Squamous cell carcinoma
Reading File
Finding Sources
Searching PubMed
"squamous cell carcinoma" AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a thorough, image-rich answer. Let me compile it.
Squamous Cell Carcinoma (SCC)
Definition
Squamous cell carcinoma is a malignant neoplasm arising from epidermal keratinocytes (or from squamous epithelium at other sites). It is the second most common skin malignancy after basal cell carcinoma (BCC), and recent evidence suggests its incidence may be approaching that of BCC. Unlike BCC, SCC carries a significant risk of regional and distant metastasis.
- Fitzpatrick's Dermatology, Vol. 1-2
Etiology and Pathophysiology
The development of SCC is multifactorial. The diagram below from Fitzpatrick's summarizes the key converging factors:
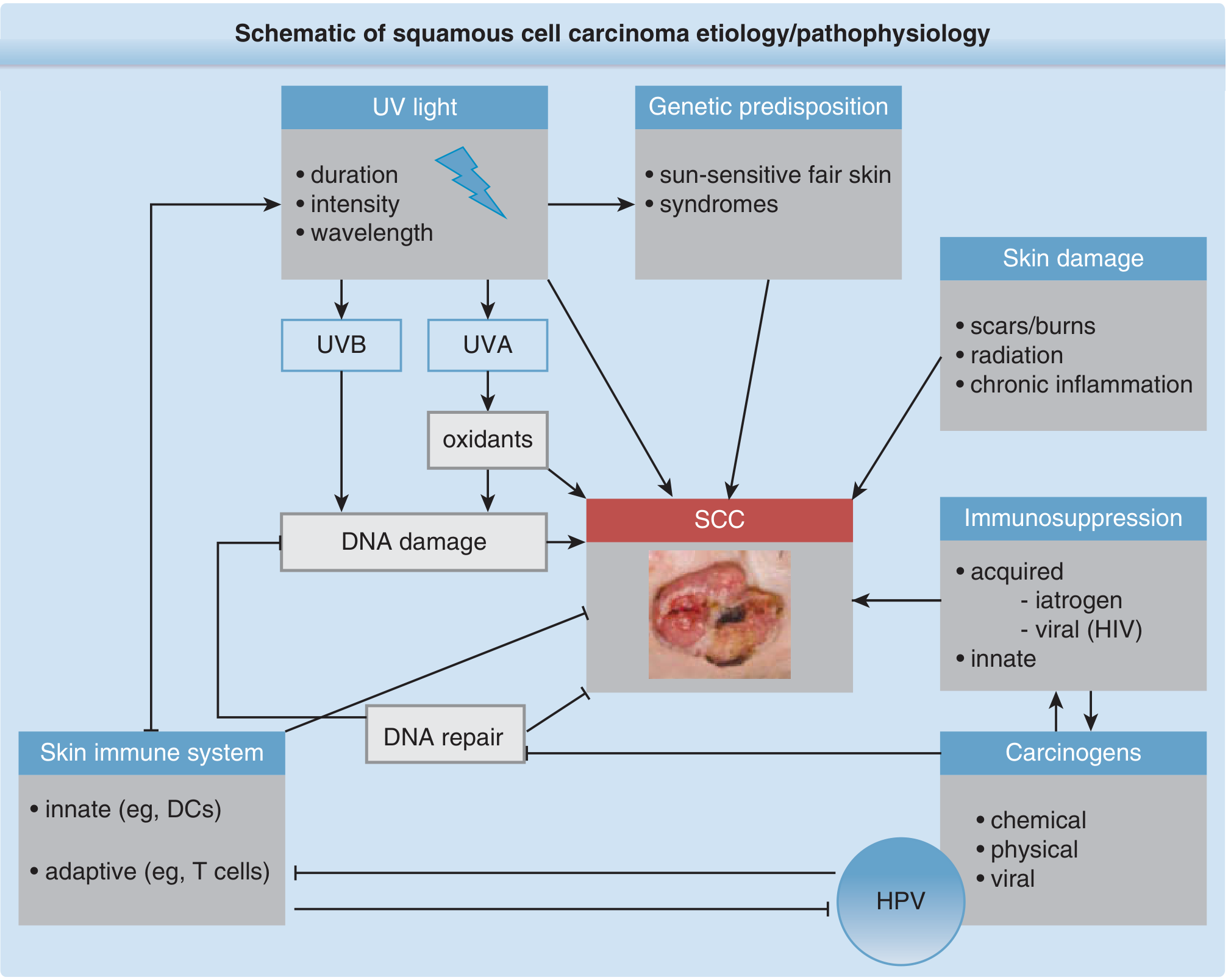
1. Ultraviolet Radiation (Primary Risk Factor)
- Both UVB and UVA are carcinogenic, with a strong dose-response relationship
- UVB causes direct UV signature mutations: characteristic C→T and CC→TT dipyrimidine transitions in TP53 and other genes
- UVA contributes via photooxidative stress and reactive oxygen species
- UVR also exerts immunosuppressive effects: depletes Langerhans cells, impairs antigen presentation, expands regulatory T cells, and shifts the response toward Th2
2. Molecular Pathogenesis
| Gene/Pathway | Role |
|---|---|
| TP53 (most prominent) | UV-induced mutations impair apoptosis and cell-cycle arrest; TP53 loss provides growth advantage to damaged keratinocytes |
| RAS protooncogene | Activating mutations in ~21% of SCCs (Hras 9%, Nras 7%, Kras 5%); drives tumorigenesis |
| EGFR | Persistently overactivated in SCC; upregulates MAPK and mTOR signaling; targeted therapeutically |
3. Other Risk Factors
- Genetic predisposition: Skin phototypes I/II (fair skin); MC1R variants; oculocutaneous albinism (1000-fold increased risk in Black albinos)
- Genodermatoses: Xeroderma pigmentosum (XPA-G, XP-V defects), Recessive dystrophic epidermolysis bullosa (>90% cumulative SCC risk by age 55)
- Immunosuppression: Organ transplant recipients (OTRs) have markedly elevated risk; SCC accounts for >60% of skin cancer deaths in OTRs
- HPV: Certain HPV types inhibit p53-mediated checkpoints via E6/E7 oncoproteins (especially relevant in anogenital SCC and oropharyngeal SCC)
- Skin damage: Chronic scars/burns, radiation exposure, chronic inflammation (Marjolin's ulcer concept)
- Chemical carcinogens: Arsenic, polycyclic aromatic hydrocarbons, tobacco (oral SCC)
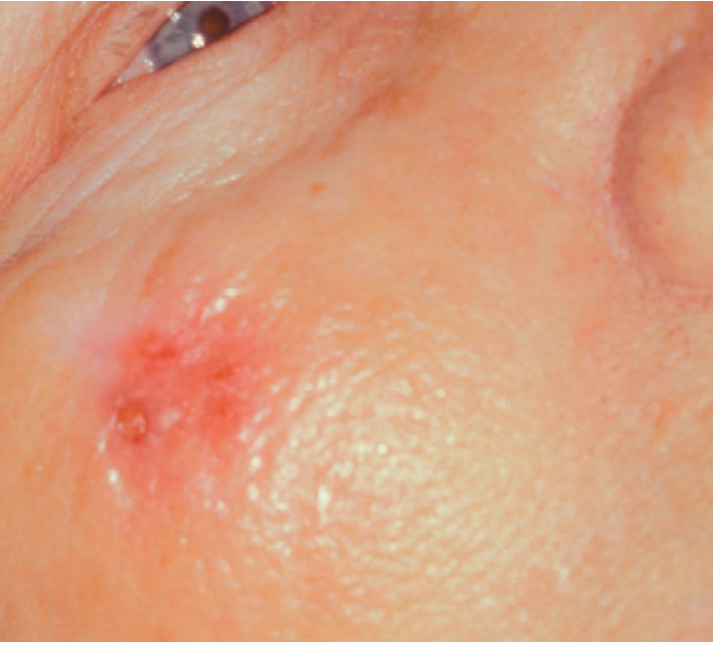
Clinical Features
SCC most commonly appears on chronically sun-exposed sites (scalp, face, ears, dorsal hands, lips) as:
- A diffuse, non-healing, crusted or ulcerated lesion
- A firm, indurated nodule or plaque, often with surrounding erythema
- May arise at the base of an actinic keratosis (AK) - the principal precursor lesion
- Lesions may be multifocal
Clinical photo - SCC lesion:
SCC in Situ (Bowen's Disease)
- Severely dysplastic lesion confined to the epidermis (has not yet invaded the dermis)
- Presents as a well-demarcated, erythematous, scaly plaque
- Treated similarly to invasive SCC; excision is rarely required unless concern for invasion
Histopathology
Classic findings: Atypical keratinocytes originating in the epidermis and infiltrating into the dermis.
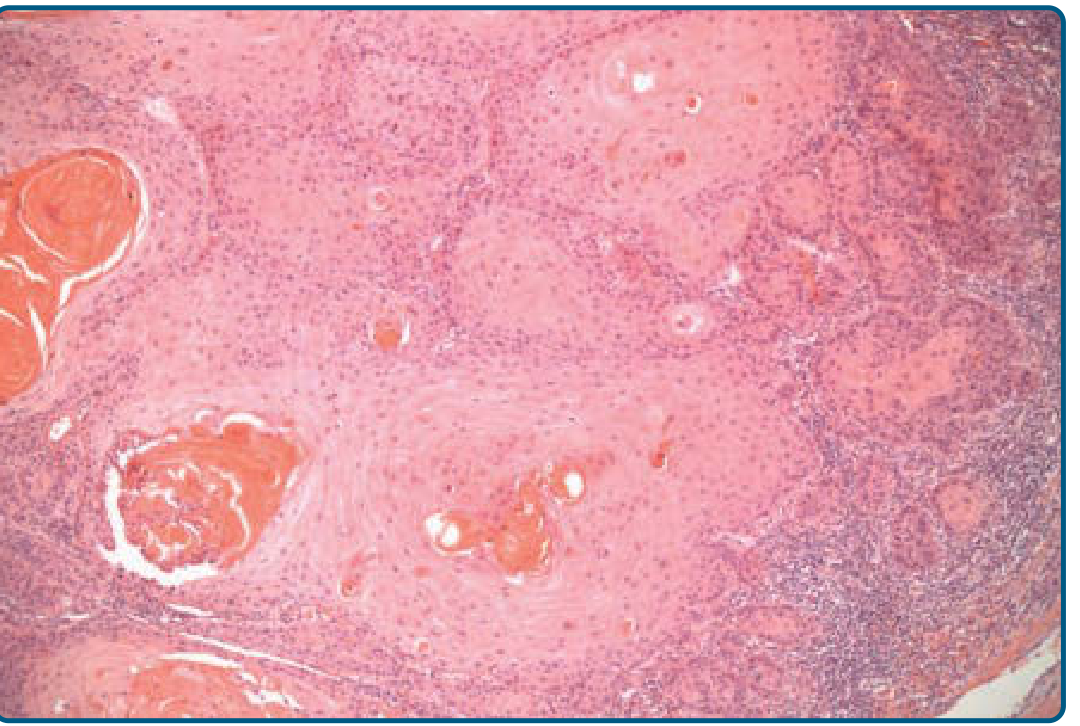
The degree of differentiation is the key histologic variable:
- Well-differentiated (Grade 1): Minimal pleomorphism, prominent keratinization, parakeratosis, individual cell dyskeratosis, horn (keratin) pearl formation
- Poorly differentiated (Grade 3-4): Pleomorphic nuclei, high atypia, frequent mitoses, minimal keratinization
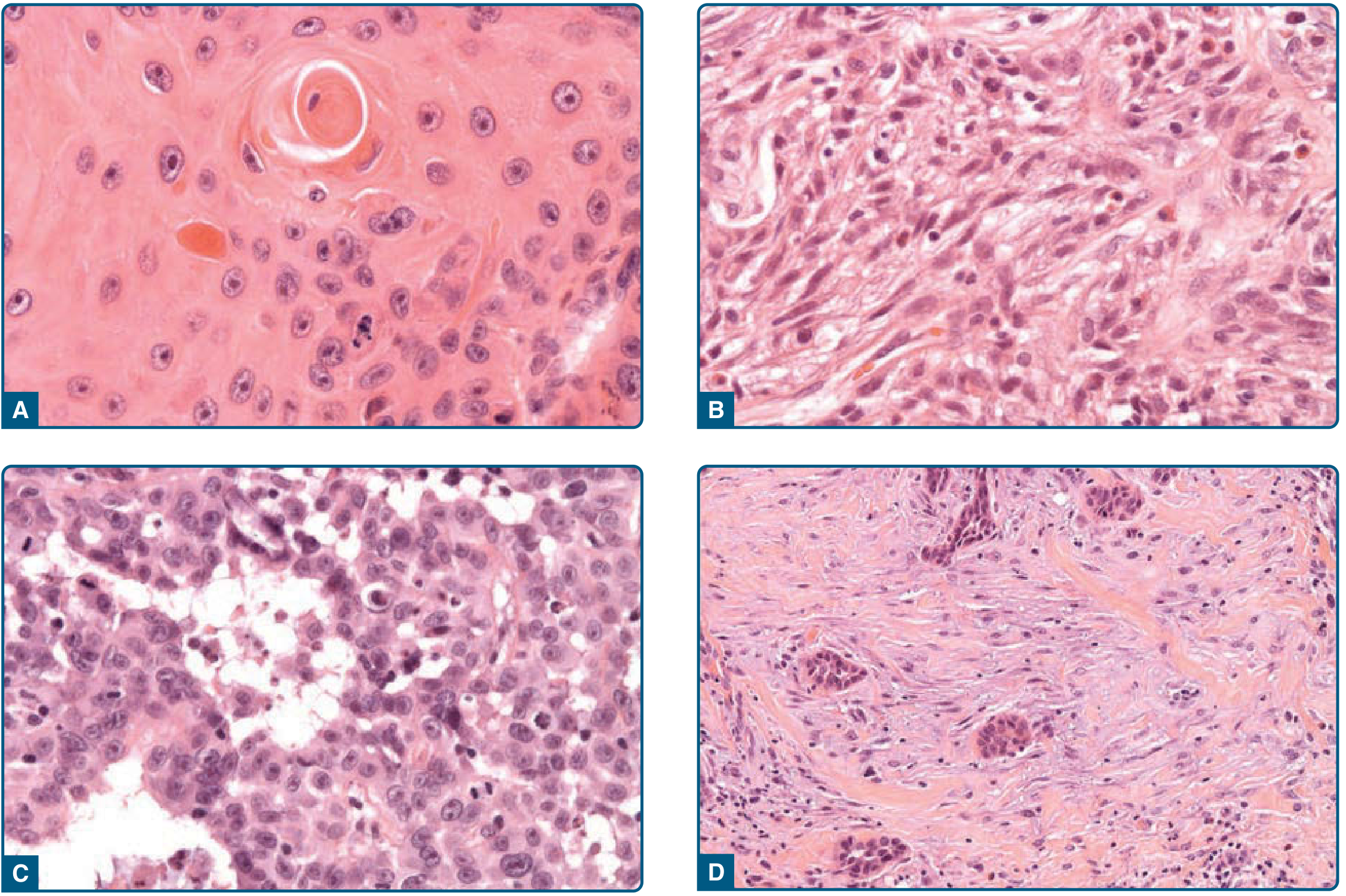
Key Histologic Variants
| Variant | Features | Notes |
|---|---|---|
| Spindle-cell SCC | Spindled keratinocytes, no keratinization | Must differentiate from atypical fibroxanthoma, spindle-cell melanoma, sarcoma (use cytokeratin IHC) |
| Acantholytic (adenoid) SCC | Acantholysis of atypical keratinocytes → pseudoglandular structures | <5% of SCCs; increased metastatic propensity |
| Desmoplastic SCC | Infiltrative growth, abundant mucinous stroma | High-risk variant |
Head & Neck SCC - Special Histology (Goldman-Cecil)
- HPV-negative (environmental): Well- to poorly differentiated; keratin pearls present
- HPV-positive (oropharyngeal): Poorly differentiated or basaloid; no keratin pearls; diagnosed by p16 immunohistochemistry (>70% diffuse nuclear/cytoplasmic staining = HPV-positive); confirms functionally relevant E7 oncoprotein
High-Risk Features (NCCN Criteria)
Four factors most strongly associated with adverse outcomes in cutaneous SCC:
- Diameter >2 cm
- Depth of invasion below subcutaneous adipose
- Perineural invasion
- Immunosuppression (organ transplant recipients)
Additional high-risk criteria per NCCN: location on H-zone of face, aggressive histologic subtype (poorly differentiated, acantholytic, desmoplastic, spindle-cell), recurrent tumor.
Staging (Head & Neck SCC)
Once pathologic diagnosis is established, staging workup includes:
-
Complete head/neck examination with fiberoptic endoscopy
-
CT or MRI for locoregional staging
-
Chest imaging (synchronous pulmonary primary in <10%)
-
HPV status determination for all oropharyngeal SCC (alters both staging and prognosis)
-
Goldman-Cecil Medicine, International Edition
Treatment
1. Surgical Excision (Primary Treatment)
- Standard excision with at least 5 mm clear margins for invasive SCC
- Mohs micrographic surgery is preferred for high-risk tumors (H-zone of face, >2 cm, aggressive histology, perineural invasion, recurrent tumors)
- Recurrence rates: Standard excision 8.1% (primary) / 23.3% (recurrent); Mohs surgery 3.1% / 10.0%
- Mohs provides 3-4x lower recurrence rate than standard excision (supported by meta-analyses of >10,000 patients)
2. Electrodessication and Curettage (ED&C)
- Acceptable for early, small, low-risk lesions
- Not appropriate for high-risk tumors
3. Cryotherapy
- For small, early lesions in good-risk anatomic locations
- Post-treatment residual lesions after treating actinic changes should be biopsied
4. Radiation Therapy
- Used for adjuvant treatment of high-risk or node-positive disease
- Option for patients not surgical candidates
5. Chemotherapy (Advanced/Metastatic)
- Platinum-based regimens, 5-fluorouracil/capecitabine, or methotrexate monotherapy
- Limited effect on overall survival; frequently restricted by comorbidities
6. Targeted Therapy
- Cetuximab (anti-EGFR antibody): 29% response rate in unresectable SCC as first-line monotherapy (Phase II trial); also used as radiosensitizer
- Erlotinib/Gefitinib (EGFR small-molecule inhibitors): off-label options beyond radiotherapy and conventional chemotherapy
- mTOR inhibitors (sirolimus): Reduce secondary SCC incidence in OTRs
7. Immunotherapy
- PD-1/PD-L1 checkpoint inhibitors: Emerging evidence; PD-L1 overexpression in keratinocytes accelerates SCC formation in preclinical models; checkpoint blockade has shown antitumor responses in unresectable SCC
- (Note: Cemiplimab/Libtayo was FDA-approved for advanced cSCC after this textbook's publication - now first-line for unresectable/metastatic cutaneous SCC)
Metastasis and Prognosis
- Overall 5-year metastatic rate: ~5% for all-comers (85% of metastases are nodal)
- Certain high-risk subgroups: metastatic rates up to 30%
- Unresectable SCC: median overall survival only 10.9 months
- OTRs: >60% of skin cancer deaths; 5% disease-specific mortality from SCC
- Local recurrence often precedes distant metastasis and signals aggressive behavior
Follow-Up Schedule
| Cancer | Follow-up |
|---|---|
| Squamous cell carcinoma | 3 months, then 6 months - 1 year |
| Lymph node evaluation | At every follow-up visit |
SCC at Other Sites (Brief Summary)
| Site | Key Features |
|---|---|
| Oral/Oropharyngeal | HPV-positive (base of tongue, tonsil) vs. tobacco/alcohol-associated; staging differs by HPV status |
| Cervical | HPV 16/18 driven; precursor = CIN3/HSIL |
| Vulvar/Penile | High-risk HPV DNA in ~90% of basaloid/warty types |
| Esophageal | Squamous (upper/mid esophagus) vs. adenocarcinoma (lower); associated with tobacco, alcohol, achalasia |
| Urethral | Rare; presents with obstructive/irritative voiding symptoms or palpable mass |
| Anal | HPV-associated; screening guidelines recently updated (PMID: 40019005) |
Sources:
- Fitzpatrick's Dermatology, 8th ed., Vol. 1-2 - Chapters 112, 204
- Goldman-Cecil Medicine, International Edition, 2-Volume Set - Chapter 176
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. - Chapter 12
- Textbook of Family Medicine, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.