Metabolic response to injury chapter 1 in unit 1 of barley and love text book with clear explaining in exam point of view
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a complete, exam-focused explanation. Here is the full chapter breakdown:
Metabolic Response to Injury - Chapter 1, Bailey & Love's Short Practice of Surgery (28th Edition)
1. INTRODUCTION - What Is the Metabolic Response to Injury?
When the body suffers significant tissue damage (from surgery or accidental trauma), it responds with a series of systemic changes affecting vital organ function. This is called the surgical stress response or metabolic response to injury.
Pathways involved:
- Hormonal (neuroendocrine)
- Inflammatory (cytokines)
- Neural circuits
Effects include:
- Altered body metabolism
- Changes in wound healing and immunity
- Specific organ dysfunction
Exam point: If uncontrolled, this response leads to sepsis → MODS (multiple organ dysfunction syndrome). MODS carries ~25% mortality even in modern trauma systems.
2. HOMEOSTASIS AND THE TWO PHASES
Homeostasis = maintaining a constant internal environment for optimal cellular function.
The metabolic response is classically divided into two phases:
| Feature | Catabolic (Ebb) Phase | Anabolic (Flow) Phase |
|---|---|---|
| Timing | Immediately after injury (0-48 hrs) | After resuscitation |
| Metabolic rate | Decreased | Increased (hypermetabolism) |
| Cardiac output | Reduced | Increased |
| Temperature | Hypothermia | Fever |
| Key hormones | Catecholamines, cortisol, aldosterone | Insulin (with resistance) |
| Purpose | Conserve volume and energy | Mobilise stores for repair |
Exam point: The catabolic phase is also called the "ebb" phase and the anabolic flow phase corresponds to SIRS (systemic inflammatory response syndrome).
3. MAGNITUDE OF THE INJURY RESPONSE
The metabolic response is graded - more severe injury = greater response.
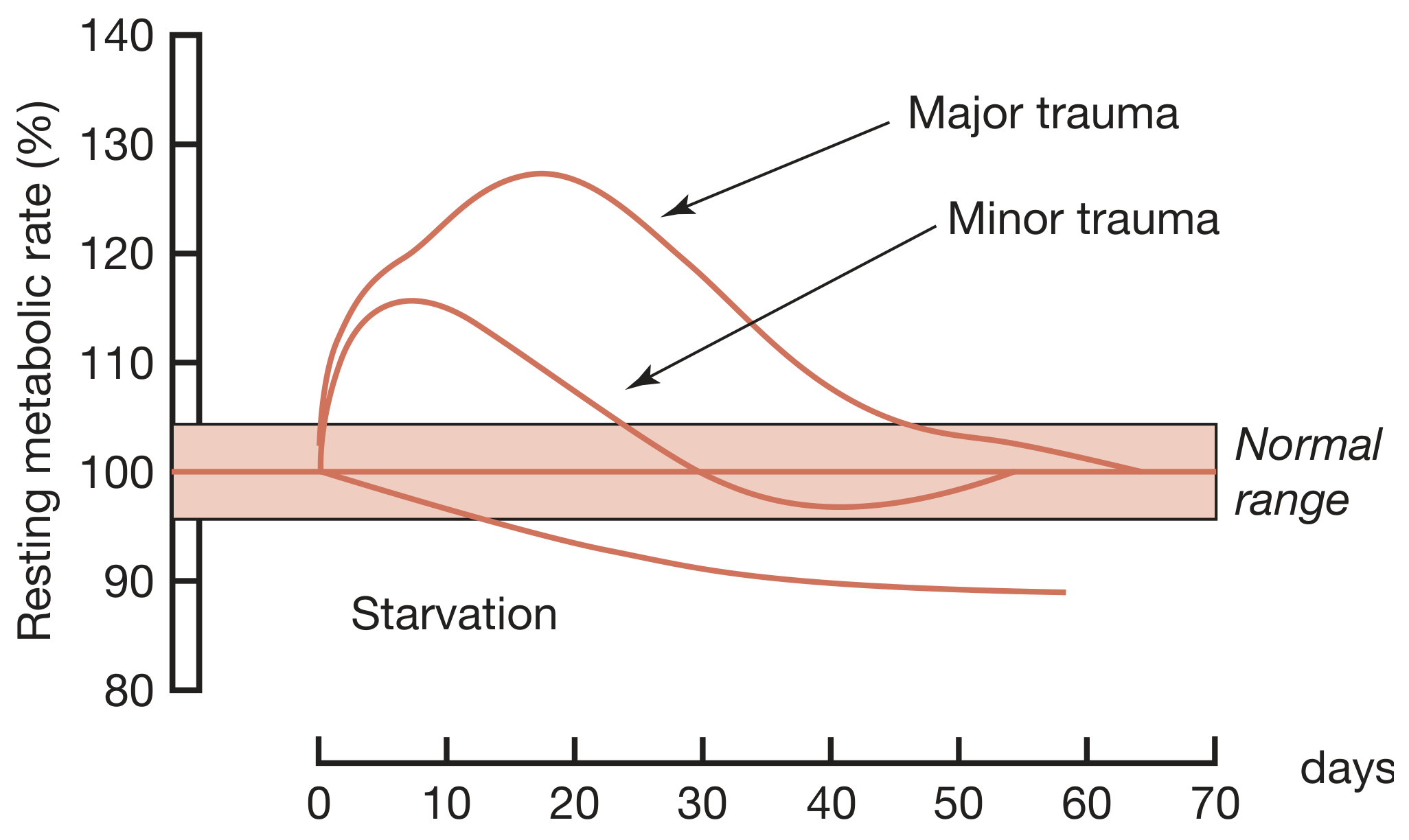
Resting metabolic rate rises proportionally with injury severity. Major trauma peaks around day 10-15 at ~128% of normal.
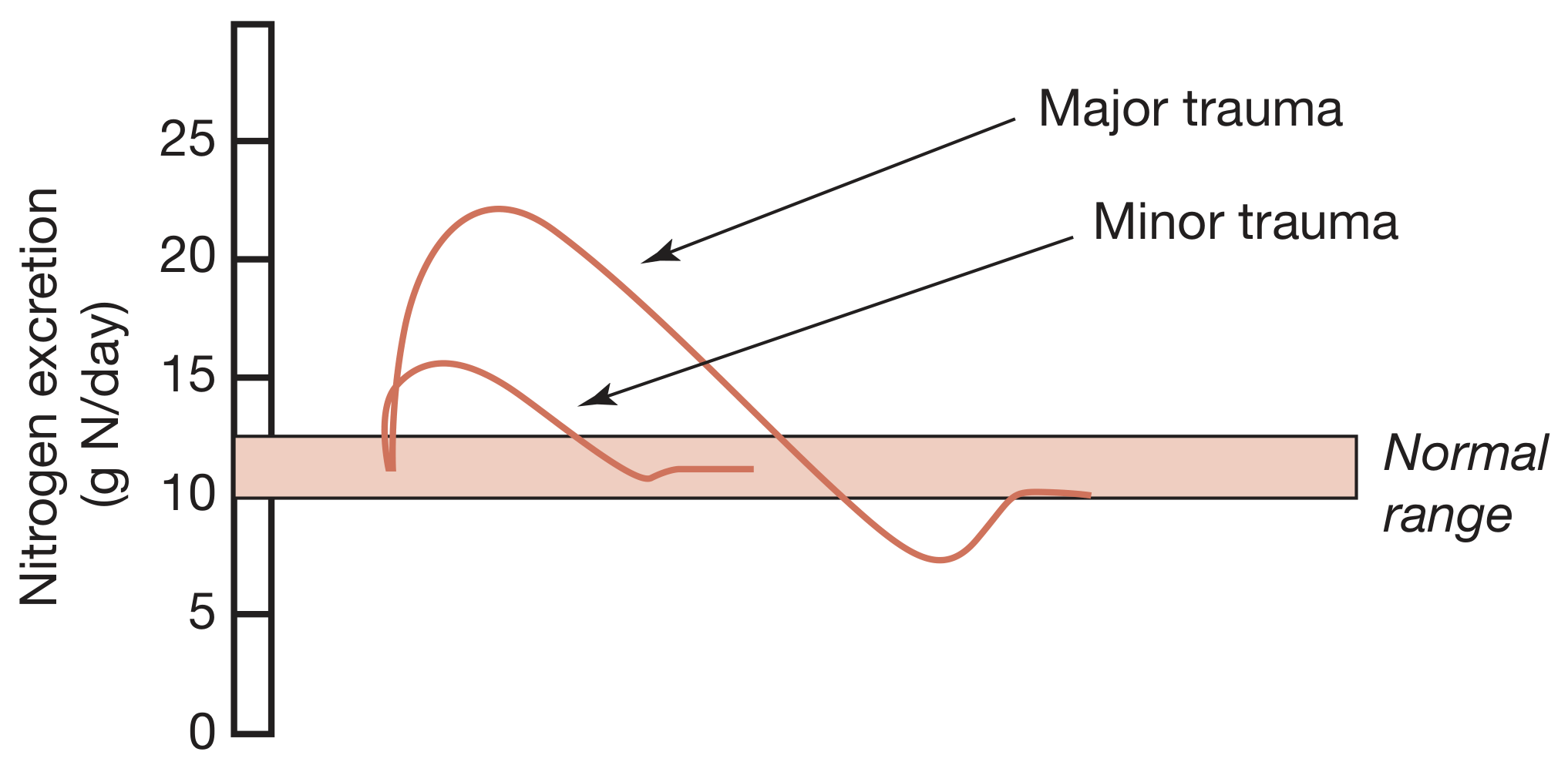
Urinary nitrogen excretion rises to ~22 g N/day in major trauma vs ~15 g N/day in minor trauma, reflecting protein catabolism.
Examples of graded responses:
- Minor elective surgery: transient modest rise in temperature, HR, RR, WBC, energy expenditure
- Major trauma/burns/sepsis: SIRS, hypermetabolism, marked catabolism, shock, MODS
Exam point: Genetic variability also determines response intensity - some patients respond much more dramatically than others to similar injuries.
4. MEDIATORS OF THE METABOLIC RESPONSE
A. Tissue Damage and Inflammation (DAMPs Pathway)
Step-by-step pathway:
- Tissue injury releases DAMPs (damage-associated molecular patterns), also called alarmins
- Examples: heat shock proteins, HMGB1 (high mobility group protein B1), S100 proteins, nucleic acid fragments
- DAMPs activate PRRs (pattern recognition receptors):
- Toll-like receptors (TLRs)
- NOD-like receptors (NLRs)
- Found on: macrophages, neutrophils, dendritic cells
- PRR activation triggers formation of inflammasomes (complex intracellular proteins)
- Inflammasomes activate caspases → activate key cytokines:
- IL-1, IL-6, TNF-alpha, IL-8, interferons, chemokines
- Result: sterile systemic inflammatory cascade → local inflammation → SIRS
Key consequences of DAMPs on endothelium and platelets:
- Leaky capillaries (oedema)
- Coagulopathy
- Local ischaemia → more DAMPs (self-perpetuating cycle)
Secondary triggers that amplify/prolong the response (Table 1.1):
- Sepsis
- Haemorrhage
- Massive transfusion
- Acidosis
- Surgery itself
- Crush syndrome
- Ischaemia-reperfusion injury
Exam point: The "redundancy" of DAMPs (ability to activate multiple receptors/pathways) is why therapeutic blockade of inflammation has been so difficult clinically.
B. Neuroendocrine Response to Injury
The classic pathway:
Tissue injury/pain
↓
Afferent nociceptive neurones
↓
Spinal cord → Thalamus → Hypothalamus
↓
CRF (corticotropin-releasing factor) released
↓
ACTH from anterior pituitary
↓
Adrenal cortex → CORTISOL (within hours)
Hypothalamus also activates:
→ Sympathetic nervous system → ADRENALINE (epinephrine)
→ Pancreas → GLUCAGON
The "counter-regulatory hormones" triad:
- Glucocorticoids (cortisol)
- Glucagon
- Catecholamines (adrenaline)
High-yield exam fact: IV infusion of these three hormones reproduces many aspects of the metabolic response to injury.
Other hormonal changes:
- Growth hormone (GH) ↑ - but paradoxically with low IGF-1; GH has direct lipolytic, insulin-antagonising and pro-inflammatory properties
- Prolactin ↑
- Peripheral thyroid hormones inactivated
- Gonadal function suppressed
The neuroendocrine response is BIPHASIC (Summary Box 1.2):
| Phase | Timing | Features |
|---|---|---|
| Acute | Hours | Elevated counter-regulatory hormones (cortisol, glucagon, adrenaline) - beneficial for short-term survival |
| Chronic | Days | Hypothalamic suppression, low serum target organ hormones - contributes to chronic wasting |
C. Cytokines and Their Actions
Proinflammatory cytokines (IL-1, TNFα, IL-6, IL-8) produced within first 24 hours:
| Cytokine | Key Action |
|---|---|
| IL-1 | Pyrexia (acts on hypothalamus), augments stress response |
| TNFα | Pyrexia, promotes proteolysis in muscle |
| IL-6 | Major driver of hepatic acute-phase protein response |
| IL-8 | Neutrophil chemotaxis |
Exam point: IL-6 is the primary driver of the hepatic acute-phase protein response.
D. Agonists and Antagonists: An Uncertain Balance
The inflammatory response involves counter-regulatory (anti-inflammatory) mediators as well:
- IL-10, IL-4, TGF-beta (anti-inflammatory)
- Glucocorticoids also have anti-inflammatory effects
This balance between pro- and anti-inflammatory mediators determines whether SIRS progresses to MODS or resolves.
Exam point: CARS (Compensatory Anti-inflammatory Response Syndrome) can lead to immune suppression if the anti-inflammatory arm is too dominant, predisposing to secondary infections.
5. METABOLIC CHANGES AFTER SURGERY AND TRAUMA
Catabolic Phase (0-48 hours)
- Hypovolaemia, ↓ BMR, ↓ cardiac output, hypothermia, lactic acidosis
- Dominant hormones: catecholamines, cortisol, aldosterone
- Insulin levels fall or do not rise appropriately → hyperglycaemia
Flow Phase (after resuscitation - corresponds to SIRS)
Features:
- Tissue oedema (vasodilatation + ↑ capillary permeability)
- Hypermetabolism (↑ BMR)
- ↑ Cardiac output
- Raised body temperature
- Leukocytosis
- ↑ Oxygen consumption
- ↑ Gluconeogenesis
Purpose of neuroendocrine changes (Summary Box 1.4):
- Provide essential substrates for survival via tissue breakdown
- Postpone anabolism
- Optimise host defence
Exam point: These changes are helpful short-term but harmful long-term, especially in the critically ill.
The vicious catabolic cycle:
Catabolism + insulin resistance → hyperglycaemia → ↑ risk of sepsis → further neuroendocrine/inflammatory stimulation → worsened catabolism
6. MANAGING THE CATABOLIC RESPONSE
The body does not catabolise uniformly - it reprioritises resources:
- Catabolic (peripheral) tissues: skeletal muscle, adipose tissue, skin
- Anabolic (central) tissues: liver, immune system, wound
A. Hypermetabolism
- Most trauma patients: energy expenditure 15-25% above predicted resting values
- Burns patients can go even higher
- Caused by: central thermodysregulation (cytokine cascade), ↑ sympathetic activity, ↑ protein turnover, wound circulation abnormalities (Cori cycle)
B. Skeletal Muscle Protein Metabolism
Normal: protein synthesis = breakdown (turnover 1-2%/day)
After injury: breakdown > synthesis → net muscle wasting
Mechanism of muscle wasting:
- ↑ Protein degradation via the ubiquitin-proteasome pathway (key exam fact)
- ↓ Protein synthesis
Consequences of muscle wasting:
- Loss of respiratory muscle → hypoventilation, chest infections
- Loss of gut muscle → ↓ gut motility
- Amino acids (especially glutamine and alanine) exported from muscle to liver (for gluconeogenesis) and wound
- Net catabolism occurs because alanine and glutamine are derived partly from irreversible degradation of branched-chain amino acids
Summary Box 1.5 - Skeletal muscle wasting:
- Provides amino acids for central organs/tissues
- Mediated mainly by ubiquitin-proteasome pathway
- Inevitable to some degree, prolonged by sepsis
- Can cause immobility, poor healing, hypostatic pneumonia, death if excessive
C. Acute-Phase Protein Response (Hepatic)
IL-6 (primarily) drives the liver to reprioritise protein synthesis:
| Acute-Phase Proteins | Direction | Examples |
|---|---|---|
| Positive reactants | ↑ | CRP, fibrinogen, alpha-1 antitrypsin |
| Negative reactants | ↓ | Albumin, transferrin, pre-albumin |
Exam point: Albumin falls after injury NOT mainly due to reduced synthesis, but due to increased transcapillary escape (3x increase in TER) secondary to microvascular permeability changes. Normal albumin TER is already ~10x the synthesis rate.
The acute-phase response is a "double-edged sword" - provides proteins needed for repair but at the cost of lean tissue and energy.
D. Insulin Resistance
After injury:
- Glucose production ↑ (gluconeogenesis)
- Glucose uptake in peripheral tissues ↓
- Mechanism: proinflammatory cytokines + decreased responsiveness of insulin-regulated glucose transporter proteins
- Degree of resistance is proportional to injury magnitude
Clinically:
- After routine upper abdominal surgery: insulin resistance persists ~2 weeks
- With prolonged sepsis: extends further
- Behaves like Type 2 diabetes mellitus
- Management in ICU: IV insulin infusion to maintain blood glucose within limits
- Caution: tight control risks significant hypoglycaemia
7. CHANGES IN BODY COMPOSITION FOLLOWING INJURY
A standard 70 kg male has:
- Fat: 13 kg
- Fat-free mass (protein + water): ~57 kg
After major surgery/critical illness:
- Fat mass ↓
- Skeletal muscle mass ↓
- Body weight may paradoxically increase due to expansion of extracellular fluid (oedema)
Summary Box 1.7:
- Catabolism decreases fat mass and skeletal muscle mass
- Body weight may increase paradoxically due to extracellular fluid expansion
8. AVOIDABLE FACTORS THAT COMPOUND THE RESPONSE
Summary Box 1.8 - Avoidable factors (must know for exams):
| Factor | Mechanism |
|---|---|
| Volume loss / haemorrhage | Activates ADH, RAAS → salt/water retention |
| Hypothermia | Amplifies catabolism, impairs coagulation |
| Tissue oedema | Impairs oxygen delivery, delays healing |
| Systemic inflammation / underperfusion | Perpetuates SIRS, promotes MODS |
| Starvation | Muscle breakdown for energy, immune compromise |
| Immobility | Muscle wasting, DVT, pneumonia |
Volume loss in detail:
- Baroreceptors (carotid, aortic arch) + volume receptors (left atrium) → CNS → ADH + aldosterone release
- ADH → fluid retention at kidney
- ↓ Pulse pressure → juxtaglomerular apparatus → renin-angiotensin → ↑ aldosterone
- Aldosterone → Na+ reabsorption → water conservation
- Net effect: oliguria after surgery (normal/expected)
- Excess saline resuscitation worsens salt/water retention → peripheral AND visceral oedema → delayed gastric emptying, prolonged hospital stay
9. ENHANCED RECOVERY AFTER SURGERY (ERAS)
Modern understanding of the metabolic response has driven ERAS (Enhanced Recovery After Surgery) protocols.
Goal: Actively reduce the need for a homeostatic response by minimising the primary insult.
Summary Box 1.9 - ERAS key elements:
- Minimal access techniques (laparoscopic surgery)
- Blockade of afferent pain stimuli (epidural analgesia, spinal, wound catheters)
- Note: epidural analgesia is no longer recommended for laparoscopic surgery (patient-controlled analgesia is sufficient)
- Minimal periods of starvation (avoid prolonged preoperative fasting)
- Early mobilisation
Benefits of ERAS:
- Reductions in length of hospital stay of 30-50%
- Improved outcomes
- Reduced healthcare costs
Other modulating strategies:
- Beta-blockers: associated with improved short- and long-term survival after major surgery (by modulating the hyper-adrenergic state)
- Epidural analgesia in open surgery: reduces pain, blocks cortisol stress response, attenuates postoperative insulin resistance
- IV lidocaine infusion (6-12 hr): opioid-sparing, improves gut function
- 'One-shot' spinal diamorphine: opioid-sparing effect
HIGH-YIELD EXAM SUMMARY
| Topic | Key Point |
|---|---|
| Two phases of metabolic response | Catabolic (ebb) → Anabolic (flow/SIRS) |
| Initiating molecules | DAMPs activate PRRs → inflammasomes → caspases → IL-1, IL-6, TNFα |
| Counter-regulatory hormone triad | Cortisol + Glucagon + Catecholamines |
| Muscle wasting pathway | Ubiquitin-proteasome pathway |
| Why albumin falls | Increased transcapillary escape (NOT reduced synthesis) |
| Driver of acute-phase response | IL-6 (mainly) |
| Insulin resistance duration | ~2 weeks after upper abdominal surgery |
| Paradox of body weight | Weight may increase despite catabolism (due to oedema) |
| MODS mortality | ~25% |
| ERAS hospital stay benefit | 30-50% reduction |
| GH after injury | ↑ GH but low IGF-1; GH is lipolytic and insulin-antagonising |
| Why DAMP blockade fails clinically | Redundancy - DAMPs activate multiple receptors/pathways |
| Epidural - when NOT used | Not recommended for laparoscopic surgery |
Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 1, pp. 22-35
This is a shared conversation. Sign in to Orris to start your own chat.