Status epilepticus
Reading File
Finding Sources
Reading File
Searching PubMed
"status epilepticus" management treatment
Reading File
Reading File
Running Command
Running Command
Reading File
Reading File
Running Command
Loading Image
Running Command
Reading File
Running Command
Loading Image
Finding Sources
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full response:
Status Epilepticus
Definition
Status epilepticus (SE) is defined as a single seizure lasting ≥5 minutes, or two or more seizures without recovery of consciousness between them. After 5 minutes, seizures are:
- Less likely to terminate spontaneously
- Less likely to respond to antiepileptic drugs
- More likely to cause neuronal damage
Subtypes by duration:
| Type | Duration |
|---|---|
| Established SE | ≥5 min |
| Refractory SE | Persists despite 2 appropriately dosed anti-seizure therapies |
| Super-refractory SE | Persists ≥24 hours despite anesthetic coma (including when seizures recur on anesthetic withdrawal) |
SE is a neurologic emergency — treatment must begin within 5 minutes of onset. — Tintinalli's Emergency Medicine
Etiology
Common causes include:
- Subtherapeutic antiepileptic drug (AED) levels (most common in known epileptics)
- Acute stroke / anoxia / hypoxia
- CNS infection (bacterial meningitis, viral encephalitis)
- Metabolic disturbances (hypoglycemia, hyponatremia, hypocalcemia, hypomagnesemia)
- Head trauma
- Alcohol or drug intoxication/withdrawal
- Autoimmune encephalitis (e.g., NMDA receptor antibody)
- Eclampsia / posterior reversible encephalopathy syndrome (PRES)
- Cortical venous thrombosis
Pathophysiology
Two critical molecular shifts occur as SE progresses:
- ≥5 minutes: Internalization/decreased expression of GABA-A receptors + upregulation of glutamate/NMDA receptors → markedly reduced seizure threshold and pharmacoresistance
- Blood-brain barrier breakdown: CNS penetration of potassium and albumin (both hyperexcitatory)
After 20 minutes, systemic complications develop:
- Hypotension, hypoxia
- Metabolic acidosis
- Hyperthermia
- Hypoglycemia
- Cardiac dysrhythmias
- Pulmonary edema
This milieu makes standard anti-seizure therapies far less effective. — Tintinalli's Emergency Medicine, p. 1199
Nonconvulsive SE (NCSE)
- Patient is comatose or has fluctuating/altered mental status — no overt convulsions
- Subtle signs: eye deviation, blinking, twitching
- Diagnosis requires EEG (often continuous)
- Suspect in: prolonged postictal period, unexplained stupor/confusion
- Delays in diagnosis worsen mortality, especially in patients >60 years or without prior seizure disorder
Initial Stabilization (0–5 minutes)
Simultaneously:
- Position to maximize ventilation, prevent aspiration; immobilize cervical spine if trauma suspected
- Airway: Nasopharyngeal airway preferred (oral airway provokes vomiting on seizure resolution); bag-valve-mask if ventilation inadequate
- Oxygen via nasal cannula or face mask
- Large-bore IV access (or IO if IV unavailable within 1–2 min)
- Cardiac monitor, pulse oximetry, continuous temperature monitoring
- Bedside glucose — administer D50W (adults) or D10W (children, 5 mL/kg) if glucose <60 mg/dL; give thiamine 100 mg IV first in adults at risk
- Treat hyperthermia (antipyretics + cooling blankets)
Labs: Electrolytes, glucose, calcium, magnesium, lactate, CBC, LFTs, renal function, AED levels (if applicable), pregnancy test, toxicology screen
Do not attempt lumbar puncture during active SE. If meningitis/encephalitis is suspected, start empiric antibiotics/antivirals immediately without waiting for LP.
Treatment Algorithm
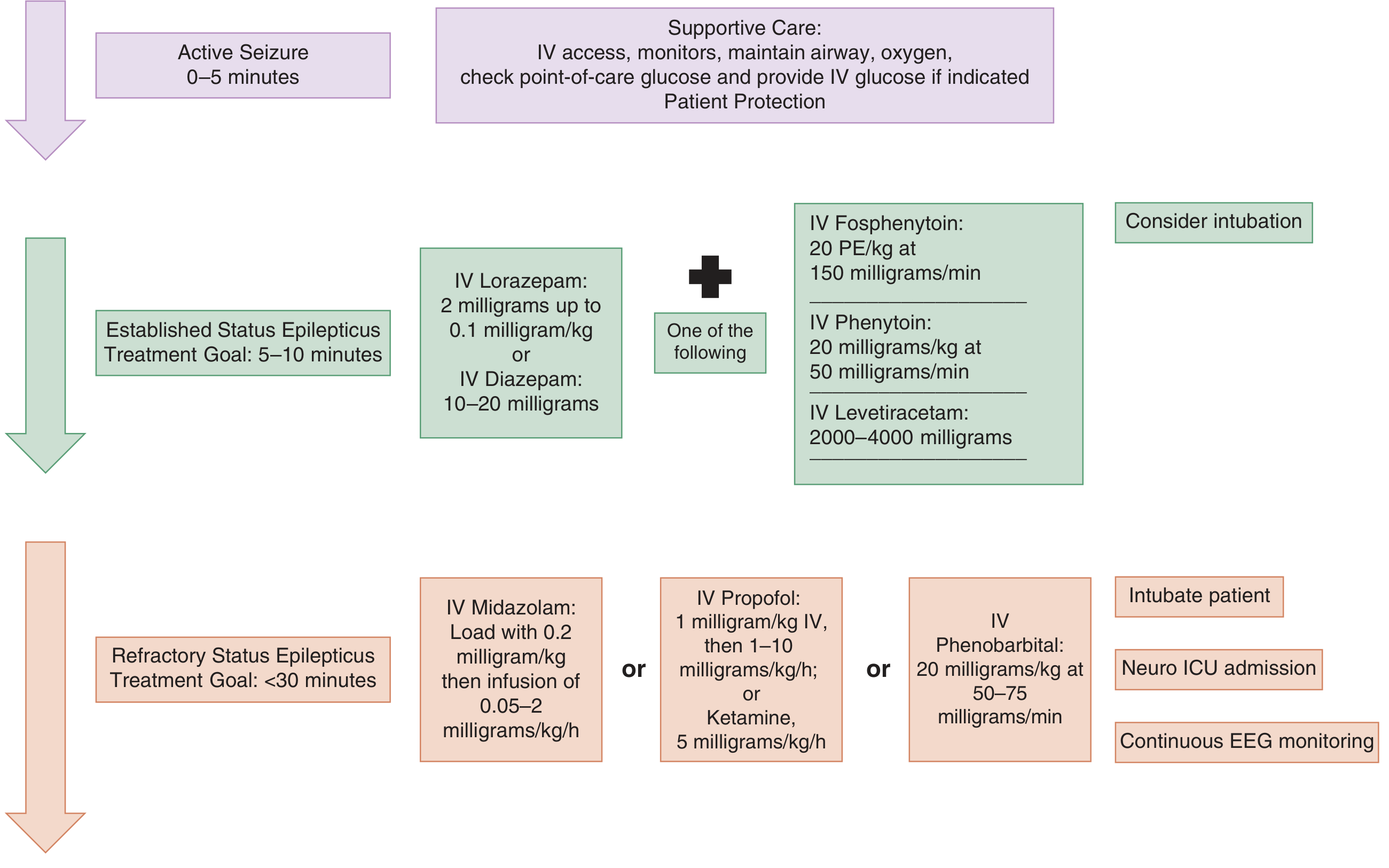
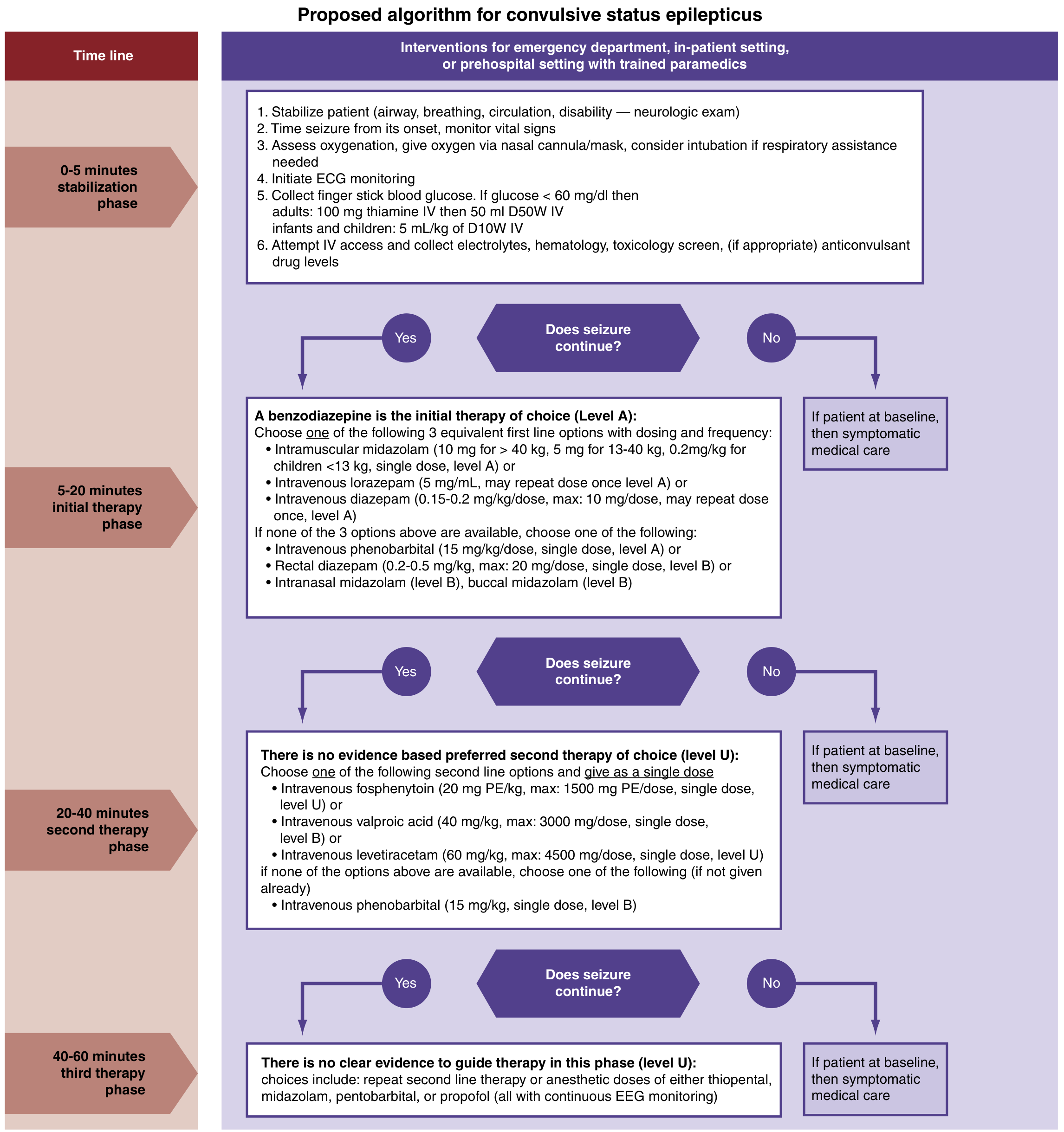
Phase 1: Initial Therapy (5–20 min) — Benzodiazepines (Level A)
First-line: Benzodiazepines terminate SE ~70% of the time by enhancing GABA-A activity.
Delays in benzodiazepine initiation >10 minutes are associated with higher mortality, longer seizure duration, and more complications. — Rosen's Emergency Medicine
| Drug | Route | Adult dose | Pediatric dose |
|---|---|---|---|
| Lorazepam (preferred if IV available) | IV | 2–4 mg (0.1 mg/kg) | 0.1 mg/kg IV (max 4 mg) |
| Midazolam (preferred if no IV) | IM | 10 mg (>40 kg) | 0.2 mg/kg (<13 kg); 5 mg (13–40 kg) |
| Diazepam | IV | 5–10 mg (0.15–0.2 mg/kg) | 0.2–0.5 mg/dose (< 5 yr); 1 mg/dose (≥5 yr) |
| Diazepam | Rectal | — | 0.5 mg/kg (max 20 mg) |
| Midazolam | Intranasal/buccal | — | Level B evidence |
| Phenobarbital | IV | — | 15 mg/kg single dose (if above unavailable) |
- A second dose of benzodiazepine may be given after 5 minutes of continued seizure activity
- Lorazepam vs. diazepam: Lorazepam has a slightly slower onset (3 vs. 2 min) but dramatically longer duration (12–24 h vs. 15–60 min) and fewer recurrences
- IM midazolam was non-inferior to IV lorazepam in prehospital trials — preferred when no IV access
Phase 2: Second-Line Therapy (20–40 min) — No evidence-based preference among agents (Level U)
If seizure persists after benzodiazepines:
| Drug | Dose | Notes |
|---|---|---|
| Fosphenytoin (preferred over phenytoin) | 20 PE/kg IV at 150 PE/min (max 1500 PE) | Water-soluble phenytoin prodrug; can give IM; less cardiotoxic; infuses 3× faster |
| Levetiracetam | 60 mg/kg IV (max 4500 mg) | Fewer adverse events vs. phenytoin in some trials; no significant difference in seizure termination in controlled trials |
| Valproic acid | 40 mg/kg IV (max 3000 mg) | Contraindicated in liver disease, thrombocytopenia, suspected metabolic disease |
| Phenytoin | 20 mg/kg IV at ≤50 mg/min | Cardiotoxic; infusion-site reactions; not compatible with glucose solutions |
| Phenobarbital | 15 mg/kg IV | Alternative if others unavailable |
Current consensus guidelines do not recommend one second-line agent over the others. If seizures persist after first second-line agent, a second second-line agent may be tried before escalating to anesthetic therapy. — Tintinalli's/Rosen's
Phase 3: Refractory SE (40–60 min) — Anesthetic / Third-Line (Level U)
Requires: Endotracheal intubation + continuous EEG monitoring + Neuro ICU admission
Choose one anesthetic agent:
| Drug | Dose |
|---|---|
| Midazolam infusion | Load 0.2 mg/kg IV, then 0.05–2 mg/kg/h infusion |
| Propofol infusion | 1 mg/kg IV bolus, then 1–10 mg/kg/h |
| Phenobarbital | 20 mg/kg IV at 50–75 mg/min |
| Ketamine | 5 mg/kg/h (adjunct; evidence limited to case reports) |
All third-line agents cause apnea, depressed consciousness, and hypotension — effects more pronounced in the presence of benzodiazepines. Continuous cardiorespiratory monitoring is mandatory. — Rosen's Emergency Medicine
Intubation notes: Use a short-acting neuromuscular blocker (e.g., succinylcholine) to allow monitoring of continued seizure activity. If sedative required for intubation, select one with antiepileptic activity (propofol, ketamine).
Super-Refractory SE (≥24 h despite anesthetics)
No established therapies. Options reported in literature:
- Repeat/titrate second-line agents
- Pentobarbital coma
- Thiopental
- Inhalant anesthetics
- Plasmapheresis (scoping review data only)
- Electroconvulsive therapy (ECT)
- Ketogenic diet
Mortality ~3%; survivors face significant morbidity (recurrent seizures, cognitive-behavioral impairment). — Rosen's/Katzung's
Post-Seizure Workup (after SE terminated)
- Neuroimaging (CT or MRI) to identify structural cause
- Lumbar puncture if CNS infection or autoimmune encephalitis suspected
- Continuous EEG — especially after neuromuscular blockade to detect ongoing nonconvulsive SE
- Identify and correct the underlying etiology
Special Populations
Pediatric SE
- Benzodiazepine protocol is the same; weight-based dosing critical
- Buccal midazolam is more effective than rectal diazepam in children
- Valproic acid contraindicated if possible metabolic disease (mitochondrial disorders)
- Neurology consultation strongly recommended for refractory pediatric SE
- Harriet Lane Handbook diazepam rectal dosing: 0.5 mg/kg (2–5 yr), doses rounded to nearest 2.5 mg increment
Pregnancy (eclampsia-associated SE)
- Magnesium sulfate is first-line for eclamptic SE (not a standard AED — acts via NMDA receptor antagonism)
- Phenobarbital or lorazepam/midazolam acceptable for non-eclamptic SE in pregnancy
- Avoid valproic acid (teratogenic, especially first trimester)
- Common causes in pregnancy: eclampsia, PRES, cortical venous thrombosis, NMDA-receptor encephalitis
Prognosis
- Outcome strongly determined by underlying etiology and duration before treatment
- Mortality dramatically increases with delayed diagnosis/treatment
- Worst prognosis: no prior seizure disorder, age >60, nonconvulsive SE
- ~60% good outcome in refractory SE in pregnancy; ~50% fetal survival (retrospective data) — Bradley & Daroff's Neurology
Recent Evidence
Three 2024 systematic reviews are available:
- Stiripentol for prevention/cessation of SE — systematic review (Specchio et al., Epilepsia Open 2024; PMID 39360600)
- Clinical practice guidelines for SE management in adults — systematic review of guidelines (Vignatelli et al., Epilepsia 2024; PMID 38606469)
- Surgical management of SE — systematic review (Jha et al., Epilepsia Open 2024; PMID 38456595)
Sources: Tintinalli's Emergency Medicine (9e), Rosen's Emergency Medicine, Katzung's Basic & Clinical Pharmacology (16e), Harriet Lane Handbook (23e), Bradley & Daroff's Neurology in Clinical Practice; AES Guideline (Glauser et al., Epilepsy Curr. 2016)
This is a shared conversation. Sign in to Orris to start your own chat.