Otitis externa
Reading File
Finding Sources
Searching Images
otitis externa ear canal
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer:
Otitis Externa
Definition & Overview
Otitis externa (OE) is inflammation of the external auditory canal (EAC), affecting up to 10% of people during their lifetimes. It is more common in warm climates and summer months, and accounts for approximately 2.4 million healthcare visits per year in the US. Peak incidence is in 5–10 year-olds, though over half of cases occur in adults >20 years. — Cummings Otolaryngology
Classification
1. Acute Localized OE (Furunculosis)
- One or more pustules/furuncles in the EAC
- Causative organism: S. aureus
- Symptoms: itching, pain, swelling, redness, occasionally decreased hearing
2. Acute Diffuse OE ("Swimmer's Ear" / "Tropical Ear")
- Rapid onset (<48 hours) of canal inflammation
- Most common causative organism: P. aeruginosa (>90% of AOE is bacterial; P. aeruginosa and S. epidermidis are the dominant pathogens)
- Associated with water exposure or local trauma
3. Erysipelas of the Ear
- Caused by group A Streptococcus (S. pyogenes)
- Diffusely red, painful ear; hemorrhagic bullae may appear on canal walls
4. Chronic Otitis Externa (COE)
- Prolonged EAC inflammation; bilateral in >50% of patients; affects 3–5% of the population
- Mild discomfort, pruritus, aural fullness; skin shows atrophy ± stenosis
- Causes include: allergic/contact reactions (commonly neomycin), systemic diseases (psoriasis, seborrhoea, sarcoidosis, Sjögren), and chronic infection
5. Eczematous (Dermatitic) OE
- Severe pruritus, scaling, crusting, oozing, erythema
- Underlying skin conditions: contact dermatitis, seborrhoeic or atopic dermatitis
6. Malignant (Necrotizing) OE
- Aggressive, life-threatening form
- Predominantly in diabetics and immunocompromised patients
- Organism: P. aeruginosa
- Progression: apparent OE → canal maceration, granulation tissue → temporal bone osteomyelitis → intracranial extension → cranial nerve palsies (VII, IX, X, XII) or meningitis
- Bacteria are thought to access the temporal bone via the fissures of Santorini between ear cartilages
7. Fungal OE (Otomycosis)
- ~10% of AOE cases
- Severe pruritus, clear drainage, "cotton-like" debris filling the canal
- Candida: typical white discharge
- Aspergillus flavus: "wet newspaper" appearance — moist white plug with black dots
8. Viral OE (Rare)
- Organisms: varicella, measles, herpesvirus
- Herpes Zoster Oticus (HZO): canal involvement without facial palsy
- Ramsay Hunt syndrome: HZO + facial paralysis ± sensorineural hearing loss or vertigo
Predisposing Factors
| Category | Examples |
|---|---|
| Anatomical | Congenitally narrow canal, exostoses |
| Skin conditions | Eczema, seborrhoea, psoriasis |
| Trauma | Ear plugs, hearing aids, cotton bud use, wax removal attempts |
| Environmental | Swimming, humid climates, elevated canal pH |
| Systemic | Diabetes, HIV, immunosuppression, prior radiotherapy |
Clinical Features
Acute OE:
- Moderate-to-severe otalgia worsened by pinna manipulation (key distinguishing feature vs. mastoiditis, where tenderness is over the mastoid tip)
- Pruritus → progresses to seropurulent discharge, oedema, aural fullness, conductive hearing loss
- Signs: circumferential EAC erythema and oedema, otorrhoea, preauricular/cervical lymphadenopathy
- Weber test lateralises to the affected side (conductive loss from canal obstruction)
Chronic OE:
- Predominantly pruritus with mild discomfort
- Secretory (wet) or dry/squamous type
- Periodic waxing and waning course; may progress to medial canal fibrosis
Investigations
- Clinical diagnosis in most cases; examination under binocular microscopy preferred
- Canal culture (bacteria + fungi) for persistent or recurrent infection
- Biopsy if treatment-resistant — to exclude malignancy
- Imaging (CT/MRI): reserved for suspected spread beyond EAC
- CT: demonstrates bony erosion in necrotizing OE
- MRI with gadolinium: preferred for soft tissue and intracranial extension in malignant OE
Treatment
Acute OE (Uncomplicated)
- Canal debridement/cleaning — removes obstructive debris, allows drop penetration
- Topical antibiotic drops — effective for most cases; systemic antibiotics are not indicated in immunocompetent patients with infection confined to the canal
- Fluoroquinolone drops (e.g., ciprofloxacin/ofloxacin): first choice; safe with tympanic membrane perforation
- Aminoglycoside drops (e.g., neomycin, gentamicin): effective but contraindicated with TM perforation (ototoxic)
- Topical corticosteroids often combined to reduce inflammation
- Acidifying drops (acetic acid) useful for mild cases and prophylaxis
Fungal OE
- Topical antifungal agents after thorough canal cleaning
Chronic OE
- Address underlying cause (allergic: remove offending agent; systemic disease: treat primary condition)
- Periodic aggressive debridement
Malignant (Necrotizing) OE
- Systemic antipseudomonal antibiotics — ciprofloxacin is standard initial therapy
- Aggressive debridement by an otolaryngologist
- MRI with gadolinium for extent assessment
- Surgical intervention for refractory cases
- Coordination with ENT is mandatory
Clinical Images



Sources: Cummings Otolaryngology Head and Neck Surgery | Textbook of Family Medicine 9e, p. 267 | Rosen's Emergency Medicine
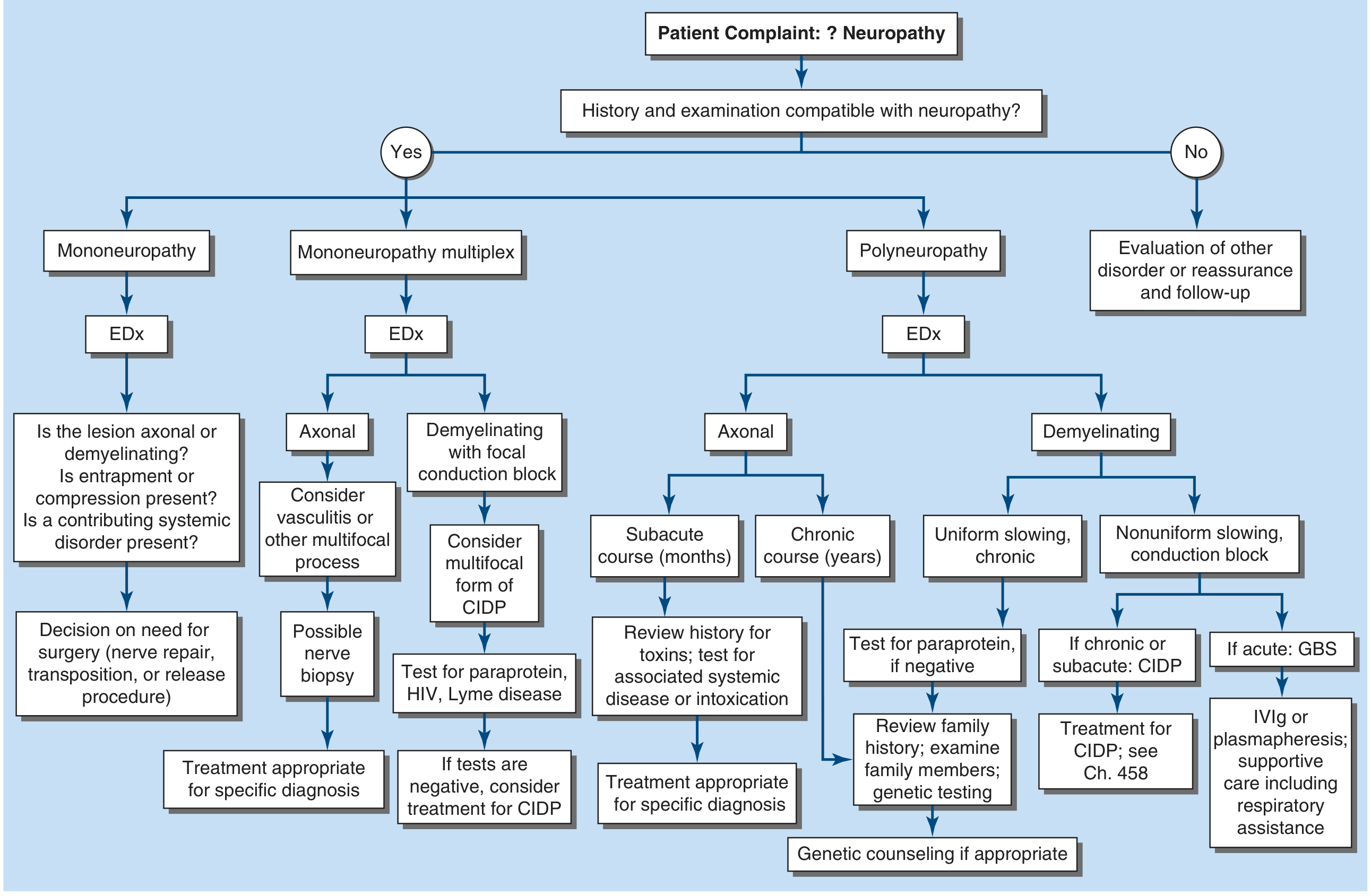
Neuropathy
Reading File
Finding Sources
Finding Sources
Searching Images
peripheral neuropathy nerve pathology diagram
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive content and a diagnostic flowchart. Let me compile the full, structured answer.
Peripheral Neuropathy
Overview
Peripheral nerves contain sensory, motor, and autonomic fibers. Diseases can affect the cell body (neuronopathy/ganglionopathy), the myelin sheath (myelinopathy), or the axon (axonopathy) — each with distinct clinical and electrophysiologic signatures.
Nerve fibers are classified into:
- Large myelinated — conduct at ~50 m/s; motor axons; also carry vibration/proprioception
- Small myelinated — transmit pain and temperature
- Small unmyelinated — autonomic fibers; also pain/temperature
Despite extensive evaluation, ~50% of peripheral neuropathies remain idiopathic (cryptogenic sensory and sensorimotor polyneuropathy, CSPN), typically presenting as predominately sensory polyneuropathy. — Harrison's Principles of Internal Medicine 22E
Classification
By Distribution
| Pattern | Features | Key Diagnoses |
|---|---|---|
| Mononeuropathy | Single nerve, focal | Entrapment (carpal tunnel, ulnar), trauma, vasculitis |
| Mononeuropathy multiplex | Multiple non-contiguous nerves, asymmetric, stepwise | Vasculitis, diabetes, leprosy, sarcoid, Lyme, HIV, cryoglobulinemia |
| Polyneuropathy | Bilateral, symmetric, length-dependent (distal > proximal) | Diabetes, alcohol, uremia, drugs/toxins, hereditary, GBS, CIDP |
| Polyradiculopathy/Plexopathy | Asymmetric proximal + distal | Diabetic amyotrophy, meningeal carcinomatosis, amyloid |
By Pathology
| Type | Mechanism | NCS Finding |
|---|---|---|
| Axonopathy | Axonal degeneration (dying-back) | Reduced amplitude, normal or mildly reduced conduction velocity |
| Myelinopathy | Demyelination | Markedly slowed conduction velocity, prolonged latencies, conduction block |
| Neuronopathy | Cell body loss (DRG or motor neuron) | Absent sensory responses, normal motor conduction |
The Seven Key Diagnostic Questions (Harrison's)
- What systems are involved? Motor / sensory / autonomic / combined
- Distribution of weakness? Distal only vs. proximal+distal; focal/asymmetric vs. symmetric
- Nature of sensory involvement? Small-fiber (pain/temp loss, burning) vs. large-fiber (vibration/proprioception loss)
- UMN involvement? Suggests central + peripheral pathology (e.g., B₁₂ deficiency, adrenoleukodystrophy)
- Temporal evolution? Acute (≤4 weeks) / subacute (4–8 weeks) / chronic (>8 weeks)
- Hereditary neuropathy? Family history; sensory signs without symptoms (asymptomatic at first)
- Associated medical conditions? Cancer, diabetes, connective tissue disease, infection (HIV, Lyme, leprosy), alcohol, drugs, toxins
Diagnostic Approach
Major Causes
1. Diabetic Neuropathy (most common cause in clinical practice)
~15% of diabetics have symptomatic polyneuropathy; ~50% have electrophysiological evidence. Duration of diabetes is the single most important factor — <10% at diagnosis, rising to 50% after 25 years. — Adams & Victor's Neurology 12E
Six clinical syndromes:
| Syndrome | Features |
|---|---|
| Distal symmetric sensory polyneuropathy | Most common; chronic, slowly progressive; stocking-glove paresthesias, pain, numbness; feet and legs |
| Acute painful mononeuropathy | Acute onset, single nerve (limb or trunk); thoracolumbar radiculopathy pattern |
| Diabetic amyotrophy (proximal motor neuropathy) | Acute/subacute painful asymmetric proximal weakness; upper lumbar roots; "Bruns-Garland syndrome" |
| Cranial mononeuropathy | Acute ophthalmoplegia (CN III most common, or CN VI); pupil-sparing CN III palsy typical |
| Proximal symmetric motor neuropathy | Subacute/chronic; symmetrical proximal wasting; variable sensory loss |
| Autonomic neuropathy | Orthostatic hypotension, gastroparesis, neurogenic bladder, anhidrosis, erectile dysfunction |
Pathomechanism: Microangiopathy → ischemia/infarction of endoneurial blood vessels (vasa nervorum); also direct metabolic axonal damage and inflammation. — Robbins & Kumar Basic Pathology
2. Uremic Neuropathy (CKD)
- Length-dependent axonal degeneration of lower limbs
- Mechanism: accumulated "middle molecules" (300–12,000 Da uremic toxins) inhibit Na⁺/K⁺-ATPase → altered nerve excitability; lower limb motor axons depolarized pre-dialysis, normalise post-dialysis
- Mononeuropathy multiplex in CKD → consider vasculitic neuropathy (ANCA+ vasculitis, polyarteritis nodosa)
- Very slow NCV (<½ normal) suggests coexisting demyelination — Comprehensive Clinical Nephrology 7E
3. Inflammatory / Immune-Mediated
| Condition | Key Features | Treatment |
|---|---|---|
| GBS (Acute AIDP) | Acute ascending paralysis, areflexia, albuminocytologic dissociation in CSF; peak 2–4 weeks | IVIg or plasmapheresis + respiratory support |
| CIDP | Symmetric proximal + distal weakness, sensory loss; >8 weeks; relapsing-remitting | IVIg, plasmapheresis, steroids |
| Multifocal motor neuropathy | Asymmetric distal weakness without sensory loss; anti-GM1 antibodies; conduction block on NCS | IVIg |
| Vasculitic neuropathy | Mononeuropathy multiplex; stepwise, painful | Immunosuppression (steroids ± cyclophosphamide) |
4. Hereditary Neuropathies
| Condition | Gene/Mechanism | Features |
|---|---|---|
| CMT1 (Charcot-Marie-Tooth type 1) | PMP22 duplication; demyelinating | Foot deformity (pes cavus), distal wasting, slow NCV |
| CMT2 | Various; axonal | Similar phenotype, normal NCV |
| Hereditary neuropathy with pressure palsies (HNPP) | PMP22 deletion | Recurrent compression palsies |
| Familial amyloid neuropathy | TTR mutations | Small-fiber + autonomic predominant |
5. Toxic / Drug-Induced
Common causative agents:
- Chemotherapy: vincristine, cisplatin, oxaliplatin, paclitaxel, bortezomib (CIPN — chemotherapy-induced peripheral neuropathy; mechanisms include microtubule disruption, mitochondrial damage, DNA injury → Wallerian degeneration or apoptosis)
- Antibiotics: isoniazid (pyridoxine deficiency), nitrofurantoin, metronidazole
- Others: amiodarone, colchicine, thalidomide, statins, heavy metals (lead, arsenic, thallium), alcohol
6. Infectious
- Leprosy — most common infectious cause of neuropathy worldwide; M. leprae directly invades Schwann cells
- HIV — distal sensory polyneuropathy; also antiretroviral toxic neuropathy
- Lyme disease (B. burgdorferi) — cranial neuropathy, radiculopathy, mononeuropathy multiplex
- Herpes zoster — postherpetic neuralgia; also rare motor neuropathy
7. Other Systemic Causes
- Vitamin B₁₂ deficiency — large-fiber + posterior column involvement (subacute combined degeneration)
- Amyloidosis — small-fiber + autonomic; autonomic dysfunction without diabetes → think amyloid
- Hypothyroidism, paraproteinaemia (MGUS, myeloma), sarcoidosis, paraneoplastic (anti-Hu, anti-CV2)
Small-Fiber Neuropathy
A distinct entity: pain and temperature loss, burning dysesthesias, autonomic symptoms — with normal NCS (only large fibers assessed by NCS).
- Diagnosis confirmed by skin punch biopsy (reduced intraepidermal nerve fiber density) or quantitative sensory testing
- Most common causes: diabetes / impaired glucose tolerance (GTT warranted even when fasting glucose is normal), amyloid, idiopathic
Investigations
| Test | Purpose |
|---|---|
| Nerve conduction studies (NCS) + EMG | Axonal vs. demyelinating; distribution; severity |
| Blood: FBS/HbA1c, B₁₂, TFTs, LFTs, CBC, ESR, CRP | Screen metabolic/systemic causes |
| Serum protein electrophoresis + immunofixation | Paraprotein |
| Anti-ganglioside antibodies (GM1, GQ1b) | MMN, Miller Fisher syndrome |
| ANCA, anti-dsDNA, ANA | Vasculitis, connective tissue disease |
| HIV, Lyme, HBV/HCV serology | Infectious |
| CSF | GBS: elevated protein, normal cells (albuminocytologic dissociation) |
| Nerve biopsy (sural nerve) | Vasculitis, amyloid, leprosy, atypical cases |
| Skin punch biopsy | Small-fiber neuropathy |
| Genetic testing | Hereditary neuropathies |
| MRI (neurography) | Plexopathy, nerve compression, CIDP |
Treatment Principles
Disease-Modifying
| Cause | Treatment |
|---|---|
| Diabetes | Glycaemic control (delays progression); no proven reversal of established neuropathy |
| GBS | IVIg (2 g/kg) or plasmapheresis; respiratory monitoring (spirometry) |
| CIDP | IVIg, plasmapheresis, corticosteroids, rituximab (refractory) |
| Vasculitis | High-dose corticosteroids + cyclophosphamide |
| Mononeuropathy (entrapment) | Splinting, corticosteroid injection, surgical decompression |
| B₁₂ deficiency | Replacement therapy |
| Amyloidosis (TTR) | Tafamidis, patisiran (siRNA), inotersen |
| Leprosy | WHO multidrug therapy (dapsone, rifampicin, clofazimine) |
Neuropathic Pain Management
| Drug Class | Examples | Notes |
|---|---|---|
| Anticonvulsants | Gabapentin, pregabalin | First-line for painful diabetic neuropathy and postherpetic neuralgia |
| SNRIs | Duloxetine, venlafaxine | Duloxetine FDA-approved for diabetic peripheral neuropathy |
| TCAs | Amitriptyline, nortriptyline | Effective; limited by anticholinergic side effects in elderly |
| Topical | Lidocaine patch, capsaicin 8% patch | Localised pain; well tolerated |
| Opioids | Tramadol, tapentadol | Second/third-line; abuse potential |
| Sodium channel blockers | Mexiletine | Refractory cases |
Sources: Harrison's Principles of Internal Medicine 22E | Adams & Victor's Principles of Neurology 12E | Robbins & Kumar Basic Pathology | Comprehensive Clinical Nephrology 7E
This is a shared conversation. Sign in to Orris to start your own chat.