Excellent content gathered. Now I have comprehensive material from both Andrews' Clinical Dermatology and Robbins Pathology. Let me compile the complete notes now:
🦠 HANSEN'S DISEASE (LEPROSY) — Complete NEET PG / INI-CET 2026 Notes
Sources: Andrews' Diseases of the Skin — Clinical Dermatology | Robbins, Cotran & Kumar — Pathologic Basis of Disease | Roitt's Essential Immunology | Sherris Medical Microbiology
1. INTRODUCTION & EPIDEMIOLOGY
- Hansen's disease = chronic granulomatous infection caused by Mycobacterium leprae (and rarely M. lepromatosis, proposed 2008)
- Obligate intracellular pathogen — infects dermal macrophages and Schwann cells
- Cannot be cultured in vitro (only in armadillo foot pads and mouse foot pads)
- Grows optimally at 32–34°C → prefers cooler tissues: skin, peripheral nerves, anterior eye, testes, upper airway
- Does NOT affect CNS, liver parenchyma, or bones directly (core temperature too high)
- Incubation period: 2–5 years (tuberculoid); 8–12 years (lepromatous) — longest incubation of any bacterial infection
- Global burden: ~200,000 new cases/year; endemic in India, Brazil, Indonesia, SE Asia, Africa
- India: elimination target <1/10,000; current prevalence ~0.45/10,000
Transmission
- Respiratory droplets (nasal secretions of LL patients) — primary route
- Skin-to-skin contact (prolonged close contact)
- Zoonotic reservoir: Nine-banded armadillo (Dasypus novemcinctus) — in southern USA
- NOT highly contagious — 95% of humans are naturally immune
2. MICROBIOLOGY OF M. LEPRAE
| Feature | Detail |
|---|
| Type | Gram-positive, acid-fast bacillus (AFB) |
| Shape | Rod-shaped, arranged in "cigar bundles" (globi) |
| Culture | Cannot be cultured in vitro |
| Animal model | Armadillo, nude mouse footpad |
| Virulence factor | PGL-1 (phenolic glycolipid-1) — essential for host cell invasion |
| Immune evasion | Inhibits mitochondrial energy metabolism; downregulates MHC |
| BCG cross-protection | Yes — BCG confers ~50% protection |
| Staining | Fite-Faraco stain (for tissue); Ziehl-Neelsen stain |
| Replication time | 13 days (slowest of all bacteria) |
NEET Key: M. leprae has the longest doubling time of any bacterium (~13 days). Cannot be cultured on artificial media.
3. IMMUNOLOGY — THE SPECTRUM CONCEPT (RIDLEY-JOPLING)
The form of leprosy depends entirely on host cell-mediated immunity (CMI):
HIGH CMI ←————————————————————————————→ LOW CMI
TT BT BB BL LL
(Tuberculoid) (Lepromatous)
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|
| Immune response | Strong Th1 (IL-2, IFN-γ, IL-12, Th17) | Weak Th1; Th2 dominant (IL-4, IL-5, IL-10); ↑ T-reg cells |
| Macrophage type | M1 (classically activated) | M2 (alternatively activated); lepra cells |
| Bacteriology | Paucibacillary (few/no bacilli) | Multibacillary (numerous bacilli, globi) |
| Lepromin test | Strongly positive | Negative |
| Antibody (anti-PGL-1) | Low | High (not protective) |
| Immune complexes | No | Yes → ENL, vasculitis, glomerulonephritis |
| Histology | Well-formed epithelioid granulomas; no bacilli | Foamy (lepra) cells; abundant globi; no/few lymphocytes |
4. CLASSIFICATION
A. Ridley-Jopling Classification (Standard/International)
| Type | Abbreviation | Lesions | Bacilli | Lepromin |
|---|
| Tuberculoid | TT | 1–3; well-defined | 0 | +++ |
| Borderline Tuberculoid | BT | Few; defined edges | Rare | + |
| Mid-Borderline | BB | Several; "punched out" | + | ± |
| Borderline Lepromatous | BL | Many; poorly defined | ++ | − |
| Lepromatous | LL | Diffuse; symmetric | +++ | − |
B. WHO Classification (used for MDT regimen selection — NEET Favourite)
| Type | Skin Smear | Lesion Count | Regimen |
|---|
| Paucibacillary (PB) | Negative | ≤5 lesions | 6 months |
| Multibacillary (MB) | Positive | >5 lesions | 12 months |
NEET Key: WHO PB = ≤5 lesions; MB = >5 lesions. Smear positivity alone = MB regardless of lesion count.
C. Indian Classification (IAL — used in Indian textbooks)
- Indeterminate (I) → Tuberculoid (T) → Borderline (B) → Lepromatous (L)
5. CLINICAL FEATURES
Indeterminate Leprosy
- Earliest form; often the first clinical sign
- Solitary, poorly defined hypopigmented macule on cheek, upper arm, thigh, buttock
- Sensory changes minimal or absent; no nerve enlargement; no nodules
- Histology: lymphocytic infiltrate without granulomas; few or no bacilli
- May spontaneously resolve (if CMI strong) or evolve into TT, BB, or LL
- Diagnosis is not indeterminate — the classification is indeterminate
Tuberculoid Leprosy (TT)
- 1–5 lesions, asymmetrically distributed
- Typical lesion: Large erythematous plaque; sharply elevated, indurated border sloping to a flattened atrophic center → "saucer right side up"
- Dry, scaly, hairless (anhidrotic), anesthetic
- Cardinal signs: Anesthesia + Anhidrosis + Alopecia within the lesion
- Enlarged peripheral nerves near the lesion → tender, cord-like
- "Feeding nerve" = enlarged nerve leading to the lesion (in BT especially)
- Common sites: face, limbs, trunk; NOT scalp, axillae, groin, perineum (these areas are warm/moist → not affected)
- Nerves commonly affected: Greater auricular, superficial peroneal, ulnar (most commonly affected nerve overall), posterior tibial, radial cutaneous, facial
Fig: Tuberculoid leprosy — Andrews' Diseases of the Skin
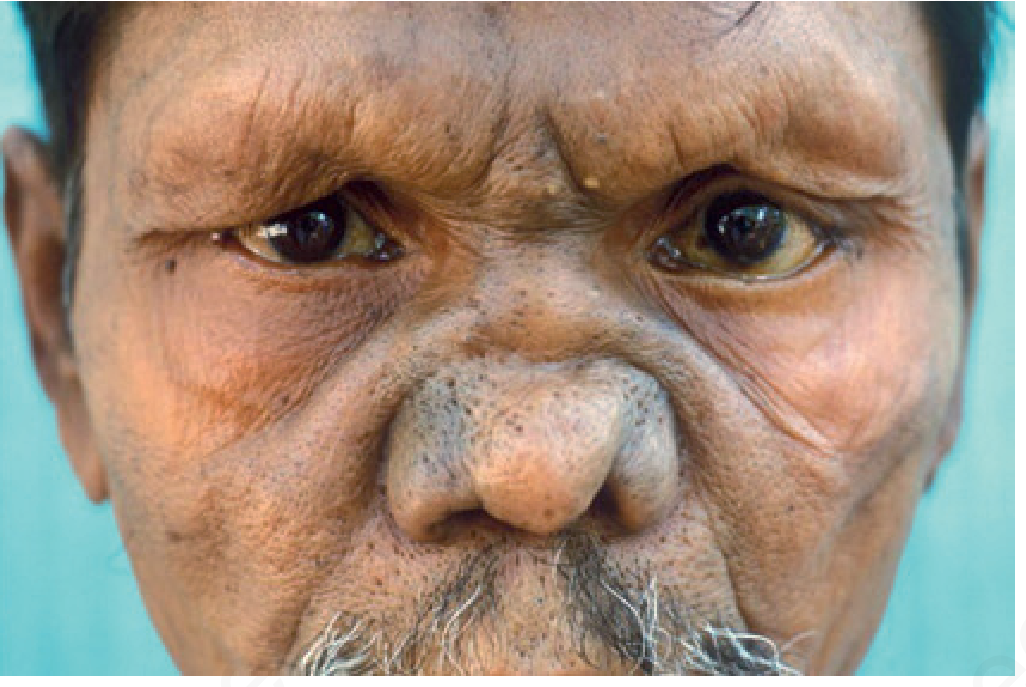
Lepromatous Leprosy (LL)
- Numerous lesions, bilaterally symmetric
- Macular → papular → nodular; coalesce → "leonine facies" (diffuse infiltration of face)
- Skin thickening, loss of eyebrows (madarosis — loss of lateral eyebrows first) and eyelashes
- Sensation relatively preserved early (but eventually lost due to diffuse nerve damage)
- Symmetric peripheral neuropathy (unlike TT where asymmetric)
- Nasal involvement: Chronic nasal congestion → saddle-nose deformity (septal perforation)
- Testes: Orchitis → hyalinization → infertility, gynecomastia
- Lymph nodes: Foamy macrophages in paracortex
- Ocular: Corneal opacities ("iris pearls" = miliary lepromas of iris in BL/LL), lagophthalmos
- Glove and stocking anesthesia — due to symmetric polyneuropathy
- Lucio phenomenon: Specific to LL; hemorrhagic necrotic lesions (form of ENL in Lucio leprosy — diffuse non-nodular lepromatous leprosy in Mexico/Central America)
Fig: Lepromatous leprosy — Andrews' Diseases of the Skin (Courtesy: Shyam Verma)
Borderline Leprosy (BB)
- Most unstable type on the spectrum
- "Punched out" lesions with irregular, vague edges
- Mixed features; may have satellite lesions
- BB leprosy is the most difficult to classify
- Liable to type 1 (reversal) reactions
Histoid Leprosy (Wade's histoid)
- Variant of LL (downgraded/relapsed); classically seen in dapsone resistance or after irregular treatment
- Well-defined, dome-shaped, shiny nodules (resembling dermatofibroma)
- Bacilli in spindle-shaped histiocytes arranged in a storiform pattern
- Highest bacterial index (BI) of all forms
- Can occur over bony prominences (elbows, knees)
6. NERVE INVOLVEMENT — HIGH-YIELD TABLE
| Nerve | Deformity/Feature |
|---|
| Ulnar nerve (most commonly enlarged/affected overall) | Claw hand (4th & 5th fingers); "Benediction sign" = inability to flex ring and little finger |
| Median nerve | Claw hand (index + middle fingers); "Ape hand" (thenar wasting) |
| Combined ulnar + median | Complete claw hand (all 4 fingers) |
| Radial nerve | Wrist drop, finger drop |
| Common peroneal (lateral popliteal) | Foot drop |
| Posterior tibial nerve | Plantar anesthesia, trophic ulcer, claw toes |
| Facial nerve (VII) | Lagophthalmos (inability to close eye) → exposure keratitis |
| Trigeminal nerve (V) | Corneal anesthesia → corneal ulcers |
| Greater auricular nerve | Visibly enlarged (tuberculoid/BT) |
| Radial cutaneous nerve | Enlarged at wrist (BT) |
Memory Aid: Ulnar = most commonly affected nerve in leprosy. Lateral popliteal = most commonly affected lower limb nerve.
Claw hand types:
- Ulnar claw = 4th & 5th fingers clawed (main-en-griffe)
- Median claw = Index + middle fingers
- Combined = all 4 fingers
- "Benediction sign" (Pope's blessing) = ulnar nerve → cannot flex 4th & 5th = they remain extended when asked to make fist
- "Ape hand" = median nerve → thenar wasting, thumb cannot oppose
7. HISTOPATHOLOGY
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|
| Granuloma | Well-formed epithelioid granulomas with Langhans' giant cells; closely resemble TB | Absent; diffuse infiltrate |
| Infiltrating cells | Lymphocytes + epithelioid cells surrounding nerves and adnexae | Foamy macrophages (lepra cells / Virchow cells) filled with bacilli |
| Bacilli | Absent (paucibacillary) | Abundant; arranged in "globi" (cigar bundle pattern); "Mori bodies" |
| Subepidermal clear zone | Absent | Present (Grenz zone — clear zone between epidermis and infiltrate) |
| Nerve | Destroyed, enclosed in granuloma | Infiltrated by bacilli (Schwann cells); onion-skin perineural fibrosis |
| Stain | H&E (no bacilli visible) | Fite-Faraco stain (modified acid-fast) for bacilli; Ziehl-Neelsen for tissue |
NEET Key — Grenz Zone: Pathognomonic of LL — normal collagen-free subepidermal zone between epidermis and the macrophage infiltrate.
Bacterial Index (BI) — Ridley's Logarithmic Scale
| Score | AFB count per oil-immersion field |
|---|
| 0 | No AFB in 100 fields |
| 1+ | 1–10 in 100 fields |
| 2+ | 1–10 per 10 fields |
| 3+ | 1–10 per field |
| 4+ | 10–100 per field |
| 5+ | 100–1000 per field |
| 6+ | >1000 per field (Histoid LL has highest BI) |
Morphological Index (MI)
- % of solid-staining (viable) bacilli in a smear
- Normal = ~25–60% solid bacilli
- After treatment: MI falls to 0 within 3–6 months (earlier than BI)
- MI falls before BI — used to monitor early treatment response
8. LEPROMIN TEST (MITSUDA REACTION)
- Not a diagnostic test — measures cell-mediated immunity (CMI)
- Intradermal injection of autoclaved M. leprae suspension (Mitsuda antigen)
| Reaction | Time | Interpretation |
|---|
| Fernandez reaction (early) | 48–72 hours | Tuberculin-like; indicates prior exposure (type IV hypersensitivity) |
| Mitsuda reaction (late) | 3–4 weeks | Granuloma formation; indicates good CMI; (+) in TT/BT, (−) in LL |
| Type | Lepromin Result |
|---|
| TT | Strongly positive (3+) |
| BT | Positive |
| BB | Weakly positive to negative |
| BL | Negative |
| LL | Strongly negative |
| Healthy population | Positive (~70%) |
| Normal newborns | Negative |
Key: Lepromin positive = good prognosis; Lepromin negative = lepromatous/poor immunity. Diagnostic value = NIL.
9. LEPROSY REACTIONS (HIGH-YIELD)
These are acute immunological episodes that can occur before, during, or after treatment. Do NOT stop MDT during reactions.
Type 1 Reaction (Reversal Reaction — RR)
| Feature | Detail |
|---|
| Mechanism | Type IV (delayed) hypersensitivity — sudden upregulation of CMI |
| Immunology | ↑ IL-2, IFN-γ; CD4+ T cells |
| Spectrum | BT, BB, BL (borderline types — most unstable) |
| NOT in | TT or LL (stable poles) |
| Skin | Existing lesions become red, swollen, edematous, warm — "upgrading" or "downgrading" |
| Nerve | Acute neuritis — painful, tender nerves; sudden nerve function impairment |
| Systemic | No systemic features (fever, lymphadenopathy absent) |
| Timing | During/after MDT |
| Treatment | Systemic corticosteroids (prednisolone 40–60 mg/day) — tapered over 3–6 months |
Type 2 Reaction — Erythema Nodosum Leprosum (ENL)
| Feature | Detail |
|---|
| Mechanism | Type III (immune complex) hypersensitivity — antigen-antibody complex deposition |
| Immunology | ↑ TNF-α, IL-6; complement activation; vasculitis |
| Spectrum | BL and LL only (multibacillary types with high antibody load) |
| Skin | Tender, erythematous nodules (new lesions, NOT existing ones) — on face, extensor limbs; may ulcerate |
| Systemic | Fever, malaise, lymphadenopathy, arthralgia, iridocyclitis, orchitis, nephritis — systemic features present |
| Timing | During/after MDT; 50% of LL patients experience ENL |
| Labs | Neutrophilia, elevated ESR, complement consumption |
| Treatment | Thalidomide (drug of choice; contraindicated in pregnancy — severe teratogen); Prednisolone; Clofazimine (↓ frequency/severity of ENL with long-term use) |
Type 3 Reaction — Lucio Phenomenon
- Specific to diffuse lepromatous (Lucio) leprosy in Mexico/Central America
- Hemorrhagic, necrotic plaques → ulceration
- Mechanism: immune complex vasculitis (similar to ENL but distinct)
- NOT a classic type 1 or type 2 — considered a separate category
Comparison — Type 1 vs Type 2 Reaction (Most Tested)
| Feature | Type 1 (RR) | Type 2 (ENL) |
|---|
| Mechanism | Type IV (cellular) | Type III (immune complex) |
| Spectrum | Borderline (BT/BB/BL) | LL and BL only |
| Skin lesions | Existing lesions — red/swollen | New tender nodules |
| Nerve involvement | Common; acute neuritis | May occur |
| Systemic symptoms | Absent | Present (fever, malaise) |
| Treatment | Prednisolone | Thalidomide |
| Histology | Lymphocytic infiltrate, edema | Neutrophilic infiltrate; vasculitis |
10. MDT — MULTIDRUG THERAPY (WHO REGIMEN)
Adult PB Leprosy (≤5 lesions) — 6 months
| Drug | Daily | Monthly (supervised) |
|---|
| Dapsone | 100 mg daily (self) | — |
| Rifampicin | — | 600 mg (supervised) |
Adult MB Leprosy (>5 lesions) — 12 months
| Drug | Daily | Monthly (supervised) |
|---|
| Dapsone | 100 mg daily (self) | — |
| Clofazimine | 50 mg daily (self) | 300 mg (supervised) |
| Rifampicin | — | 600 mg (supervised) |
Pediatric MDT (10–14 years, weight-adjusted)
- PB: Rifampicin 450 mg monthly + Dapsone 50 mg daily × 6 months
- MB: Rifampicin 450 mg + Clofazimine 150 mg monthly; Dapsone 50 mg + Clofazimine 50 mg alternate days × 12 months
- Clofazimine 6 mg/kg/month (supervised) for children
Single-Lesion PB Leprosy — ROM Regimen
- Rifampicin 600 mg + Ofloxacin 400 mg + Minocycline 100 mg — single dose
- Only for single skin lesion with no nerve involvement (not indeterminate)
Drug Mechanisms & Side Effects
| Drug | MOA | Key Side Effects |
|---|
| Rifampicin | Inhibits RNA polymerase (bactericidal); most rapidly kills M. leprae | Orange urine, hepatotoxicity, drug interactions (CYP inducer) |
| Dapsone | Inhibits PABA incorporation (bacteriostatic) | Methemoglobinemia, hemolytic anemia (G6PD deficiency), dapsone hypersensitivity syndrome (DHS), agranulocytosis |
| Clofazimine | Binds DNA, also anti-inflammatory (anti-ENL effect) | Red-brown/bronze skin discoloration (reversible), ichthyosis, GI upset; not recommended in pregnancy |
NEET Key: Rifampicin = most bactericidal drug in leprosy MDT. Clofazimine = reduces frequency/severity of ENL. Thalidomide = DOC for ENL but teratogenic.
11. DISABILITY GRADING (WHO)
| Grade | Eyes | Hands | Feet |
|---|
| 0 | No problem | No problem | No problem |
| 1 | Visual impairment <6/60; insensitive cornea | Anaesthesia (no deformity) | Anaesthesia (no deformity) |
| 2 | Severe visual impairment ≥6/60 OR obvious deformity (lagophthalmos, iridocyclitis, corneal opacity) | Visible deformity or damage | Visible deformity or damage |
NEET Key: Grade 2 disability = visible deformity. Grade 1 = only anesthesia/impairment without visible deformity.
12. DIAGNOSIS OF LEPROSY
Clinical Diagnosis (WHO Criteria — 3 Cardinal Signs)
- Hypopigmented/erythematous skin lesion with loss of sensation
- Thickened peripheral nerve with sensory/motor loss
- Positive skin smear for AFB
- 1 or more cardinal signs → diagnosis of leprosy
Investigations
| Test | Use |
|---|
| Slit skin smear | Sample from earlobe, forehead, chin, active lesion; Fite-Faraco stained; calculates BI + MI |
| Skin biopsy | Confirms histological type; most important for diagnosis; done at lesion edge |
| Lepromin test | Not diagnostic; measures CMI |
| PCR | Detects M. leprae DNA; useful for indeterminate/pure neural leprosy; can detect drug resistance |
| Serology (anti-PGL-1 IgM) | Elevated in MB leprosy; useful for monitoring relapse |
| Nerve conduction study | Assesses nerve damage |
| Nerve biopsy | Sural nerve; for pure neural leprosy |
Sensory Testing Sequence (First to Last affected)
- Temperature (cold sensation — FIRST to be lost)
- Light touch
- Pain (pin prick)
- Deep pressure (last to be lost)
NEET Key: Temperature sensation is the FIRST to be lost in leprosy.
13. SPECIAL FORMS & ASSOCIATIONS
Pure Neural Leprosy
- Only nerve involvement, no skin lesions
- Can be TT, BT, or LL type
- Constitutes up to 5% of cases in Nepal/India
- Diagnosis: Nerve biopsy (sural nerve most commonly biopsied)
Leprosy in Children
- Indeterminate form most common
- Tuberculoid most common type overall in children
- BCG vaccination offers partial protection
Leprosy and Pregnancy
- Type 1 and type 2 reactions ↑ during pregnancy and postpartum
- Clofazimine: relatively contraindicated (crosses placenta → neonatal skin discoloration)
- Thalidomide: absolutely contraindicated in pregnancy
- MDT (rifampicin + dapsone) — safe in pregnancy
Leprosy and HIV
- HIV does not dramatically increase risk of leprosy
- Can cause immune reconstitution inflammatory syndrome (IRIS) → type 1 reactions after ART
- HIV + leprosy = more unusual presentations
14. VACCINES IN LEPROSY
| Vaccine | Detail |
|---|
| BCG | ~50% protection; children benefit most; revaccination may increase protection |
| MIP (Mw vaccine) | Mycobacterium indicus pranii; developed at JALMA, Agra (ICMR); immunoprophylactic + immunotherapeutic; used as adjuvant with MDT |
| LepVax | Novel subunit vaccine in trials |
NEET Key: MIP vaccine = developed in India (JALMA, Agra/Delhi — answer varies by source; JALMA is in Agra); used as adjunct in MB leprosy. BCG gives partial protection.
15. OCULAR, NASAL & SYSTEMIC INVOLVEMENT
Ocular (Lepromatous)
- Lagophthalmos (VII nerve) → exposure keratitis
- Corneal anesthesia (V nerve) → corneal ulcers
- Iris pearls (miliary lepromas of iris) — in BL/LL
- Corneal opacities, avascular keratitis, pannus formation
- Iridocyclitis (in ENL reactions)
Nasal
- Chronic nasal congestion → epistaxis
- Septal perforation → saddle-nose deformity
- Loss of upper incisor teeth (from alveolar infiltration in LL)
Testes
- Orchitis → destruction of seminiferous tubules → azoospermia, infertility, gynecomastia (LL)
Kidney
- ENL → immune complex glomerulonephritis (mesangial)
16. LEPROSY — KEY MNEMONICS
| Mnemonic | Fact |
|---|
| "Ulnar is the MOST common nerve" | Ulnar = most frequently affected nerve in leprosy (elbow level) |
| "Temperature FIRST" | First sensation lost = cold/temperature |
| "ENL = EVERYTHING (systemic)" | Type 2 = fever, lymphadenopathy, iritis, orchitis |
| "Reversal = Reversal of CMI (Borders go up)" | Type 1 = borderline spectrum; no systemic features |
| "Thalidomide for ENL, Prednisolone for RR" | Treatment distinction |
| "Grenz zone = LL" | Subepidermal clear zone in lepromatous leprosy |
| "BI falls slowly, MI falls fast" | MI → 0 in 3–6 months; BI takes years |
| "Histoid = Highest BI" | Wade's histoid leprosy |
| "6P in PB, 12P in MB" | 6 months PB; 12 months MB |
17. PREVIOUS YEAR QUESTIONS (PYQ) — NEET PG / INI-CET / AIPGMEE
🔴 PYQ BLOCK 1 — Bacteriology & Immunology
Q1. [NEET PG / AIPGMEE] The doubling time of M. leprae is:
- A. 24 hours
- B. 6 days
- C. 13 days ✅
- D. 30 days
Explanation: M. leprae replicates every 13 days — slowest of all bacteria. This explains the long incubation period (2–12 years).
Q2. [AIPGMEE] Lepromin test is positive in all EXCEPT:
- A. Tuberculoid leprosy
- B. Normal adults
- C. Sarcoidosis
- D. Lepromatous leprosy ✅
Explanation: Lepromin measures CMI. LL has defective CMI → strongly negative. TT, normal adults, sarcoidosis, and BCG-vaccinated individuals are lepromin positive.
Q3. Which of the following correctly describes the lepromin test?
- A. It is diagnostic of leprosy
- B. It requires a live bacillus suspension
- C. It measures cell-mediated immunity ✅
- D. Mitsuda reaction is read at 48–72 hours
Explanation: Lepromin measures CMI, not diagnostic. Mitsuda reaction = 3–4 weeks (granuloma). Fernandez = 48–72 hours (early reaction).
Q4. [INICET] BCG vaccination provides protection against leprosy by:
- A. Producing anti-PGL-1 antibodies
- B. Activating Th2 cells
- C. Cross-reactive CMI against M. leprae ✅
- D. Directly neutralizing M. leprae
🔴 PYQ BLOCK 2 — Classification & Histology
Q5. [NEET PG] According to WHO classification, paucibacillary leprosy includes:
- A. ≤3 lesions only
- B. Single lesion only
- C. ≤5 lesions with negative smear ✅
- D. >5 lesions with negative smear
Explanation: WHO PB = ≤5 skin lesions + smear negative. MB = >5 lesions OR smear positive.
Q6. [AIPGMEE 2017] The most characteristic histological feature of lepromatous leprosy is:
- A. Epithelioid granuloma
- B. Caseous necrosis
- C. Foamy macrophages (lepra/Virchow cells) with globi ✅
- D. Neutrophilic microabscesses
Explanation: LL = foamy macrophages (lepra cells) packed with AFB arranged in globi. Grenz zone is also characteristic.
Q7. [AIPGMEE] Grenz zone is seen in:
- A. Tuberculoid leprosy
- B. Borderline leprosy
- C. Lepromatous leprosy ✅
- D. Indeterminate leprosy
Explanation: Grenz zone = subepidermal clear zone in LL — uninvaded subepidermal band of collagen separating epidermis from the macrophage infiltrate.
Q8. [NEET PG / INI-CET] Histoid leprosy is characterized by all EXCEPT:
- A. Well-defined shiny nodules
- B. Seen in previously untreated patients ✅ (Incorrect — seen in dapsone-resistant/relapsed patients)
- C. High bacterial index
- D. Spindle-shaped histiocytes in storiform pattern
Explanation: Histoid leprosy occurs in dapsone resistance or irregular treatment (not untreated). It has the highest BI of all forms.
Q9. What is the most unstable form in the leprosy spectrum?
- A. TT
- B. BB (mid-borderline) ✅
- C. BT
- D. LL
Explanation: BB is the most immunologically unstable — prone to upgrading (toward TT) or downgrading (toward LL) reactions.
🔴 PYQ BLOCK 3 — Clinical Features & Nerve Involvement
Q10. [AIPGMEE / NEET PG] The most commonly enlarged nerve in leprosy is:
- A. Posterior tibial nerve
- B. Ulnar nerve ✅
- C. Greater auricular nerve
- D. Facial nerve
Explanation: Ulnar nerve (at the elbow) is the most commonly involved nerve. It is also the most superficial peripheral nerve — vulnerable to thickening.
Q11. [NEET PG] "Benediction sign" (Pope's sign) in leprosy is due to involvement of:
- A. Radial nerve
- B. Ulnar nerve ✅
- C. Median nerve
- D. Peroneal nerve
Explanation: Ulnar nerve palsy → inability to flex 4th and 5th digits → they remain extended = Benediction/Pope's blessing sign.
Q12. [INICET] Foot drop in leprosy is due to involvement of:
- A. Posterior tibial nerve
- B. Femoral nerve
- C. Common peroneal (lateral popliteal) nerve ✅
- D. Sural nerve
Q13. [NEET PG 2023] A patient presents with a hypopigmented anesthetic patch on the trunk. The first sensation to be lost in leprosy is:
- A. Fine touch
- B. Pain
- C. Temperature (cold) ✅
- D. Deep pressure
Explanation: Sequence of sensory loss in leprosy: Temperature → Light touch → Pain → Deep pressure. Temperature (especially cold) is FIRST.
Q14. [AIPGMEE] The feeding nerve in leprosy (nerve visibly running into a skin lesion) is characteristically seen in:
- A. LL leprosy
- B. Indeterminate leprosy
- C. BT (borderline tuberculoid) leprosy ✅
- D. BB leprosy
Explanation: "Feeding nerve" = enlarged nerve trunk leading into the skin lesion, most characteristic of BT leprosy.
Q15. [NEET PG] Saddle-nose deformity in leprosy results from:
- A. Traumatic septal fracture
- B. Granulomatous infiltration of nasal septum (LL) ✅
- C. Type 1 reaction
- D. ENL
Explanation: In LL — nasal mucosa infiltration → septal perforation → saddle-nose deformity.
🔴 PYQ BLOCK 4 — Reactions
Q16. [NEET PG / AIPGMEE] Type 1 reaction (reversal reaction) in leprosy is seen in:
- A. TT leprosy only
- B. LL leprosy only
- C. Borderline spectrum (BT, BB, BL) ✅
- D. All forms of leprosy
Explanation: Type 1 reactions occur in borderline spectrum (BT/BB/BL). TT and LL are stable poles and do NOT develop reversal reactions.
Q17. [NEET PG 2022/2023] Erythema Nodosum Leprosum (ENL) is:
- A. Type I hypersensitivity
- B. Type III (immune complex) hypersensitivity ✅
- C. Type IV hypersensitivity
- D. Type II hypersensitivity
Explanation: ENL = immune complex deposition → complement activation → neutrophil infiltration → vasculitis. Type III reaction.
Q18. [AIPGMEE] Drug of choice for ENL (Erythema Nodosum Leprosum) is:
- A. Prednisolone
- B. Clofazimine
- C. Thalidomide ✅
- D. Dapsone
Explanation: Thalidomide is DOC for ENL. MOA: ↓ TNF-α. CONTRAINDICATED in pregnancy (phocomelia). Prednisolone used when thalidomide unavailable or in women of childbearing age.
Q19. [INICET] During type 1 reaction in leprosy, which of the following is TRUE?
- A. New lesions appear
- B. Systemic features like fever are common
- C. Existing lesions become erythematous and edematous ✅
- D. Immune complexes are deposited in vessel walls
Explanation: Type 1 (RR) — existing lesions flare up; no new lesions; no systemic features. Mechanism = CMI upregulation (Type IV).
Q20. [NEET PG] Lucio phenomenon is seen in:
- A. Borderline leprosy
- B. Tuberculoid leprosy
- C. ENL patients in India
- D. Diffuse lepromatous leprosy (Lucio leprosy) — mainly Mexico/Central America ✅
🔴 PYQ BLOCK 5 — Treatment
Q21. [NEET PG 2024] WHO-recommended treatment for multibacillary leprosy in adults:
- A. Rifampicin + Dapsone × 12 months
- B. Rifampicin + Dapsone + Clofazimine × 12 months ✅
- C. Rifampicin + Clofazimine × 6 months
- D. Rifampicin + Dapsone × 6 months
Q22. [AIPGMEE] Which drug causes red-brown skin discoloration in leprosy treatment?
- A. Dapsone
- B. Rifampicin
- C. Clofazimine ✅
- D. Minocycline
Explanation: Clofazimine → reddish-brown/bronze skin discoloration (reversible on stopping). Also causes ichthyosis and GI side effects.
Q23. [NEET PG] Dapsone causes all of the following EXCEPT:
- A. Methemoglobinemia
- B. Hemolytic anemia in G6PD deficiency
- C. Hepatocellular carcinoma ✅ (Not a known effect)
- D. Agranulocytosis
Q24. [INICET] ROM regimen in leprosy consists of:
- A. Rifampicin, Ofloxacin, Metronidazole
- B. Rifampicin, Ofloxacin, Minocycline — single dose ✅
- C. Rifampicin, Ofloxacin, Moxifloxacin
- D. Rifampicin, Ofloxacin, Minocycline × 6 months
Explanation: ROM = single-dose treatment for single lesion PB leprosy only.
Q25. [NEET PG 2025 Recall] A young patient presents with non-progressive hypopigmented lesion on trunk. Wood's lamp shows white accentuation. Diascopy is negative. Most likely diagnosis:
- A. Vitiligo
- B. Nevus depigmentosus ✅ (Note: Some sources say indeterminate leprosy — the KEY differentiator is white accentuation on Wood's lamp WITHOUT complete depigmentation)
- C. Nevus anemicus
- D. Indeterminate leprosy
Explanation: Vitiligo = chalky-white/brilliant fluorescence. Nevus depigmentosus = hypopigmented (not depigmented); white accentuation (but not chalk-white). Diascopy negative rules out vascular lesion. Indeterminate leprosy would show anesthesia within the lesion.
🔴 PYQ BLOCK 6 — Miscellaneous
Q26. [AIPGMEE] Morphological Index (MI) in leprosy smear indicates:
- A. Number of bacilli per field
- B. Percentage of solid (viable) bacilli ✅
- C. Granuloma density
- D. Nerve damage extent
Explanation: MI = % of solidly staining bacilli (viable). Falls to 0 first (3–6 months) → best early indicator of therapeutic response.
Q27. [NEET PG] In WHO disability grading of leprosy, Grade 1 for hands means:
- A. Visible deformity or damage
- B. Claw hand
- C. Anesthesia of the palm (no visible deformity) ✅
- D. Loss of digits
Q28. [INICET] MIP vaccine for leprosy was developed at:
- A. NIMHANS, Bangalore
- B. JALMA, Agra (ICMR) ✅
- C. AIIMS, New Delhi
- D. CMC, Vellore
Q29. [AIPGMEE] Clofazimine in leprosy acts by:
- A. Inhibiting RNA polymerase
- B. Inhibiting PABA synthesis
- C. Binding to mycobacterial DNA + anti-inflammatory effect ✅
- D. Inhibiting cell wall synthesis
Q30. [NEET PG] All are true about lepromatous leprosy EXCEPT:
- A. Symmetric skin lesions
- B. Leonine facies
- C. Lepromin test positive ✅
- D. Highest bacterial index
Explanation: Lepromin is NEGATIVE in LL. All other options are true for LL.
RAPID REVISION TABLE — NEET PG FAVOURITE COMPARISONS
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|
| Lesion count | 1–3 (few) | Numerous |
| Symmetry | Asymmetric | Symmetric |
| Sensation in lesion | Anesthetic | Reduced/normal early |
| Lepromin test | Strongly +ve | Strongly −ve |
| Bacilli in smear | 0 (PB) | +++ (MB) |
| Granuloma | Well-formed | Absent |
| Histology | Epithelioid granuloma | Lepra cells + Globi |
| CMI | High (Th1) | Low (Th2) |
| Prognosis | Good | Poor (without treatment) |
| Nerve damage | Early, asymmetric | Late, symmetric |
| Communicability | Low | High |
| Reactions | Type 1 (if BT) | Type 2 (ENL) |
Sources: Andrews' Diseases of the Skin – Clinical Dermatology | Robbins, Cotran & Kumar – Pathologic Basis of Disease 10e | Roitt's Essential Immunology | Indian Journal of Postgraduate Dermatology (Leprosy Quiz, 2024)
This covers the complete syllabus for Hansen's disease as tested in NEET PG and INI-CET. Key high-frequency exam areas:
- Ridley-Jopling vs WHO classification — lesion counts, smear status
- Type 1 vs Type 2 reactions — mechanism, spectrum, treatment
- Nerve involvement table — ulnar (most common), peroneal (foot drop), facial (lagophthalmos)
- MDT regimens — 6 months PB vs 12 months MB; ROM single dose
- Lepromin test — not diagnostic; Mitsuda reaction at 3–4 weeks
- Histology — epithelioid granuloma (TT) vs foamy lepra cells + Grenz zone (LL)
- Thalidomide for ENL; Prednisolone for Type 1/RR
- First sensation lost = Temperature (cold)