All about abortion in very simple with images
Reading File
Finding Sources
Finding Sources
Searching the Web
abortion types medical definition causes management simple explanation 2024
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Generating Image
A simple educational medical diagram showing the different types of abortion: threatened, inevitable, incomplete, complete, missed, and septic abortion - with simple uterus icons showing cervix open/closed and tissue present/absent for each type, in a clean infographic style
Loading Image
Loading Image
Reading File
Excellent! I now have all the information needed. Let me compile a comprehensive, simple, well-illustrated answer.
Abortion - A Simple Medical Guide
What is Abortion?
Abortion (from Latin aboriri, meaning "to miscarry") is the premature ending of a pregnancy before the fetus is able to survive outside the uterus - generally before 20 weeks of gestation. Any tissue expelled is called the abortus.
Globally, 25% of all pregnancies end in abortion. About 56 million abortions occur each year worldwide.
Two Big Categories
| Category | What it means |
|---|---|
| Spontaneous Abortion (Miscarriage) | Happens naturally, without any medical intervention |
| Induced Abortion | Deliberately ended by medicine or surgery |
Types of Abortion (Spontaneous)
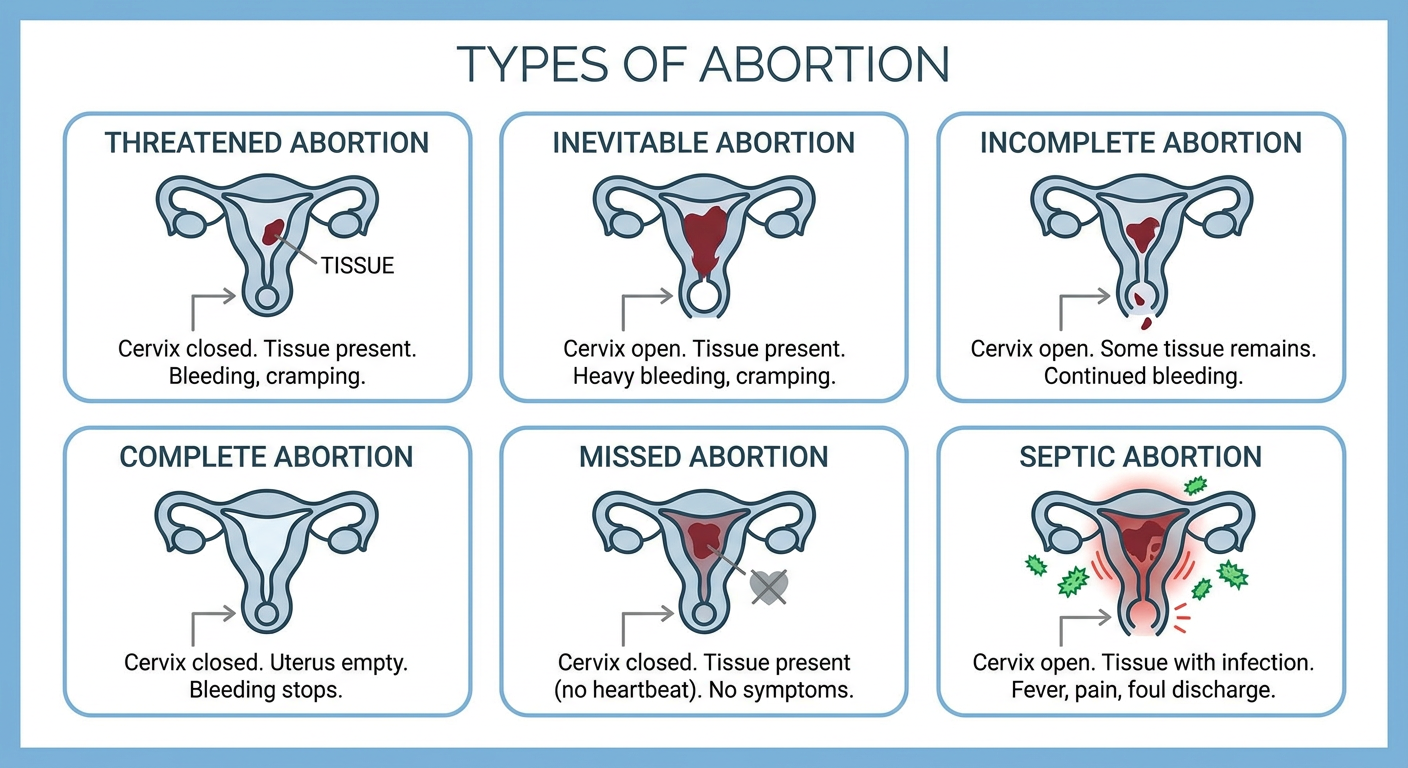
Here is what each type means:
1. Threatened Abortion
- Vaginal bleeding with or without cramping
- Cervix is CLOSED - pregnancy may still continue
- Occurs in ~25% of recognized pregnancies
- About half of these will eventually miscarry
2. Inevitable Abortion
- Cervix has opened (dilated)
- Heavy bleeding and cramping
- Pregnancy cannot be saved at this point
3. Incomplete Abortion
- Cervix is open
- Some tissue has passed, but some remains in the uterus
- Most common between 6-14 weeks
- Requires uterine evacuation (medical or surgical)
4. Complete Abortion
- All tissue has passed out of the uterus
- Cervix closes again, bleeding stops
- Confirmed by ultrasound showing an empty uterus
5. Missed Abortion
- The embryo/fetus has died but stays inside the uterus
- No cramping or bleeding - often no symptoms at all
- Discovered on ultrasound (no heartbeat)
6. Septic Abortion
- Any stage of abortion complicated by infection
- Signs: fever, uterine tenderness, foul-smelling discharge
- A medical emergency requiring antibiotics and uterine evacuation
7. Habitual (Recurrent) Abortion
- 3 or more consecutive spontaneous abortions
- Requires investigation for underlying causes
Causes of Spontaneous Abortion
Most spontaneous abortions (80%) happen in the first trimester. Common causes include:
| Cause | Examples |
|---|---|
| Chromosomal abnormalities | Aneuploidy, polyploidy - present in ~50% of cases |
| Maternal hormones | Poorly controlled diabetes, thyroid disorders, luteal phase defect |
| Uterine problems | Fibroids, polyps, uterine malformations |
| Infections | Toxoplasma, Mycoplasma, Listeria, certain viruses |
| Immune factors | Antiphospholipid antibody syndrome |
| Advanced maternal age | Risk rises sharply after age 35 |
| Exposure to toxins | Heavy metals, tobacco, some anesthetic agents |
"Fetal chromosomal anomalies are present in approximately 50% of early abortions." - Robbins Pathologic Basis of Disease
How is Abortion Diagnosed?
Doctors use several tools:
- Pelvic exam - Is the cervix open or closed? Is tissue visible?
- Quantitative β-hCG blood test - Measures pregnancy hormone levels
- Transvaginal Ultrasound - Checks for fetal heartbeat, gestational sac, retained tissue
- CBC - Checks for blood loss
Treatment Options
For Spontaneous Abortion:
Expectant Management - Wait and allow the body to expel tissue naturally, with monitoring via serial β-hCG and ultrasound.
Medical Management:
- Misoprostol (a prostaglandin) given vaginally - causes uterine contractions to expel tissue
- Works better in incomplete or inevitable abortion than missed abortion
Surgical Management:
- Manual Vacuum Aspiration (MVA) - A hand-held syringe empties the uterus
- Dilation & Curettage (D&C) - Surgical widening of the cervix + removal of uterine contents
- Preferred when medical management fails, or if heavy bleeding occurs
Induced Abortion Methods
Medical Abortion (the "Abortion Pill")
Used up to ~10 weeks of pregnancy.
- Mifepristone (200 mg orally) - Blocks progesterone, causing the uterine lining to break down
- Misoprostol (800 mcg, given 24-48 hours later) - Causes uterine contractions to expel the pregnancy
- Success rate: 96-99%
- Resembles a miscarriage
- Heavy cramping and bleeding expected for several hours
Surgical Abortion
Vacuum Aspiration (D&C)
- Used up to ~13 weeks
- A cannula (thin tube) is inserted into the uterus and suction removes the pregnancy
- Takes under 30 minutes, local or general anesthesia
- Success rate: >98%
- Major complication rate is very low (~0.16%)
Dilation & Evacuation (D&E)
- Used in the second trimester (after 14 weeks)
- More complex, requires greater cervical dilation
- Still safer than continuing pregnancy at advanced gestational age
Safety: Legal vs. Unsafe Abortion
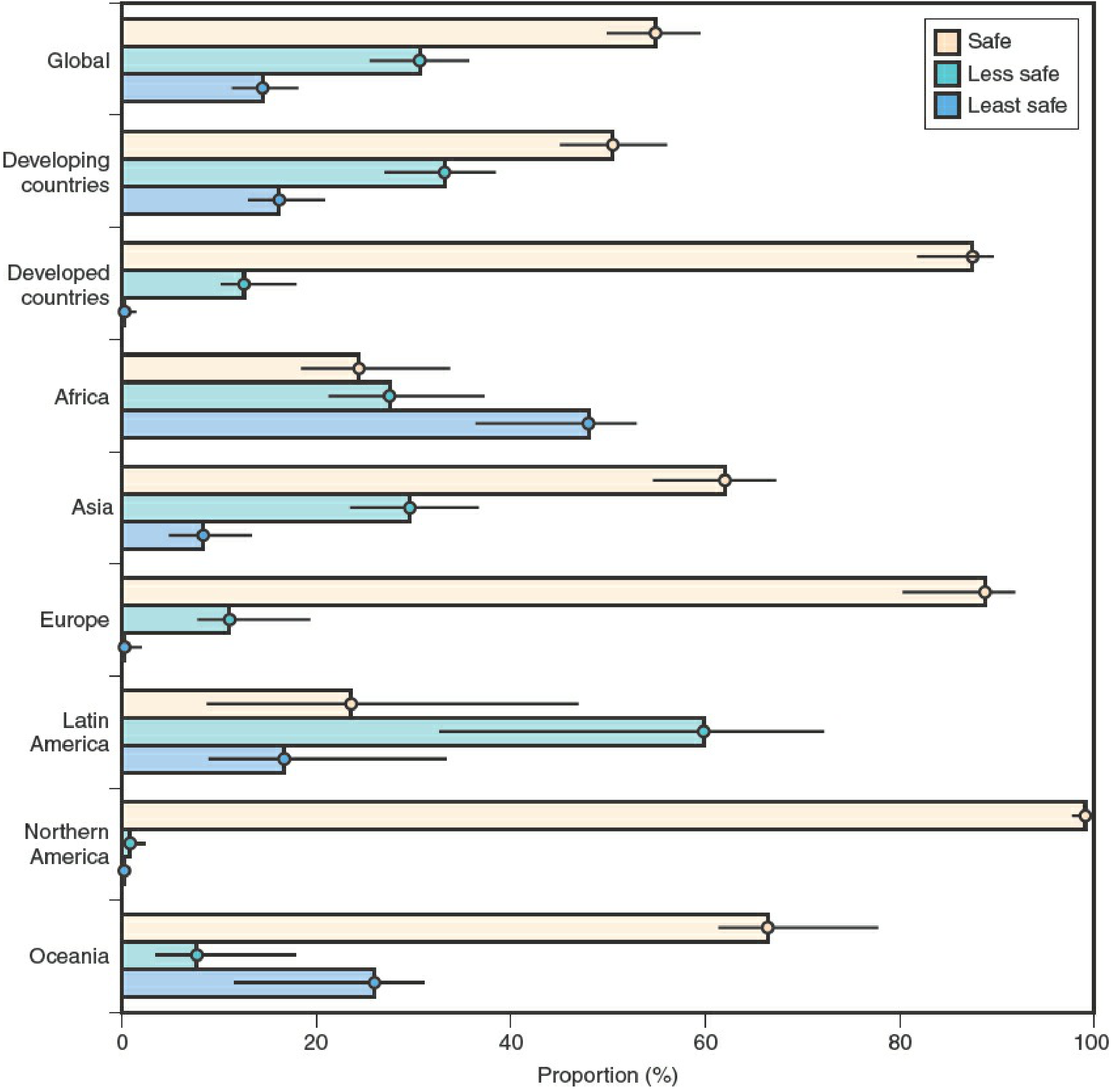
Figure: Proportion of safe, less-safe, and unsafe abortions by world region (Berek & Novak's Gynecology)
Key facts:
- Legal abortion mortality rate: 0.7 per 100,000 procedures (extremely safe)
- Unsafe abortion: ~25 million per year globally; kills 47,000 women annually
- Africa has the highest proportion of unsafe abortions
- Northern America and Northern Europe have nearly 100% safe abortions
- Where abortion is legal and accessible, it is safe. Where it is illegal or restricted, complications and deaths are common.
Key Investigations at a Glance
| Test | Why it's done |
|---|---|
| β-hCG (blood) | Confirms pregnancy; tracks hormone fall |
| Ultrasound | Confirms viability, rules out ectopic pregnancy |
| Blood type + Rh | Rh-negative women need Rh immunoglobulin (RhoGAM) to prevent future pregnancy problems |
| CBC | Checks for anemia from blood loss |
Quick Summary
| Type | Cervix | Tissue | Heartbeat | Action |
|---|---|---|---|---|
| Threatened | Closed | Inside | Present | Monitor, rest |
| Inevitable | Open | Inside | Present | Evacuation |
| Incomplete | Open | Partial | Absent | Evacuation |
| Complete | Closed | None | Absent | Monitor only |
| Missed | Closed | Inside | Absent | Medical/surgical |
| Septic | Open | Inside + infected | Absent | Urgent antibiotics + evacuation |
Sources: The Developing Human (Moore et al.), Berek & Novak's Gynecology, Tintinalli's Emergency Medicine, Robbins Pathologic Basis of Disease, Pfenninger & Fowler's Procedures for Primary Care, Swanson's Family Medicine Review.
This is a shared conversation. Sign in to Orris to start your own chat.