Ceohalosporin pharmacology details
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from both Katzung's and Lippincott's. Let me compile the full detailed answer.
Cephalosporin Pharmacology
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed.; Lippincott Illustrated Reviews: Pharmacology
1. Structure & Classification
Cephalosporins are semi-synthetic beta-lactam antibiotics derived from 7-aminocephalosporanic acid. The core bicyclic structure consists of a beta-lactam ring fused to a dihydrothiazine ring (vs. the thiazolidine ring in penicillins).
- Position 7 (acyl side chain): determines antibacterial spectrum and beta-lactamase stability
- Position 3: determines pharmacokinetic profile (half-life, protein binding, route)
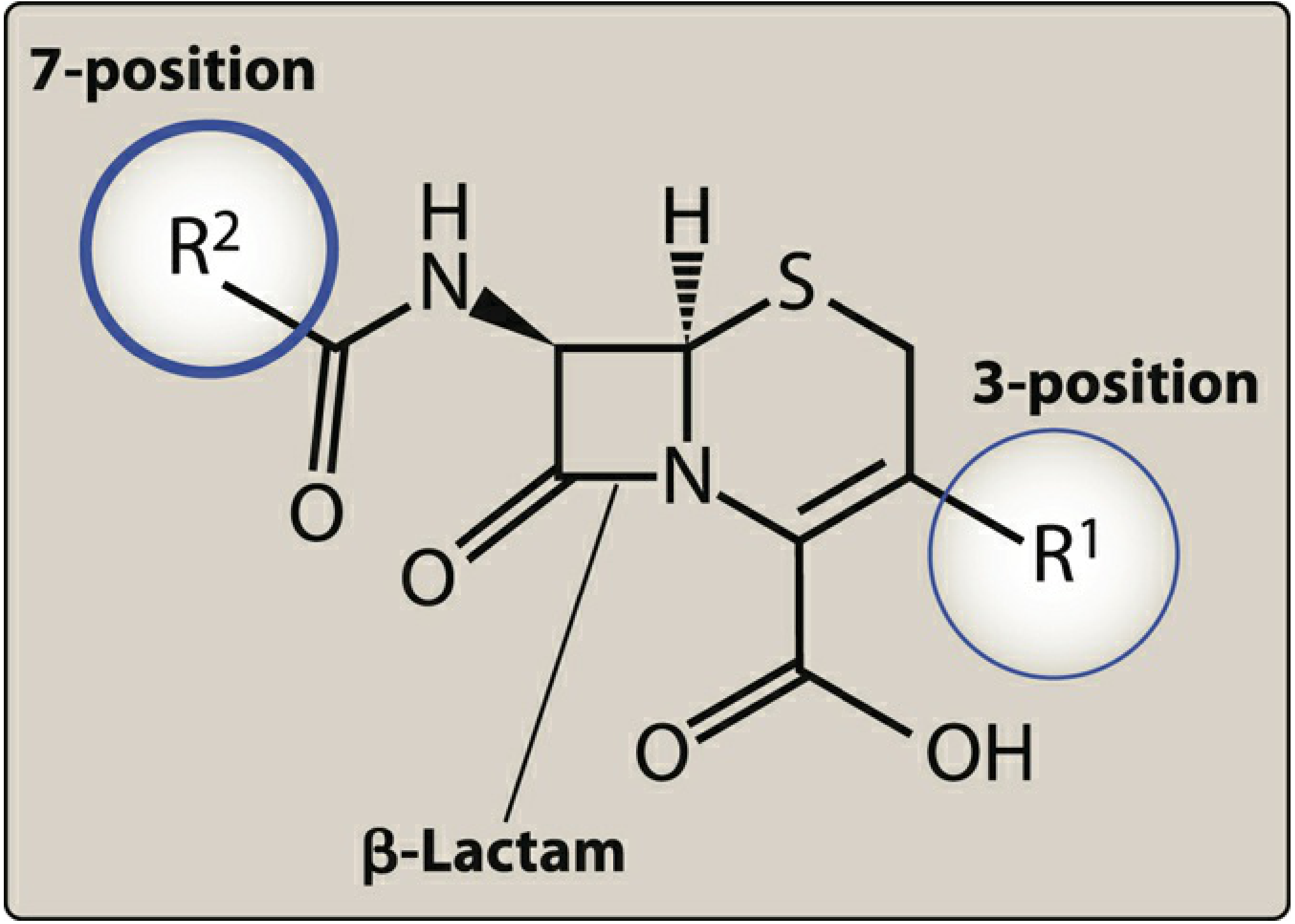
Figure: Structural features of cephalosporin antibiotics - the 7-position side chain governs activity, the 3-position governs PK (Lippincott Illustrated Reviews: Pharmacology)
2. Mechanism of Action
Same as all beta-lactams:
- Bind penicillin-binding proteins (PBPs) - bacterial enzymes (transpeptidases, carboxypeptidases) involved in cross-linking the peptidoglycan cell wall
- Inhibit transpeptidation - the final cross-linking step of peptidoglycan synthesis
- Result: structural weakening of the cell wall → bactericidal (cell lysis via autolysins)
- Activity is time-dependent: efficacy correlates with time the free drug concentration exceeds the MIC (fT > MIC)
3. Resistance Mechanisms
Three major mechanisms (Lippincott):
| Mechanism | Details |
|---|---|
| Beta-lactamase production | Enzymes hydrolyze the beta-lactam ring. Gram-positives secrete them extracellularly; gram-negatives hydrolyze in the periplasmic space. Includes chromosomal (AmpC, often inducible by 2nd/3rd gen agents) and plasmid-mediated (ESBLs, KPC, MBL) enzymes |
| Decreased permeability | Reduced or absent outer membrane porins (especially in gram-negatives like P. aeruginosa). Efflux pumps (e.g., in K. pneumoniae) actively remove drug |
| Altered PBPs | Modified PBPs have lower affinity for beta-lactams. Classic example: MRSA - mecA gene produces PBP2a, which is resistant to most commercially available beta-lactams |
4. Generations: Spectrum and Key Agents
First Generation
Drugs: Cefazolin (IV), Cephalexin (PO), Cefadroxil (PO)
Spectrum:
- Excellent gram-positive coverage: S. aureus (MSSA), S. epidermidis, S. pneumoniae, S. pyogenes, anaerobic streptococci
- Limited gram-negative: E. coli, K. pneumoniae, Proteus mirabilis (the "3 EKPs")
- No activity against MRSA, enterococci, Pseudomonas, Enterobacter, Serratia, B. fragilis
Key uses:
- Cefazolin: surgical prophylaxis (drug of choice), MSSA bacteremia, soft tissue infections
- Cephalexin: oral UTIs, cellulitis, minor skin/soft tissue infections
Dosing (Katzung):
- Cephalexin: 0.25-0.5 g PO q.i.d.; peak serum 15-20 mcg/mL
- Cefazolin: 0.5-2 g IV q8h; peak serum ~185 mcg/mL after 1 g IV
Second Generation
Drugs: Cefuroxime, Cefaclor, Cefprozil (oral); Cefoxitin, Cefotetan (parenteral cephamycins)
Spectrum:
- Retains gram-positive coverage of 1st gen
- Extended gram-negative: adds H. influenzae, Moraxella, Klebsiella (including 1st-gen resistant strains), Neisseria
- Cephamycins (cefoxitin, cefotetan): add Bacteroides fragilis and anaerobic coverage
- None active against enterococci or Pseudomonas
Key uses:
- Cefuroxime: respiratory tract infections, sinusitis, otitis media
- Cefoxitin/cefotetan: intra-abdominal, pelvic infections (anaerobic coverage); surgical prophylaxis for colorectal procedures
- Caution: Do NOT use for Enterobacter infections - chromosomal AmpC beta-lactamase readily selects resistant mutants
Dosing:
- Cefuroxime oral: 250-500 mg twice daily
- Cefuroxime IV: 75-125 mcg/mL after 1 g infusion
Third Generation
Drugs: Ceftriaxone, Cefotaxime (parenteral); Cefdinir, Cefixime, Cefpodoxime (oral); Ceftazidime (anti-pseudomonal)
Spectrum:
- Markedly expanded gram-negative coverage, including Enterobacterales
- CSF penetration: therapeutic levels achieved (used for meningitis)
- Ceftazidime and ceftizoxime: active against P. aeruginosa
- Reduced gram-positive coverage compared to 1st gen
- Not active against MRSA, L. monocytogenes, C. difficile, enterococci
Key uses (Katzung):
- Ceftriaxone: meningitis (N. meningitidis, S. pneumoniae, H. influenzae), gonorrhea, community-acquired pneumonia, Lyme disease (disseminated), empiric sepsis coverage; unique biliary excretion
- Cefotaxime: meningitis, sepsis, serious gram-negative infections; metabolized by liver (useful in renal impairment)
- Ceftazidime: Pseudomonas infections (pneumonia, bacteremia)
- Oral 3rd gen (cefdinir, cefpodoxime): otitis media, community respiratory infections
Half-life: Ceftriaxone has a long half-life (~8 hours), allowing once-daily dosing
Fourth Generation
Drug: Cefepime (IV/IM only)
Spectrum:
- Wide spectrum: gram-positives (streptococci, MSSA - NOT MRSA) + extensive gram-negatives including Enterobacter species and P. aeruginosa
- More stable to chromosomal AmpC beta-lactamases than 3rd gen (zwitterionic structure allows rapid outer membrane penetration)
- E. coli, K. pneumoniae, P. mirabilis, Enterobacter spp., P. aeruginosa
Key uses: Febrile neutropenia, nosocomial pneumonia, complicated UTIs, Pseudomonas infections, Enterobacter infections where 3rd gen may fail
Advanced Generation (5th Generation)
Drugs: Ceftaroline, Cefiderocol
Ceftaroline
- Only beta-lactam in the US with activity against MRSA
- Binds PBP2a (the modified PBP that confers MRSA resistance) and PBP of penicillin-resistant S. pneumoniae
- Gram-negative coverage similar to ceftriaxone
- Gaps: No Pseudomonas, ESBL-producers, Acinetobacter
- Indications: complicated skin/soft tissue infections (cSSTI), community-acquired pneumonia (CAP)
- Twice-daily dosing limits outpatient use
Cefiderocol (Siderophore Cephalosporin)
- Novel mechanism: acts as a siderophore - binds extracellular ferric iron (Fe³+), then enters gram-negative bacteria via the iron uptake (active transport) pathway in addition to passive diffusion through porins
- Achieves high intracellular concentrations
- Active against multidrug-resistant gram-negatives, including those with KPC, OXA-type, and metallo-beta-lactamases (MBL)
- Active against: MDR Enterobacterales, P. aeruginosa, Acinetobacter baumannii
- No gram-positive or anaerobic activity
- Indications: complicated UTIs (including pyelonephritis), hospital-acquired and ventilator-associated pneumonia
- Warning: Associated with increased mortality in some carbapenem-resistant infections in one trial - reserve for limited/no alternative situations
- Dose adjustment for augmented renal clearance (may need 4x daily dosing)
5. Pharmacokinetics
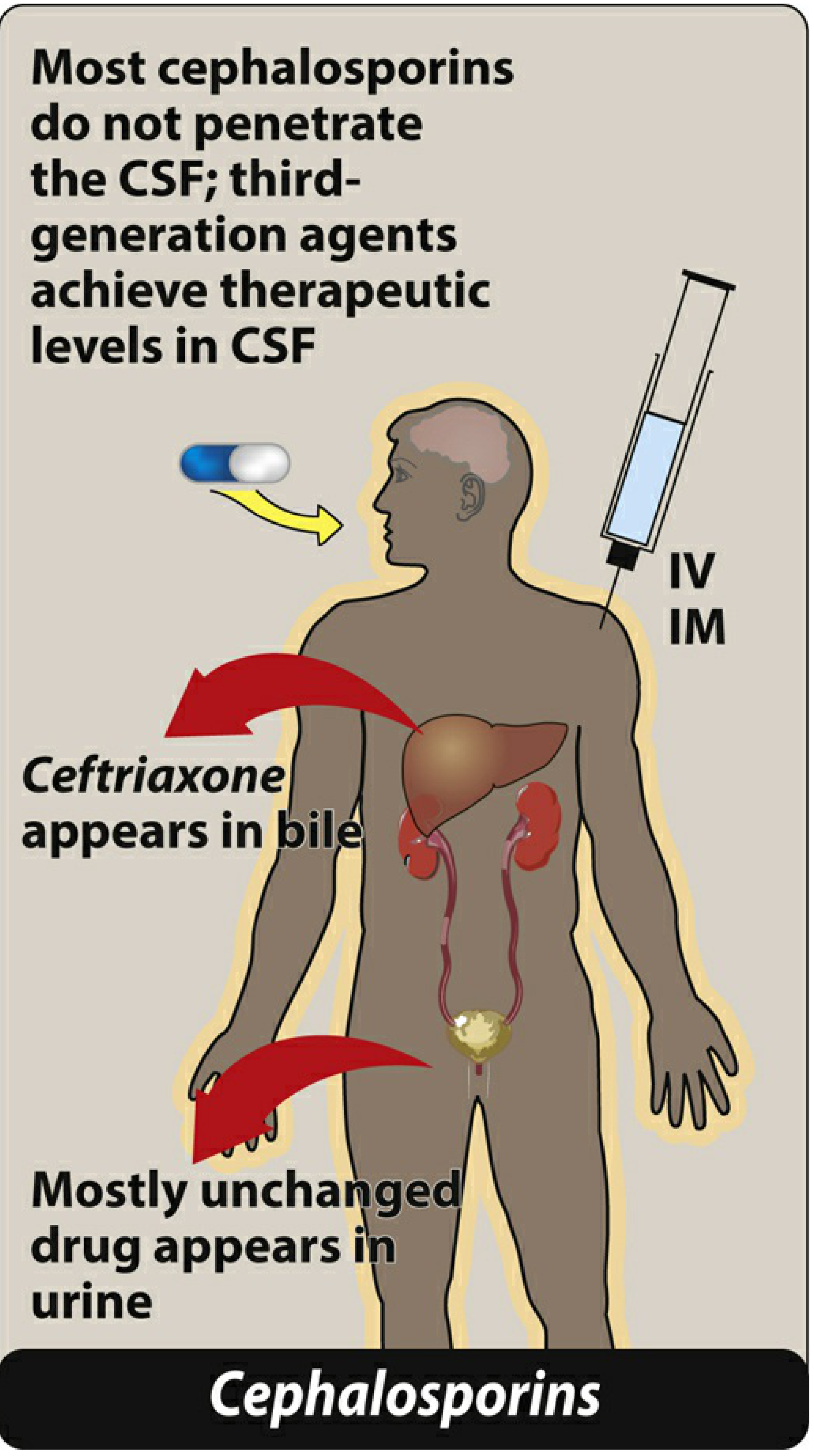
Figure: Administration and fate of the cephalosporins - most excreted unchanged in urine; ceftriaxone eliminated in bile (Lippincott Illustrated Reviews: Pharmacology)
| Parameter | Details |
|---|---|
| Route | Most require IV/IM (poor oral absorption). Oral agents: 1st gen (cephalexin), some 2nd gen (cefuroxime, cefaclor), oral 3rd gen (cefdinir, cefixime) |
| Distribution | Distribute widely into most tissues. Most do NOT penetrate CSF except 3rd gen and cefepime |
| Elimination | Primarily renal (glomerular filtration + tubular secretion). Probenecid blocks tubular secretion, raising serum levels |
| Exceptions | Ceftriaxone: biliary elimination (~40%); Cefotaxime: hepatic metabolism to active desacetylcefotaxime |
| Half-lives | Variable: cephalexin ~1h; cefazolin ~1.8h; ceftriaxone ~8h (once daily dosing possible) |
| Renal adjustment | Required for most agents when CrCl is impaired (except ceftriaxone). See table below |
Dosage adjustment for renal impairment (Katzung):
| Drug | Normal dose | CrCl ~50 mL/min | CrCl ~10 mL/min |
|---|---|---|---|
| Cephalexin PO | 0.25-0.5 g q6h | 50% | 25% |
| Cefazolin IV | 0.5-2 g q8h | 50% | 25% |
| Ceftriaxone IV | 1-2 g q12-24h | 100% | 100% |
6. Adverse Effects
Allergy & Cross-reactivity
- Hypersensitivity reactions (anaphylaxis, urticaria, fever, rashes, nephritis, granulocytopenia, hemolytic anemia) - similar to penicillins
- Cross-allergenicity with penicillins is low (1-2%) overall - the beta-lactam nucleus differs enough
- Cross-reactivity is most common when cephalosporins share identical R-side chains with penicillins (particularly 1st/2nd gen with aminopenicillins)
- Patients with penicillin anaphylaxis should NOT receive 1st or 2nd gen cephalosporins; use 3rd/4th gen with caution in a monitored setting (Katzung)
Toxicity
| Toxicity | Details |
|---|---|
| Local irritation | Pain at IM site; thrombophlebitis with IV infusion |
| Renal toxicity | Interstitial nephritis, tubular necrosis (uncommon) |
| Hypoprothrombinemia/Bleeding | Agents with methylthiotetrazole (MTT) group - cefotetan is the relevant current US agent. Prevented by vitamin K 10 mg PO twice weekly |
| Disulfiram-like reaction | MTT-containing agents (cefotetan) cause severe reaction with alcohol - alcohol must be avoided |
| Diarrhea / C. difficile | Disruption of gut flora; broad-spectrum agents are higher risk |
7. Important Coverage Gaps (All Generations)
Cephalosporins as a class are NOT active against:
- MRSA (except ceftaroline, cefiderocol has no gram-positive activity either)
- Enterococci (inherent resistance)
- Listeria monocytogenes
- Clostridioides difficile
- Atypicals (Mycoplasma, Chlamydia, Legionella - no cell wall)
8. Key Clinical Pearls
| Clinical Scenario | Drug of Choice |
|---|---|
| Surgical prophylaxis | Cefazolin (1st gen) |
| MSSA bacteremia | Cefazolin (superior to antistaphylococcal PCN in tolerability) |
| Bacterial meningitis (community) | Ceftriaxone + vancomycin (empiric) |
| Gonorrhea (uncomplicated) | Ceftriaxone IM |
| Lyme disease (disseminated/CNS) | Ceftriaxone IV |
| Pseudomonas infection | Ceftazidime, cefepime, or cefiderocol (MDR) |
| MRSA infection | Ceftaroline (only beta-lactam option) |
| Febrile neutropenia | Cefepime |
| Intra-abdominal (anaerobes) | Cefoxitin or cefotetan (2nd gen cephamycins) |
| MDR gram-negative (last resort) | Cefiderocol |
- Katzung's Basic and Clinical Pharmacology, 16th Ed., pp. 1247-1253
- Lippincott Illustrated Reviews: Pharmacology, pp. 955-962
This is a shared conversation. Sign in to Orris to start your own chat.