Examination of cranial nerve
Reading File
Finding Sources
Searching Images
cranial nerve examination clinical
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive guide to the Examination of Cranial Nerves, structured in numerical order as recommended in clinical practice.
Examination of the Cranial Nerves
Bare minimum screen: Check the fundi, visual fields, pupil size and reactivity, extraocular movements, and facial movements. CNs are best examined in numerical order, except grouping CN III, IV, and VI together due to shared function.
CN I — Olfactory Nerve
- Testing is often omitted unless inferior frontal lobe disease (e.g., meningioma) is suspected.
- With eyes closed, ask the patient to sniff a mild, familiar odorant (toothpaste or coffee) and identify it.
- Test each nostril separately.
CN II — Optic Nerve
| Test | Method |
|---|---|
| Visual acuity | Snellen chart (with glasses/contacts) |
| Visual fields | Confrontation: stand 0.6–1.0 m away, hands at periphery, ask patient to fixate on your face and detect finger movement in all four quadrants (inferior then superior) |
| Optic fundus | Ophthalmoscope — note disc color, size, swelling/elevation; check retinal vessels for hemorrhage, exudates, AV nicking |
- If a field defect is found on screening, test each eye individually and use focal perimetry or a tangent screen for full mapping.
CN III, IV, VI — Oculomotor, Trochlear, Abducens
Pupils
- Describe size, shape, and equality at rest.
- Test direct and consensual light reflex.
- Test accommodation: ask patient to follow your finger moving toward the bridge of the nose — pupils should constrict (accommodation reflex).
Extraocular Movements (EOMs)
- Ask patient to hold head still and track fingertip in the H-pattern (horizontal and vertical planes).
- Note any paresis, nystagmus, or saccadic pursuit.
- Horizontal nystagmus is best assessed at 45° lateral gaze (not extreme gaze) and held for several seconds.
- Ask about diplopia in any direction — true diplopia resolves with one eye closed.
Ptosis
- CN III palsy → ptosis + mydriasis (fixed, dilated pupil) ± "down and out" eye position.

CN V — Trigeminal Nerve
Sensory (three divisions)
| Division | Territory |
|---|---|
| Ophthalmic (V1) | Forehead, upper eyelid, cornea, nose tip |
| Maxillary (V2) | Cheek, upper lip, upper teeth |
| Mandibular (V3) | Lower lip, chin, lower teeth, jaw |
- Test light touch and temperature (or pin-prick) in each territory bilaterally.
- Corneal reflex: touch cornea lightly with cotton wisp — afferent V1, efferent CN VII (blink). Test when suggested by history.
- Motor: ask patient to clench jaw — palpate the masseter muscles for bulk and symmetry. Pterygoids: jaw deviation on opening points to the weak side.
CN VII — Facial Nerve
| Maneuver | What it tests |
|---|---|
| Raise eyebrows / wrinkle forehead | Upper facial muscles |
| Tightly close eyes (resist opening) | Orbicularis oculi |
| Smile / show teeth | Lower facial muscles |
| Puff out cheeks | Buccinator |
Upper vs. Lower Motor Neuron Distinction:
- UMN lesion (e.g., cortical stroke): weakness of the lower two-thirds only; forehead spared (bilateral cortical representation of forehead).
- LMN lesion (e.g., Bell's palsy): weakness of the entire ipsilateral half of the face, including forehead.

CN VIII — Vestibulocochlear Nerve
Cochlear (auditory) component:
- Screen: finger rub or whispered voice at each ear separately.
- Rinne test: vibrating 512 Hz tuning fork placed on mastoid (bone conduction), then at external meatus (air conduction). Normally air > bone (Rinne positive). Reversed in conductive hearing loss.
- Weber test: tuning fork on vertex of skull. Sound lateralizes to the affected ear in conductive loss; to the normal ear in sensorineural loss.
Vestibular component:
- Nystagmus assessment (see CN III/IV/VI section).
- If the patient is in coma or has altered consciousness: ice-water caloric testing (vestibulo-ocular reflex — see below).
CN IX & X — Glossopharyngeal & Vagus Nerves
- Observe the palate and uvula at rest — look for asymmetry.
- Ask patient to say "aah" — the soft palate should rise symmetrically; the uvula deviates away from the side of CN X weakness.
- Gag reflex: stimulate the posterior pharyngeal wall with a tongue blade on each side. Note: the reflex may be absent in normal individuals.
- Check voice quality (hoarseness = vagal dysfunction) and swallowing.
CN XI — Spinal Accessory Nerve
| Muscle | Test |
|---|---|
| Trapezius | Shoulder shrug against resistance |
| Sternocleidomastoid (SCM) | Head rotation against resistance (each side) |
- Weakness of right SCM → difficulty turning head to the left.
CN XII — Hypoglossal Nerve
- Inspect tongue at rest for atrophy or fasciculations (LMN lesion signs).
- Ask patient to protrude the tongue — it deviates toward the side of weakness.
- Test tongue strength: push tongue against inner cheek on each side against examiner's finger.
Quick Reference Summary Table
| CN | Name | Function | Key Test |
|---|---|---|---|
| I | Olfactory | Smell | Identify odorant (each nostril) |
| II | Optic | Vision | Snellen chart, visual fields, fundoscopy |
| III | Oculomotor | EOM (SR, IR, MR, IO), lid, pupil | Pupil reflex, EOM, ptosis |
| IV | Trochlear | EOM (SO — downward/inward) | Depression in adduction |
| V | Trigeminal | Face sensation, mastication | Sensation V1/V2/V3, corneal reflex, jaw clench |
| VI | Abducens | EOM (LR — lateral gaze) | Lateral gaze |
| VII | Facial | Facial expression, taste (anterior 2/3 tongue) | Raise brows, close eyes, smile, puff cheeks |
| VIII | Vestibulocochlear | Hearing, balance | Whisper/Rinne/Weber, nystagmus |
| IX | Glossopharyngeal | Taste (posterior 1/3 tongue), gag afferent | Gag reflex |
| X | Vagus | Palate, pharynx, larynx | Palate rise "aah," voice, gag efferent |
| XI | Spinal Accessory | Trapezius, SCM | Shoulder shrug, head rotation against resistance |
| XII | Hypoglossal | Tongue movement | Tongue protrusion, strength |
Clinical Pearls
- Pupillary response distinguishes structural from toxic-metabolic coma: pupils remain reactive in toxic-metabolic coma but are abnormal (often asymmetric) in structural lesions (e.g., transtentorial herniation).
- In CN III compression (e.g., herniation), pupil dilation precedes ophthalmoplegia because parasympathetic fibers run on the outside of the nerve.
- Pontine lesions cause pinpoint pupils (parasympathetic stimulation + sympathetic loss) — still reactive under magnification.
- Horizontal conjugate deviation: "look toward a stroke, look away from a seizure."
- Vertical dysconjugation (skew deviation) is almost always abnormal and signals a structural rostral brainstem lesion.
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine, International Edition.
Examination of cranial nerve full detail from 4th y standard textbook
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
visual field confrontation testing optic nerve examination
Searching Images
Rinne Weber tuning fork hearing test cranial nerve VIII
Searching Images
pupillary light reflex direct consensual examination
Loading Image
Loading Image
Searching Images
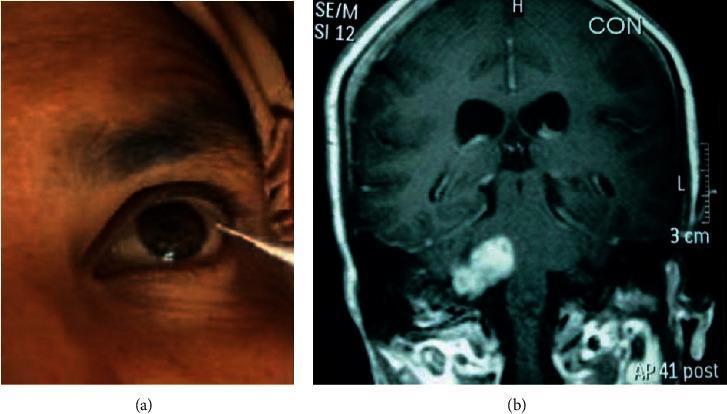
corneal reflex trigeminal facial nerve test cotton wisp
Loading Image
Searching Images
extraocular movement H pattern testing CN III IV VI diplopia
Loading Image
Searching Images
gag reflex palate uvula CN IX X examination tongue protrusion CN XII
Loading Image
Loading Image
I now have all the textbook content and clinical images needed. Let me compile the full, detailed 4th-year standard guide.
Examination of Cranial Nerves — Full Clinical Detail
Source: Adams and Victor's Principles of Neurology 12th Ed; Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine Standard: 4th Year MBBS / Clinical Neurology
Overview
There are 12 pairs of cranial nerves (CNs), each with specific anatomical pathways and clinical tests. Examine them in numerical order, except grouping CN III, IV, VI together (all control eye movement). Deficits provide precise anatomical localization.
CN I — Olfactory Nerve
Anatomy
- Bipolar olfactory receptor neurons → cribriform plate of ethmoid → olfactory bulb → olfactory tract → primary olfactory cortex (piriform/uncus)
- Only sensory CN with no thalamic relay
When to Test
Test whenever inferior frontal lobe disease is suspected (e.g., olfactory groove meningioma, frontal trauma, early Parkinson's or Alzheimer's disease).
Method
- Ensure nasal passages are patent (no obstruction/rhinitis)
- Ask patient to close eyes
- Occlude one nostril at a time
- Present a familiar, non-pungent odorant (toothpaste, coffee, vanilla, cloves) under the open nostril
- Ask: "Can you smell something? What does it smell like?"
- Repeat for other side
Abnormalities
| Term | Meaning |
|---|---|
| Anosmia | Complete loss of smell (unilateral or bilateral) |
| Hyposmia | Reduced smell |
| Parosmia | Distorted smell perception |
| Cacosmia | Everything smells unpleasant |
| Olfactory hallucinations | Suggest temporal lobe (uncal) lesion — "uncinate fits" |
Avoid ammonia — it stimulates trigeminal free nerve endings, not olfactory receptors, and can give false-positive results.
CN II — Optic Nerve
Anatomy
Retinal ganglion cells → optic nerve → optic chiasm (nasal fibers cross) → optic tract → lateral geniculate nucleus → optic radiation → primary visual cortex (occipital lobe)
Tests
1. Visual Acuity
- Use Snellen chart at 6 metres (20 feet), with glasses/contact lenses corrected
- Test each eye separately (cover the other)
- Record as 6/6 (normal), 6/9, 6/12, etc.
- If chart unavailable: count fingers (CF), hand movement (HM), perception of light (PL), or no perception of light (NPL)
2. Visual Fields by Confrontation

Technique:
- Sit facing the patient at ~0.6–1.0 m (2–3 feet)
- Patient covers their right eye; examiner closes their own left eye (mirror image comparison)
- Patient fixes gaze on the examiner's nose/opposite eye
- Examiner places hands at periphery of their own visual field (equidistant plane)
- Move one or two fingers in each quadrant (inferior temporal, inferior nasal, superior temporal, superior nasal)
- Patient reports "now" when movement is seen
- Test each eye separately; then both together (to detect visual inattention/neglect)
Visual Field Defects and Localization:
| Defect | Site of Lesion |
|---|---|
| Monocular blindness | Ipsilateral optic nerve |
| Bitemporal hemianopia | Optic chiasm (pituitary tumour) |
| Homonymous hemianopia | Contralateral optic tract, radiation, or cortex |
| Superior quadrantanopia | Temporal lobe (Meyer's loop) |
| Inferior quadrantanopia | Parietal lobe (upper optic radiation) |
| Macular sparing | Occipital cortex lesion |
| Central scotoma | Optic nerve/macular disease |
3. Colour Vision
- Use Ishihara plates (test for red-green colour defects — optic neuritis classically impairs colour early)
- Bedside: compare redness of a red hat pin in each eye
4. Pupillary Reflexes (see CN III for full detail)
- Swinging flashlight test (RAPD): Swing light between eyes every 2–3 seconds. If the pupil of one eye dilates when light swings to it (instead of maintaining constriction), there is a Relative Afferent Pupillary Defect (RAPD/Marcus Gunn pupil) → ipsilateral optic nerve or retinal disease
5. Fundoscopy (Ophthalmoscopy)

Examine in a darkened room after pupillary dilation if necessary:
- Optic disc: colour (pale = optic atrophy), margins (blurred = papilloedema), cup-to-disc ratio
- Retinal vessels: calibre, AV nicking, silver/copper wiring, haemorrhages, exudates
- Macula: drusen, haemorrhage, degeneration
- Retina: pigmentary changes, detachment
Papilloedema signs: blurred disc margins, absent venous pulsations, disc elevation, flame haemorrhages around disc
CN III, IV, VI — Oculomotor, Trochlear, Abducens
Anatomy
| CN | Muscle(s) | Action |
|---|---|---|
| III (Oculomotor) | SR, IR, MR, IO, levator palpebrae | Elevation, depression, adduction; lid elevation; pupil constriction (parasympathetic) |
| IV (Trochlear) | Superior oblique (SO) | Depression + intorsion in adduction |
| VI (Abducens) | Lateral rectus (LR) | Abduction |
Tests
1. Inspect for Ptosis
- Ptosis = drooping of upper lid (>2 mm)
- Partial ptosis + miosis (Horner syndrome): sympathetic chain lesion
- Complete ptosis + fixed dilated pupil: CN III palsy (compressive — posterior communicating artery aneurysm)
- Bilateral ptosis: myasthenia gravis, bilateral CN III, myopathy
2. Pupil Examination
| Test | Method | Normal | Abnormal |
|---|---|---|---|
| Direct light reflex | Shine light in eye | Pupil constricts | Absent = CN III or optic nerve lesion |
| Consensual reflex | Light in one eye | Opposite pupil constricts | Absent = CN III or optic nerve lesion |
| Accommodation reflex | Finger approaching nose | Pupils constrict (convergence) | Absent = CN III or Argyll Robertson |
| RAPD (swinging flashlight) | Alternate light between eyes | Both stay constricted | Dilation in one eye = optic nerve disease |
Argyll Robertson pupil: small, irregular, accommodates but doesn't react to light — pathognomonic of neurosyphilis
Horner syndrome triad: ptosis + miosis + anhidrosis (sympathetic lesion at T1 or sympathetic chain)
3. Extraocular Movements (EOMs)

Technique:
- Ask patient to hold head still
- Hold your finger ~0.5 m from the patient's face
- Ask patient to track the finger with eyes only, following an "H" pattern:
- Lateral → up → down (tests SR, IR, LR)
- Medial → up → down (tests IO, SO, MR)
- Pause at each position for 2–3 seconds and observe for:
- Nystagmus (especially at lateral gaze — hold for 30 seconds)
- Failure to move (palsy)
- Conjugate vs. disconjugate movement
Ask at each position: "Do you see double?" — true diplopia resolves on closing one eye.
Key EOM Defects:
| Defect | Nerve | Finding |
|---|---|---|
| Failure to adduct | CN III | MR paresis |
| "Down and out" eye | CN III (complete) | All muscles except LR and SO |
| Failure to look down in adduction | CN IV | Difficulty going down stairs; head tilt away |
| Failure to abduct | CN VI | Horizontal diplopia, greatest on gaze toward lesion |
| Internuclear ophthalmoplegia (INO) | MLF lesion | Failure of adduction ipsilateral + nystagmus of abducting eye |
Nystagmus assessment:
- Test at 45° lateral gaze (not at extreme gaze — physiological endpoint nystagmus occurs)
- Hold position for at least 30 seconds
- Note: direction, fast vs slow phase, horizontal/vertical/rotatory
CN V — Trigeminal Nerve
Anatomy
- Three sensory divisions: Ophthalmic (V1), Maxillary (V2), Mandibular (V3)
- One motor division: muscles of mastication (masseter, temporalis, pterygoids) — via mandibular branch
- Sensory nucleus extends from pons to C3 spinal cord
Tests
1. Facial Sensation
Method:
- Test each division bilaterally with:
- Light touch (cotton wisp) — dorsal column pathway via main sensory nucleus
- Pain/pin-prick (broken orange stick, NOT a needle) — spinothalamic pathway via spinal nucleus
- Temperature (cold tuning fork or tubes with hot/cold water) — optional but sensitive
| Division | Area to Test |
|---|---|
| V1 (Ophthalmic) | Forehead, scalp (above supraorbital line), upper eyelid, cornea, dorsum of nose |
| V2 (Maxillary) | Cheek, lower eyelid, lateral nose, upper lip, upper teeth |
| V3 (Mandibular) | Lower lip, chin, lower teeth, jaw, anterior ear |
Note: The angle of the jaw is supplied by C2/C3, NOT the trigeminal nerve — an important clinical discriminator for functional/psychogenic sensory loss.
2. Corneal Reflex
- Afferent: V1 (nasociliary branch → trigeminal ganglion → pontine sensory nucleus)
- Efferent: CN VII (facial nerve → orbicularis oculi)
Technique:
- Approach the cornea from the side (not from above — to avoid blinking to visual threat)
- Touch the cornea (not conjunctiva) lightly with a fine wisp of cotton
- Normal: bilateral blink (direct blink = efferent CN VII; consensual blink = opposite CN VII)
Interpretation:
- Absent direct + absent consensual blink → CN V1 lesion (afferent arc)
- Absent direct + present consensual (other side) → CN VII lesion (efferent arc)
3. Motor (Muscles of Mastication)
Temporalis: Ask patient to clench teeth → palpate temporalis fullness in temple region
Masseter: Ask patient to clench jaw → palpate masseter bulk bilaterally at angles of jaw
Pterygoids: Ask patient to open mouth against resistance → jaw deviates toward the weak side (pterygoid pushes jaw to opposite side)
Jaw jerk reflex:
- Finger on chin; tap with tendon hammer
- Absent or normal in healthy adults
- Brisk jaw jerk = bilateral UMN lesion above the pons (e.g., pseudobulbar palsy)
CN VII — Facial Nerve
Anatomy
- Motor: muscles of facial expression (via stylomastoid foramen)
- Sensory: taste to anterior 2/3 tongue (via chorda tympani → lingual nerve → geniculate ganglion)
- Parasympathetic: lacrimal gland (via greater petrosal nerve), submandibular and sublingual glands (via chorda tympani)
Tests
1. Inspect at Rest and During Speech
- Look for facial asymmetry, flattening of nasolabial fold, drooping of one corner of mouth
2. Upper Face Tests
| Test | Command | What to Look For |
|---|---|---|
| Frontalis | "Raise your eyebrows" | Symmetrical forehead wrinkling |
| Orbicularis oculi | "Shut your eyes tightly, don't let me open them" | Resistance; look for Bell's phenomenon if unable to close |
3. Lower Face Tests
| Test | Command | What to Look For |
|---|---|---|
| Orbicularis oris | "Puff out your cheeks; now whistle" | Air escapes from weak side |
| Zygomaticus | "Smile / show your teeth" | Asymmetry; nasolabial fold obliteration |
| Buccinator | "Press cheek against teeth" | Weakness allows air to escape |
4. UMN vs LMN Distinction — Critical Examination Point
| Feature | UMN (Cortical/Subcortical) | LMN (Nerve/Nucleus) |
|---|---|---|
| Forehead | Spared (bilateral cortical supply) | Involved (ipsilateral weakness) |
| Lower face | Weak (contralateral) | Weak (ipsilateral) |
| Bell's phenomenon | Not present | May be present |
| Taste | Normal | Affected (if lesion proximal to chorda tympani) |
| Hyperacusis | Absent | Present (if lesion proximal to nerve to stapedius) |
| Example | Contralateral cortical stroke | Bell's palsy, parotid tumour |
Bell's phenomenon: on attempting to close the eye, the globe rolls upward and outward — protective reflex, visible when orbicularis oculi is weak (LMN CN VII palsy).
5. Taste (Anterior 2/3 Tongue)
- Place salt, sugar, vinegar, or quinine solution on tongue with cotton bud
- Test anterior tongue quadrants on each side
- Patient identifies taste without retracting tongue
- Taste loss = chorda tympani lesion (proximal to its junction with lingual nerve)
CN VIII — Vestibulocochlear Nerve
Anatomy
Two functional components:
- Cochlear (auditory): spiral ganglion → cochlear nerve → cochlear nuclei in pons → bilateral ascending pathway → auditory cortex
- Vestibular: hair cells of semicircular canals/otolith organs → vestibular nerve → vestibular nuclei in pons/medulla → connections to cerebellum, spinal cord, and CN III/IV/VI (VOR)
Tests
COCHLEAR (Hearing)
1. Bedside screening:
- Rub thumb and finger together near each ear
- Whisper numbers at 60 cm in each ear (occlude opposite ear with finger)
- Watch tests: tick heard at ≥15 cm = normal
2. Rinne Test (512 Hz tuning fork):
- Strike fork, hold base on mastoid process (bone conduction) until sound disappears
- Immediately hold vibrating tines next to ear canal (air conduction)
- Ask: "Where is it louder — before or now?"
| Result | Interpretation |
|---|---|
| AC > BC (Rinne +ve) | Normal OR sensorineural hearing loss |
| BC > AC (Rinne –ve) | Conductive hearing loss |
3. Weber Test (512 Hz tuning fork):
- Place base of vibrating fork on vertex of skull (midline)
- Ask: "Does the sound feel louder in one ear, or is it the same?"
| Result | Interpretation |
|---|---|
| Central (no lateralization) | Normal |
| Lateralizes to affected ear | Conductive hearing loss (ipsilateral) |
| Lateralizes to normal ear | Sensorineural hearing loss (contralateral) |
Mnemonic: WCSCA — Weber Conductive → Same side, Absent AC
Audiometry is required if hearing loss is detected — distinguishes type and quantifies degree.
VESTIBULAR (Balance)
1. Nystagmus: See CN III/IV/VI section
- Peripheral vestibular nystagmus: horizontal ± torsional, fatigable, inhibited by fixation
- Central vestibular nystagmus: pure vertical or direction-changing, non-fatigable, not inhibited by fixation
2. Romberg Test:
- Patient stands feet together, arms at sides, eyes open then closed
- Sways or falls with eyes closed (positive Romberg) = proprioceptive or vestibular problem (not cerebellar per se)
3. Dix-Hallpike Manoeuvre (BPPV):
- Move patient rapidly from sitting to supine with head turned 45° and extended 30° below horizontal
- Positive: delayed onset (latency 5–10 sec), brief, fatigable nystagmus = posterior canal BPPV
CN IX — Glossopharyngeal Nerve
Anatomy
- Sensory: posterior 1/3 tongue (taste + general sensation), oropharynx, tonsils, middle ear (tympanic branch = Jacobson's nerve), carotid body/sinus
- Motor: stylopharyngeus muscle
- Parasympathetic: parotid gland (via lesser petrosal nerve → otic ganglion)
- Reflex arcs: afferent limb of gag reflex; carotid sinus reflex
Tests
- CN IX and CN X are usually tested together as they share the nucleus ambiguus
Gag Reflex:
- Stimulate posterior pharyngeal wall on each side with tongue blade
- Afferent: CN IX | Efferent: CN X
- Normal: bilateral elevation of palate ± retching
- Absent bilaterally is often normal in adults — clinically meaningful only if unilateral or if correlated with other deficits
Taste (Posterior 1/3 Tongue):
- Tested as above (bitter substances) — rarely done routinely
CN X — Vagus Nerve
Anatomy
- Motor: soft palate, pharynx, larynx (via recurrent laryngeal nerve — left loops around aortic arch, right loops around subclavian)
- Sensory: ear (auricular branch), viscera
- Parasympathetic: heart, lungs, GI tract to splenic flexure
Tests
1. Palate and Uvula
- Ask patient to open mouth and say "Aah"
- Observe: soft palate rises symmetrically
- Unilateral CN X palsy: palate fails to rise on affected side; uvula deviates away from the lesion (pulled by intact side)
- Unilateral CN IX/X palsy: uvula deviates to the normal side
2. Voice Quality
- Hoarseness = laryngeal muscle weakness (recurrent laryngeal nerve)
- Bovine cough = inability to build up expiratory pressure (vocal cord palsy)
- Nasal voice = palatal weakness (air escapes through nose)
3. Swallowing
- Ask patient to swallow water; note drooling, nasal regurgitation, coughing
CN XI — Spinal Accessory Nerve
Anatomy
- Arises from upper cervical cord (C1–C5) + lower medulla
- Ascends through foramen magnum, exits via jugular foramen
- Two muscles: sternocleidomastoid (SCM) + trapezius
Tests
| Muscle | Test | Normal | Weakness Sign |
|---|---|---|---|
| Trapezius | "Shrug both shoulders" against downward resistance | Bilateral elevation, equal | Weak/absent shrug = ipsilateral CN XI |
| SCM | "Turn head to the left/right" against resistance | Strong resistance | Weakness turning head away from lesion side |
Mnemonic: Left SCM turns head to the RIGHT. Weak left SCM = difficulty turning head right.
Inspection: Wasting of trapezius → asymmetric shoulder drop; wasting of SCM → asymmetric neck contour.
CN XII — Hypoglossal Nerve
Anatomy
- Nucleus in dorsal medulla
- Exits through hypoglossal canal
- Innervates all intrinsic and extrinsic muscles of the tongue (except palatoglossus = CN X)
Tests
1. Inspection at rest:
- Look for fasciculations (fine flickering movements) = LMN lesion
- Look for atrophy (wasting, scalloped edges, thinning)
2. Tongue protrusion:
- "Stick out your tongue"
- Normal: midline protrusion
- Deviation toward the weak side (the intact genioglossus pushes the tongue toward the paralyzed side)
3. Tongue strength:
- "Push your tongue into your cheek" — examiner pushes from outside
- Test both sides
4. Rapid tongue movements:
- "Say la-la-la quickly" (tests tongue tip) — dysarthria if CN XII paresis
UMN vs LMN CN XII:
| Feature | UMN | LMN |
|---|---|---|
| Atrophy | Absent | Present |
| Fasciculations | Absent | Present |
| Tone | Spastic (stiff tongue) | Flaccid (soft tongue) |
| Deviation | Away from lesion side | Toward lesion side |
| Example | Contralateral hemisphere stroke | Motor neuron disease, hypoglossal canal tumour |
Bulbar vs. Pseudobulbar Palsy
| Feature | Bulbar Palsy (LMN) | Pseudobulbar Palsy (UMN) |
|---|---|---|
| Site | CN IX, X, XII nuclei or nerves | Bilateral corticobulbar tracts |
| Voice | Nasal, hoarse, quiet | High-pitched, strangled ("Donald Duck") |
| Tongue | Wasted, fasciculating | Small, spastic |
| Jaw jerk | Normal or absent | Brisk |
| Gag reflex | Absent | Exaggerated |
| Emotion | Normal | Emotional lability (pathological laughing/crying) |
| Example | MND (LMN), Guillain-Barré, syringobulbia | Stroke (bilateral), MND (UMN), MS |
Quick Summary Table
| CN | Name | Modality | Key Test | Key Sign if Lesion |
|---|---|---|---|---|
| I | Olfactory | Sensory | Identify odorant | Anosmia |
| II | Optic | Sensory | Snellen, fields, fundoscopy, RAPD | Visual loss, RAPD, field defect |
| III | Oculomotor | Motor + Para | Pupil reflex, EOM, ptosis | Ptosis, dilated pupil, "down & out" |
| IV | Trochlear | Motor | Depression in adduction | Diplopia going down stairs, head tilt |
| V | Trigeminal | Sensory + Motor | Pin, cotton, corneal reflex, jaw clench | Facial numbness, absent corneal reflex |
| VI | Abducens | Motor | Lateral gaze | Failure to abduct, horizontal diplopia |
| VII | Facial | Motor + Sensory | Raise brows, close eyes, smile | UMN = lower face; LMN = whole face |
| VIII | Vestibulocochlear | Sensory | Whisper, Rinne, Weber, Romberg | Deafness, vertigo, nystagmus |
| IX | Glossopharyngeal | Sensory + Motor | Gag reflex (afferent) | Absent gag, lost taste posterior tongue |
| X | Vagus | Motor + Para | Palate "aah", voice, swallowing | Uvula deviates away, hoarse, dysphagia |
| XI | Spinal Accessory | Motor | Shoulder shrug, head rotation | Weak shrug, difficulty turning head |
| XII | Hypoglossal | Motor | Tongue protrusion, strength | Deviation toward lesion, atrophy (LMN) |
Important Clinical Syndromes
| Syndrome | CNs Involved | Site |
|---|---|---|
| Cavernous sinus | III, IV, V1/V2, VI, Horner | Cavernous sinus |
| Superior orbital fissure | III, IV, V1, VI | Orbital fissure |
| Orbital apex | II + III, IV, V1, VI | Orbital apex |
| CPA (cerebellopontine angle) | V, VII, VIII | Posterior fossa |
| Jugular foramen (Vernet) | IX, X, XI | Jugular foramen |
| Collet-Sicard | IX, X, XI, XII | Retroparotid space |
| Paratrigeminal (Raeder) | V + Horner | Middle fossa |
| Millard-Gubler | VI, VII (ipsi) + hemiplegia (contra) | Pons |
| Wallenberg (PICA) | V, IX, X (ipsi) + spinothalamic (contra) | Lateral medulla |
Sources: Adams and Victor's Principles of Neurology, 12th Ed; Harrison's Principles of Internal Medicine, 22E (2025, McGraw Hill); Goldman-Cecil Medicine, International Edition.
This is a shared conversation. Sign in to Orris to start your own chat.