Colle's fracture
Reading File
Searching the Web
Colles fracture management 2024 2025
Finding Sources
Searching PubMed
"Colles fracture" OR "distal radius fracture" treatment outcomes
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is the full response:
Colles' Fracture
Definition
A Colles' fracture is a transverse fracture of the distal radial metaphysis, located within 2 cm of the radial articular surface, with dorsal displacement and angulation of the distal fragment. It is the most common wrist fracture.
Mechanism
- Fall on an outstretched hand (FOOSH) with the wrist in dorsiflexion and forearm in pronation
- Tension on the volar aspect causes the fracture line to extend dorsally
- Compression on the dorsal side produces dorsal comminution
- Low-energy mechanisms (e.g., simple falls) cause mainly extra-articular, minimally displaced fractures in elderly patients; high-energy mechanisms in younger patients produce comminuted or intra-articular fractures
Epidemiology / Risk Factors
- Most common in older women with osteoporosis (post-menopausal)
- Risk factors: decreased bone mineral density, female sex, white ethnicity, early menopause, prolonged steroid use
Fracture Characteristics
The classic Colles' fracture shows:
- Dorsal angulation of the distal radial articular surface
- Proximal and dorsal displacement of the distal fragment
- Radial displacement of the carpus
- Radial shortening (negative ulnar variance)
- Associated ulnar styloid fracture in ~60% of cases
- May extend intra-articularly into the radiocarpal or radioulnar joint ("die-punch" fracture)
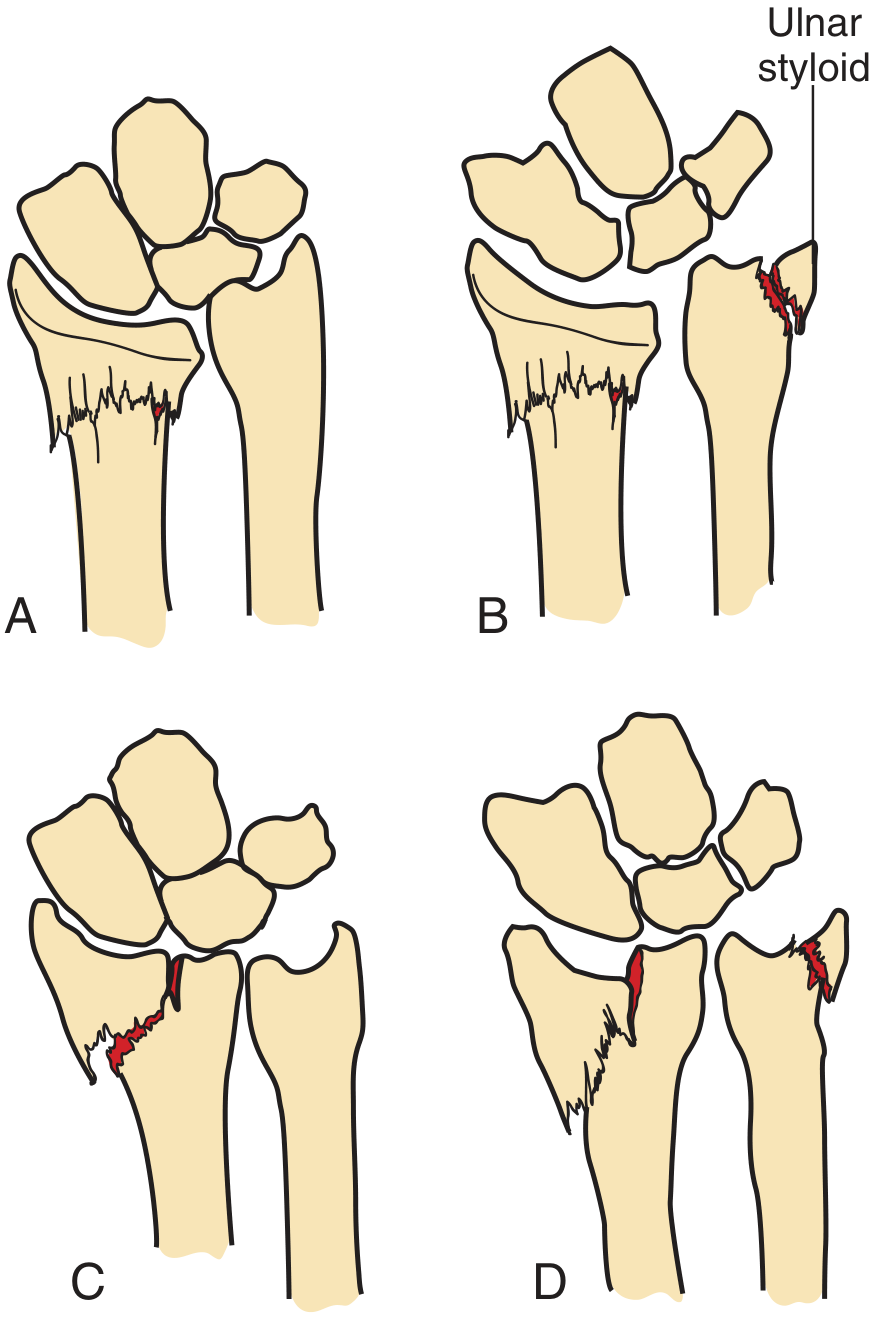
Fracture diagram - Pfenninger & Fowler's Procedures for Primary Care:
Clinical Presentation
- "Dinner fork" deformity - the classic appearance on physical exam and lateral X-ray
- Pain, swelling, and tenderness over the distal forearm
- Palmar paresthesias - from pressure or traction on the median nerve
- Neurologic exam is mandatory before and after any reduction attempt
Radiology
PA (posteroanterior) view:
- Distal metaphyseal fracture with radial shortening
- Intra-articular extension into radiocarpal or radioulnar joint if present
- Ulnar styloid fracture
Lateral view:
- Best shows the dorsal angulation and comminution
- Loss of normal volar tilt of the distal radial articular surface
X-ray: PA and lateral views showing Colles' fracture with radial shortening, intra-articular extension, ulnar styloid fracture, and classic dinner fork deformity on lateral (Rosen's Emergency Medicine):
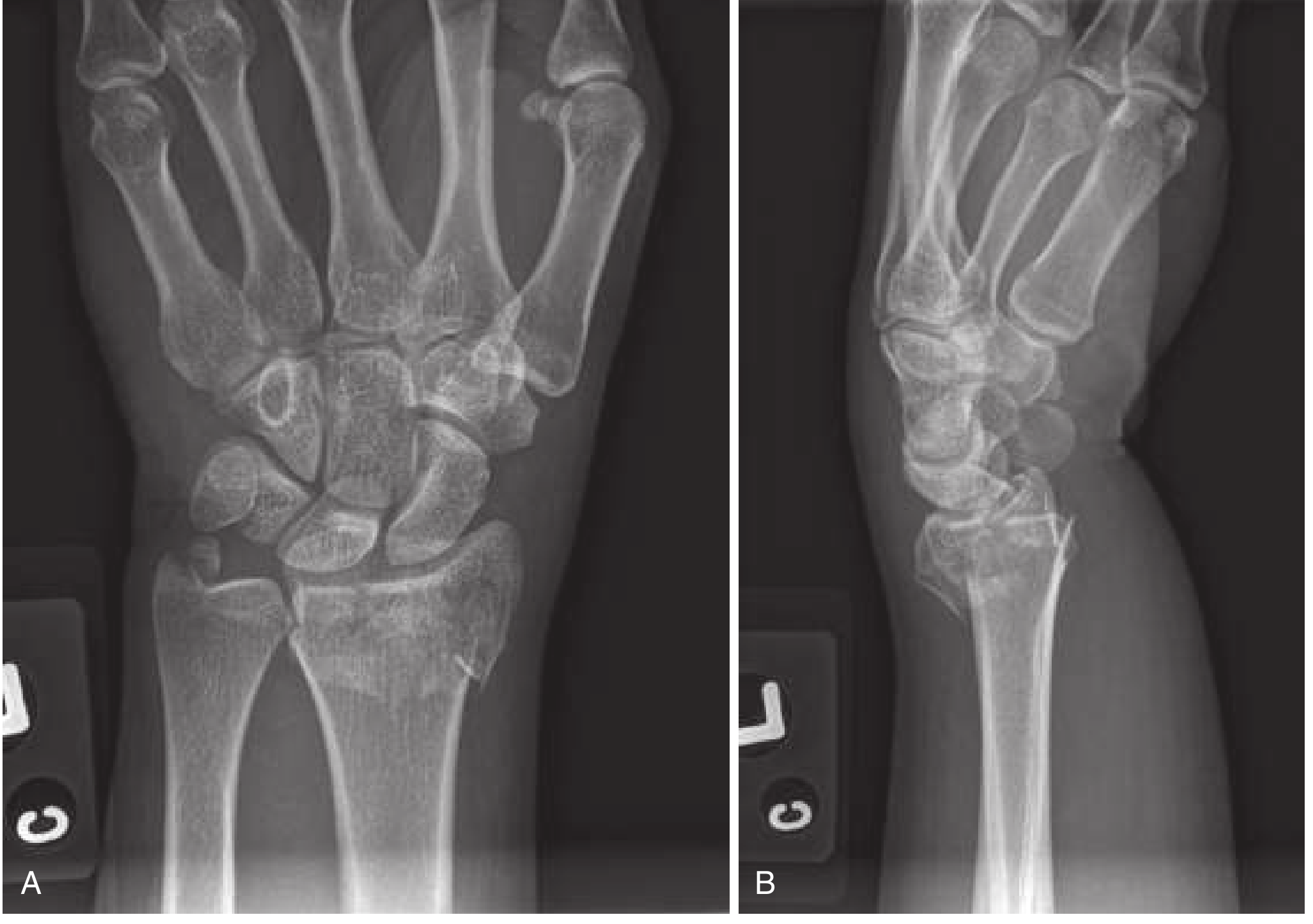
CT is indicated when significant intra-articular extension, comminution, or distal radioulnar joint instability is suspected.
Radiographic Criteria for Instability (Indicating Likely Surgical Need)
| Feature | Threshold |
|---|---|
| Dorsal angulation | >20 degrees |
| Radial shortening | >5 mm (radius shorter than ulna) |
| Intra-articular involvement | Any significant step-off |
| Marked comminution | Present |
Management
Stable, Non-displaced Fractures
- Double sugar-tong splint (one from elbow to wrist, second extending to axilla) for 3-5 days, then short-arm cast for 4-6 weeks
- Serial radiographs at 1, 2, and 6 weeks to confirm no displacement
- Urgent outpatient orthopedic referral within 7-10 days
Displaced Fractures - Closed Reduction
Goal: Restore volar tilt (minimum neutral/zero degrees), radial inclination, and proper radial length.
Anesthesia options:
- Hematoma block - most practical: 22-gauge needle on dorsum of distal radius, withdraw until hematoma encountered, instill 5-10 mL of 1% or 2% lidocaine ± bupivacaine
- Bier block (IV regional anesthesia)
- Median, radial, ulnar, or brachial plexus nerve blocks
- Procedural sedation
Reduction technique:
- Apply finger traps to provide longitudinal traction - relaxes deforming muscle forces; may alone achieve reduction
- Push distal fragment distally and palmarly while holding the forearm firmly
- If periosteal entrapment is suspected - re-create then reverse the injury mechanism under traction to unfold the periosteum
Post-reduction immobilization:
- Double sugar-tong splint or sugar-tong splint - do NOT apply circumferential cast immediately (edema risk)
- Allow finger movement; immobilize wrist
- Orthopedic follow-up within 2-3 days
Indications for Surgery
- Unstable, severely comminuted, or intra-articular fractures
- Fractures unreducible by closed means
- All open fractures
- Neurovascular compromise
- Dominant-wrist fractures in high-demand (very active) patients
- Loss of reduction after closed treatment
Surgical options include volar locking plate fixation (most common), external fixation, or dorsal bridge plating.
Complications
Occur in 6-80% of cases, more common with open fractures. Key complications:
| Complication | Notes |
|---|---|
| Carpal tunnel syndrome / median nerve injury | Most common; acute or delayed; 17% incidence |
| Malunion | Risk with inadequate reduction |
| Ulnar styloid fracture | 60% of radius fractures |
| TFCC injury | Triangular fibrocartilage complex; may cause DRUJ instability |
| Radiocarpal / radioulnar instability | Leads to arthritis |
| CRPS (complex regional pain syndrome) | Formerly "reflex sympathetic dystrophy" |
| Stiffness and weakness | Common long-term outcome, especially in elderly |
| Iatrogenic | Splinting in extreme flexion can damage median nerve |
Factors predicting long-term disability: dorsal angulation ≥20 degrees and ≥5 mm radial shortening.
Differential Diagnosis / Related Fractures
- Smith's fracture ("reverse Colles'") - volar angulation/displacement, from fall on a flexed wrist
- Barton's fracture - intra-articular fracture-dislocation of the radiocarpal joint (dorsal or volar variant)
- Chauffeur's / Hutchinson's fracture - radial styloid fracture
- Galeazzi fracture - distal radius fracture with DRUJ disruption
Sources:
- Tintinalli's Emergency Medicine, 9th ed., p. 1847
- Rosen's Emergency Medicine, p. 612
- Pfenninger & Fowler's Procedures for Primary Care, 3rd ed., p. 1321
Recent evidence: A 2024 meta-analysis (PMID 38987723) found that for distal radius fractures overall, surgical vs. non-surgical outcomes are similar in low-demand elderly patients but surgical fixation offers functional advantages in higher-demand patients - broadly consistent with current guidelines. A 2024 systematic review (PMID 39459458) on periarticular distal radius fractures in the elderly supports individualized surgical decision-making based on functional demand and bone quality.
This is a shared conversation. Sign in to Orris to start your own chat.