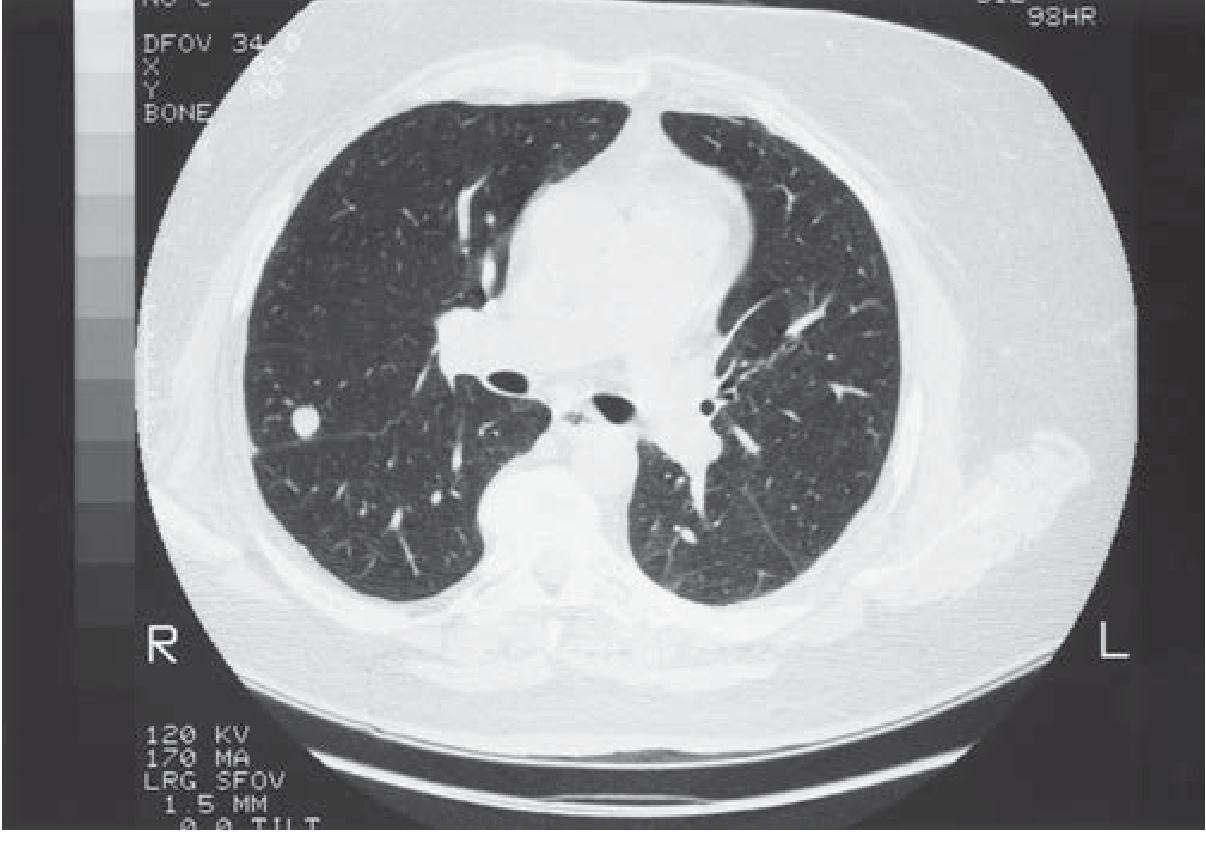
CT (1.5 mm thin sections) is the gold standard for:
- Size, shape, density
- Calcification pattern
- Margin characteristics
- Fat content
- Satellite nodules
- Number/location
CT Characteristics: BENIGN vs. MALIGNANT
Features suggesting BENIGN:
| Sign | Details |
|---|---|
| Calcification - diffuse/central | Granuloma pattern |
| Calcification - laminated/"onion ring" | Granuloma (TB) |
| Calcification - "popcorn" | Hamartoma (pathognomonic) |
| Calcification - "bull's eye" | Granuloma (histoplasmosis) |
| Fat attenuation (-40 to -120 HU) | Hamartoma |
| Smooth, well-defined margins | Lower risk (but not zero) |
| Stability over 2 years | Most reliable sign of benignity |
| Perifissural location, lentiform shape | Intrapulmonary lymph node |
Only 2 criteria definitively predict benignity: (1) no growth for >2 years, and (2) benign calcification pattern. - Harrison's 22e
Features suggesting MALIGNANT:
| Sign | Details |
|---|---|
| Spiculation | "Corona radiata" - fine linear strands radiating 4-5 mm outward |
| Lobulated/irregular margins | Higher risk |
| Size >3 cm | Mass = almost certainly malignant |
| Upper lobe location | Higher risk |
| Growth on serial imaging | Volume doubling time 20-400 days for lung cancer |
| Eccentric/stippled/amorphous calcification | Cancer with dystrophic calcification |
| Air bronchograms within nodule | Common in adenocarcinoma |
| Pleural tethering/"tail" | Non-specific (once thought malignant - this has changed!) |
| Internal cystic lucency/pseudocavitation | Part-solid adenocarcinoma |
Professor-level nuance on pleural tail: Once thought to suggest malignancy, it is now recognized as a non-specific finding that can be seen in both benign and malignant nodules. Murray & Nadel explicitly states this.
Eccentric calcification: This does NOT mean benign - cancer can engulf a pre-existing calcified granuloma and show eccentric/stippled calcium. This is one of the most common exam traps.
Volume Doubling Time (VDT)
- Lung cancers: VDT = 20 to 400 days
- VDT <20 days = infection (too fast for cancer)
- VDT >400 days = suggests benign, but can still be slow-growing cancer (especially GGO-type adenocarcinomas!)
- 2D diameter underestimates growth; volumetric analysis (3D) is more accurate and is preferred in BTS guidelines
7. PROBABILITY OF MALIGNANCY - RISK MODELS
Clinical Risk Factors (Independent Predictors - Mayo Clinic Model)
The landmark Mayo Clinic study identified these independent predictors of malignancy:
- Older age
- Cigarette smoking history
- Prior cancer diagnosis (especially >5 years before)
- Nodule diameter (larger = more likely malignant)
- Spiculation on CT
- Upper lobe location
Smokers: 50%+ malignancy probability
Never smokers: 20-40% malignancy probability
Risk Stratification Categories
- Low probability: <5% chance of malignancy
- Moderate probability: 5-65%
- High probability: >65%
The Brock Model (also called "PanCan model" from the Pan-Canadian Early Detection Study): Includes nodule type (solid vs. sub-solid), family history of lung cancer, nodule count. This is used in BTS and BCCA guidelines. Good question to ask professors: "Does the Mayo model or the Brock model incorporate sub-solid nodule characteristics?" - Brock does, Mayo doesn't (it predates modern CT classification).
8. DIAGNOSTIC WORKUP - STEP BY STEP
Step 1: Get old films
Always compare with prior CXR or CT. Stability for 2 years = benign. Growth = act.
Step 2: CT Characterization
High-resolution thin-section CT (1-2 mm collimation):
- Nodule size, density, margins, calcification
- Look for satellite nodules, lymphadenopathy
- Contrast enhancement: benign nodules enhance <15 HU; most malignant nodules enhance >20 HU (contrast CT enhancement study - less commonly used now)
Step 3: FDG-PET / PET-CT
Indications: Solid nodules ≥8 mm where CT is indeterminate
Performance of FDG-PET:
- Sensitivity: 87-97%
- Specificity: 78-82%
- PPV: ~91%
- NPV: ~90%
SUV cutoff: SUVmax >2.5 = malignant (traditional), but visual analysis comparing to mediastinal blood pool is equally valid
False Negatives (cancer that is PET-negative):
- Adenocarcinoma in situ / minimally invasive adenocarcinoma
- Mucinous adenocarcinoma
- Carcinoid tumors (low metabolic activity)
- Nodules <8 mm (spatial resolution limit)
- Hyperglycemia (competes with FDG)
False Positives (benign that is PET-positive):
- Active TB granuloma
- Histoplasmosis
- Aspergillosis
- Sarcoidosis
- Rheumatoid nodules
PET in GGOs: Essentially useless - sensitivity only 10%, specificity 20% for ground-glass nodules. Use thin-section CT for GGOs instead.
Step 4: Tissue Sampling Options
1. CT-guided Transthoracic Needle Biopsy (TTNB)
- Best for peripheral nodules, >1 cm
- Sensitivity 80-95%
- Complication: pneumothorax (10-30%; ~5% require chest tube)
- Non-diagnostic result does NOT exclude malignancy
2. Bronchoscopy (Flexible)
- Best for central/endobronchial lesions
- Sensitivity for peripheral nodules is low (~20-30% for <2 cm nodules) with conventional bronchoscopy
- Endobronchial Ultrasound (EBUS): For nodules with airway proximity
- Electromagnetic navigation bronchoscopy (ENB): Newer modality for peripheral nodules, improves yield to ~60-80%
- Robotic bronchoscopy (e.g., Monarch, Ion systems): Cutting edge; navigates to peripheral nodules
3. VATS (Video-Assisted Thoracoscopic Surgery)
- Diagnostic AND therapeutic in one procedure
- For nodules with high probability of malignancy (>65%) OR indeterminate after all non-invasive workup
- If nodule is too deep for VATS, CT-guided hookwire localization or dye injection can mark the target preoperatively
4. Bronchoscopic Cryobiopsy - Emerging technique, higher yield than conventional BAL
9. MANAGEMENT GUIDELINES - THE FLEISCHNER SOCIETY 2017 (Gold Standard)
The Fleischner Society is the international multidisciplinary gold standard. These apply to incidentally detected nodules in adults >35 years. They do NOT apply to lung cancer screening programs (that uses Lung-RADS).
Solid Nodules
| Size | Low Risk | High Risk |
|---|---|---|
| <6 mm (<100 mm³) | No routine follow-up | Optional CT at 12 months |
| 6-8 mm (100-250 mm³) | CT at 6-12 months, then consider CT at 18-24 months | CT at 6-12 months, then CT at 18-24 months |
| >8 mm (>250 mm³) | Consider CT, PET/CT, or tissue sampling at 3 months | Consider CT, PET/CT, or tissue sampling at 3 months |
Low risk: No smoking history, no known malignancy, young age
High risk: Smoking, family history of lung cancer, occupational exposure, upper lobe location, suspicious morphology
Major change from previous Fleischner: The 2017 version raised the no-follow-up threshold from 4 mm to 6 mm in low-risk patients. This eliminates thousands of unnecessary follow-up scans per year. Rationale: Cancer risk in nodules <6 mm is considerably less than 1% even in high-risk patients.
Subsolid Nodules (2017 Fleischner)
| Type | Size | Management |
|---|---|---|
| Pure GGO | <6 mm | No follow-up |
| Pure GGO | ≥6 mm | CT at 6-12 months; if stable, CT at 2 and 4 years |
| Part-solid | <6 mm total | No follow-up |
| Part-solid | ≥6 mm total | CT at 3-6 months; if stable and solid component remains <6 mm, annual CT for 5 years |
| Part-solid with solid component ≥6 mm | Any | High suspicion - PET/CT, biopsy, or resection |
Why 5-year follow-up for GGOs? Because subsolid nodules grow MUCH more slowly. Volume doubling times can be years, not months. A GGO that appears stable at 2 years can still become invasive cancer years later. This is the biology of the AAH → AIS → MIA → invasive adenocarcinoma spectrum. They essentially start as non-malignant cells that transform over years.
Lung-RADS (ACR) - for Screening Programs
| Category | Finding | Cancer Risk | Action |
|---|---|---|---|
| 1 | Negative / benign calcification | <1% | Annual screening |
| 2 | Small nodule (<6 mm solid, <30 mm GGO) | <1% | Annual screening |
| 3 | Probable benign | 1-2% | 6-month CT |
| 4A | Suspicious | 5-15% | 3-month CT |
| 4B | Highly suspicious | >15% | Chest CT + PET/CT and/or tissue sampling |
10. WHAT HAPPENS WHEN TISSUE IS NEEDED - SURGERY
For nodules requiring surgical resection:
- Lobectomy is the standard of care for resectable lung cancer
- VATS lobectomy has largely replaced open thoracotomy for most cases
- Wedge resection/segmentectomy: For small peripheral nodules or patients with poor pulmonary reserve
- Anatomic resection (lobectomy) has better local control and survival than wedge resection for invasive cancers
For metastatic disease to lung (solitary metastasis):
- Pulmonary metastasectomy - the IRLM (International Registry of Lung Metastases) data: 5-year survival after complete resection is 36% for all tumor types
- Best outcomes: germ cell tumors, disease-free interval >36 months, single metastasis
11. THE FUTURE - WHERE SPN MANAGEMENT IS HEADING
1. Artificial Intelligence and Deep Learning
- AI algorithms now achieve radiologist-level performance in nodule detection and characterization
- Deep learning models can predict malignancy risk from CT features alone with AUC >0.95
- Multi-institutional AI validation studies are ongoing
- Future: AI-integrated reporting that auto-classifies every nodule and generates a follow-up plan
2. Liquid Biopsy
- Circulating tumor DNA (ctDNA) and cell-free DNA can potentially be detected even for small cancers
- GRAIL Galleri test and similar assays detect multi-cancer early detection signals from a blood draw
- Currently insufficient sensitivity for sub-cm nodules, but improving rapidly
- Could replace some invasive tissue sampling for risk stratification
3. Proteomics and Biomarker Panels
- MiR-Test (microRNA panel) and Nodify XL2 (plasma protein panel) are commercially available in some markets
- Nodify XL2 (LG3BP + C163A) combined with clinical/CT data: when test indicates low risk (<50% pretest probability), can safely defer invasive testing
- Useful when the pretest probability is intermediate (5-65%) - can reclassify to low or high, guiding whether to biopsy
4. Radiomics
- Extraction of hundreds of quantitative features from CT images (texture, entropy, heterogeneity, wavelets)
- Combined with machine learning to predict malignancy, histology, and mutation status (e.g., EGFR, KRAS)
- Can potentially non-invasively predict molecular subtypes guiding targeted therapy decisions
5. Robotic Bronchoscopy
- Systems like the Monarch (J&J) and Ion (Intuitive) platforms enable ultra-peripheral nodule access
- Can reach 6th-generation bronchi for biopsy
- Real-time imaging guidance, reduced need for CT-guided TTNB
6. Lung Cancer Screening Expansion
- Current USPSTF criteria: 50-80 years old, 20 pack-year history
- 2025 European Society of Thoracic Imaging published updated recommendations for LDCT screening result classification
- Global debate: Should never-smokers with other risk factors (radon, occupational, genetics) also be screened?
- Integration of polygenic risk scores into nodule management is an active research frontier
7. SBRT/SABR for High-Risk Non-Surgical Candidates
- Stereotactic Body Radiotherapy (SBRT) / Stereotactic Ablative Radiotherapy (SABR): for patients with malignant-appearing nodules who cannot tolerate surgery
- Local control rates >90% for Stage I NSCLC
- This means "too sick to operate" is no longer "too sick to treat"
12. SPECIAL POPULATIONS AND TRAPS
Prior Malignancy
- Always biopsy rather than assume metastasis vs. new primary
- Metastatic lesions: classically smooth, multiple, bilateral, lower lobe predominance (blood flow distribution), temporal proximity to primary
- Single lesion in prior malignancy: high chance of new primary, especially with head/neck, lung, uterine, bladder primaries
Immunocompromised Patients
- Higher rate of infectious causes: cryptococcosis, aspergillosis, nocardia
- Septic emboli can present as multiple nodules (NOT technically SPN, but differential)
- Post-transplant lymphoproliferative disease (PTLD) must be considered
Young Patient / Non-smoker
- Probability of malignancy is much lower - granuloma, hamartoma, carcinoid are more likely
- Carcinoid tumors: well-circumscribed, often central, calcified, highly vascular; "salt and pepper" appearance on octreotide scan; associated with carcinoid syndrome only when metastatic
Pregnant Patient
- Radiation dose considerations for CT and PET
- MRI (no contrast) can be used for characterization in some cases
- Management generally deferred unless high suspicion, then VATS can be performed with appropriate precautions in 2nd trimester
13. QUESTIONS TO ASK THAT WILL STUMP YOUR PROFESSORS
-
"If FDG-PET has 97% sensitivity for detecting malignancy in a nodule, why do the guidelines say a negative PET cannot rule out malignancy in a 9 mm nodule?"
- Answer: Because a false-negative PET still has a post-test probability of ~18% malignancy (one study found 18% of PET-negative solid nodules were ultimately malignant). A negative test reduces probability but doesn't eliminate it - Bayesian reasoning applies.
-
"The Fleischner Society says no follow-up for solid nodules <6 mm in low-risk patients. But what if that nodule is in the right upper lobe with a spiculated margin and the patient is a 70-year-old ex-smoker?"
- Answer: The guidelines explicitly state that "suspicious morphology, upper lobe location, or both can increase cancer risk into the 1-5% range; therefore follow-up at 12 months may be considered depending on comorbidity and patient preference." Guidelines are not algorithms - they require individualization.
-
"What is the volume doubling time paradox with GGOs, and why do we follow them for 5 years instead of 2?"
- Answer: Solid lung cancers have VDT of 20-400 days. But GGO-type adenocarcinomas (AAH, AIS, MIA) have VDT that can exceed 800-1400 days. A nodule can appear stable for 2 full years and still be pre-invasive or invasive cancer that is simply growing very slowly. The AAH→AIS→MIA→invasive progression is years-long. Two years of stability is NOT reassuring for pure GGOs.
-
"Can a calcified nodule be malignant?"
- Answer: Yes. Eccentric, stippled, or amorphous calcification can represent cancer that has engulfed a pre-existing calcified granuloma or dystrophic calcification within a tumor. Only central, diffuse, laminated, or popcorn calcification reliably indicates benignity.
-
"Why is FDG-PET essentially useless for ground-glass nodules?"
- Answer: The cells in GGO lesions (AAH, AIS, MIA) have low metabolic activity even when malignant. FDG-PET sensitivity for GGOs is only ~10%, specificity only ~20%. The biology - low cellularity, lepidic growth pattern, preserved air spaces - means glucose metabolism is too low to generate a positive signal.
-
"In a patient who presents with a 2.5 cm SPN, if CT shows it to be spiculated and PET shows SUVmax of 4.2, what is the next step - biopsy first or surgery first?"
- Answer: In a patient fit for surgery with high probability (spiculated + PET-positive), proceeding directly to VATS resection is appropriate - it is both diagnostic and therapeutic. CT-guided biopsy is usually reserved for: confirming malignancy before neo-adjuvant chemotherapy, confirming recurrence, high surgical risk patients, or when non-surgical treatment is planned.
-
"What molecular assay can be used non-invasively on blood or BAL to help classify an intermediate-risk nodule?"
- Answer: Nodify XL2 (plasma protein panel: LG3BP + C163A), Nodify CDT (autoantibody panel), and various microRNA panels. When pretest probability is intermediate and test indicates low risk, invasive biopsy can be safely deferred. This is the most current frontier.
14. RAPID-FIRE SUMMARY TABLE
| Question | Answer |
|---|---|
| Size definition of SPN | ≤3 cm |
| Size of mass | >3 cm |
| Most common malignant type | Adenocarcinoma (47%) |
| Most common benign cause | Infectious granuloma (80% of benign) |
| 2nd most common benign cause | Hamartoma (~10%) |
| Only 2 signs that definitively predict benignity | No growth >2 years + benign calcification pattern |
| Most reliable benign calcification patterns | Central, diffuse, laminated, popcorn |
| PET threshold for malignancy | SUVmax >2.5 |
| PET threshold nodule size | ≥8 mm (not useful below this) |
| PET sensitivity/specificity | 87-97% / 78-82% |
| VDT of lung cancer | 20-400 days |
| VDT <20 days | Infection |
| VDT >400 days | Usually benign (but can be slow-growing cancer!) |
| Fleischner 2017 - no follow-up low-risk cutoff | <6 mm solid |
| Fleischner 2017 new vs. old cutoff | Changed from 4 mm to 6 mm |
| Highest risk nodule type | Part-solid (semisolid) |
| GGO follow-up duration | Up to 5 years |
| CT collimation for nodule evaluation | 1-2 mm thin sections |
| Hamartoma fat density range | -40 to -120 HU |
| Corona radiata sign | Fine linear strands radiating 4-5 mm from nodule |
| Pleural tail sign - now considered | Non-specific (both benign and malignant) |
| PET for GGO sensitivity | Only ~10% - essentially useless |
| Best tissue sampling for peripheral nodule | CT-guided TTNB or VATS |
| Pneumothorax rate with TTNB | 10-30% |
| Gold standard surgical resection | Lobectomy (VATS preferred) |
Sources: Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine; Harrison's Principles of Internal Medicine 22e (2025); Goldman-Cecil Medicine; Schwartz's Principles of Surgery 11e; Fleischner Society Guidelines 2017 (Radiology); ACR Appropriateness Criteria 2026 [PMID 41721805]; AATS Consensus 2024 for Subsolid Nodules [PMID 38878052]; ESTI Screening Guidelines 2026 [PMID 40593170]
This is a shared conversation. Sign in to Orris to start your own chat.