what is plantar plate dysfunction in podiatry uk and what are the clinical tests and management and insole prescription and diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent — I now have comprehensive textbook material and images. Here is a thorough clinical answer:
Plantar Plate Dysfunction
Anatomy
The plantar plate is a dense fibrocartilaginous thickening of the plantar joint capsule at the metatarsophalangeal (MTP) joint. It sits on the plantar aspect of each lesser MTP joint and has the following key attachments:
- Distally — firmly attached to the plantar base of the proximal phalanx
- Proximally — loosely attached to the metatarsal head (this proximal insertion is the weak point prone to tearing)
- Laterally — connected via the deep transverse metatarsal (intermetatarsal) ligament to adjacent plantar plates
- Dorsally — the margins attach to the accessory collateral ligaments and the extensor sling (transverse lamina of the extensor aponeurosis)
- Plantarly — attached to the flexor tendon sheath, plantar aponeurosis longitudinal septa, and plantar fascia
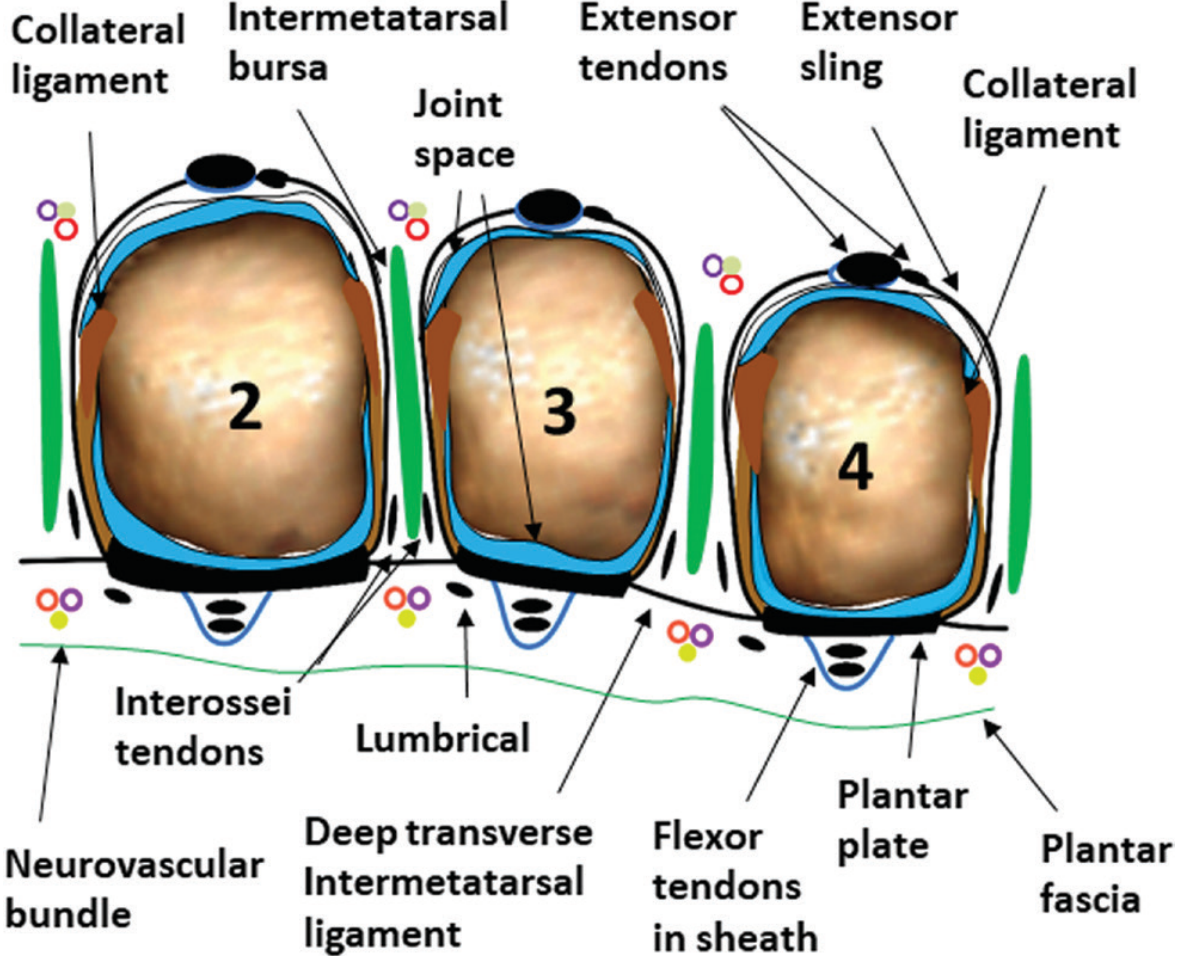
Schematic of lesser MTP joints (2nd, 3rd, 4th). The plantar plate sits plantar to the MTP joint, with flexor tendons in their sheaths running beneath it. — Imaging Anatomy: Bones, Joints, Vessels & Nerves
The plate acts as the primary restraint against dorsal subluxation of the proximal phalanx on the metatarsal head. It also resists hyperextension, provides a smooth gliding surface for the flexor tendons, and transmits metatarsal head load.
What Is Plantar Plate Dysfunction?
Plantar plate dysfunction (PPD) is a spectrum of injury — from attenuation and partial tearing through to complete rupture — of the plantar plate, usually at the lesser MTP joints (most commonly the 2nd). In the UK podiatric context it is also referred to as predislocation syndrome or MTP joint instability.
The injury typically occurs at the proximal insertion (where the plate attaches to the metatarsal neck), and is classified using the Thompson and Hamilton grading system (widely used in UK practice):
| Grade | Pathology |
|---|---|
| 0 | Synovitis / capsulitis — plate intact |
| 1 | Partial thickness tear, medial or lateral extension |
| 2 | Complete transverse tear, distal |
| 3 | Extensive tear with collateral ligament involvement |
| 4 | Button-hole tear with MTP dislocation |
Aetiology & Risk Factors
- Long 2nd metatarsal (index minus / Greek foot) — increased load under 2nd MTP
- Hallux valgus — transfers load laterally to 2nd MTP
- Equinus / tight gastrocnemius — increased forefoot loading
- High-heeled or narrow footwear — sustained dorsiflexion position
- Repetitive microtrauma — runners, court sports players
- Iatrogenic — steroid injection into the MTP joint can attenuate the plantar plate, leading to crossover toe deformity
- Inflammatory arthropathy (RA, gout)
Clinical Presentation
- Pain localised to the plantar aspect of the lesser MTP joint, often described as walking on a "stone"
- Swelling at the MTP joint ("sausage toe" / synovitis)
- Plantar callosity under the affected metatarsal head
- Toe deviation — the toe may drift dorsally or medially (crossover toe) as the plate fails
- Worse with barefoot walking, pushing off, and high-heeled shoes
- Morning stiffness less pronounced than in inflammatory arthritis
Clinical Tests
1. Lachman / Anterior Drawer Test of the MTP Joint (most sensitive)
This is the most sensitive physical examination test for plantar plate injury.
- Hold the metatarsal shaft stable with one hand
- Grasp the proximal phalanx of the affected toe between thumb and index finger
- Apply a dorsal thrust force (push the toe up/dorsally)
- Positive: pain elicited at the MTP joint, or excessive dorsal translation (>2 mm compared to the adjacent toes), or instability/subluxation
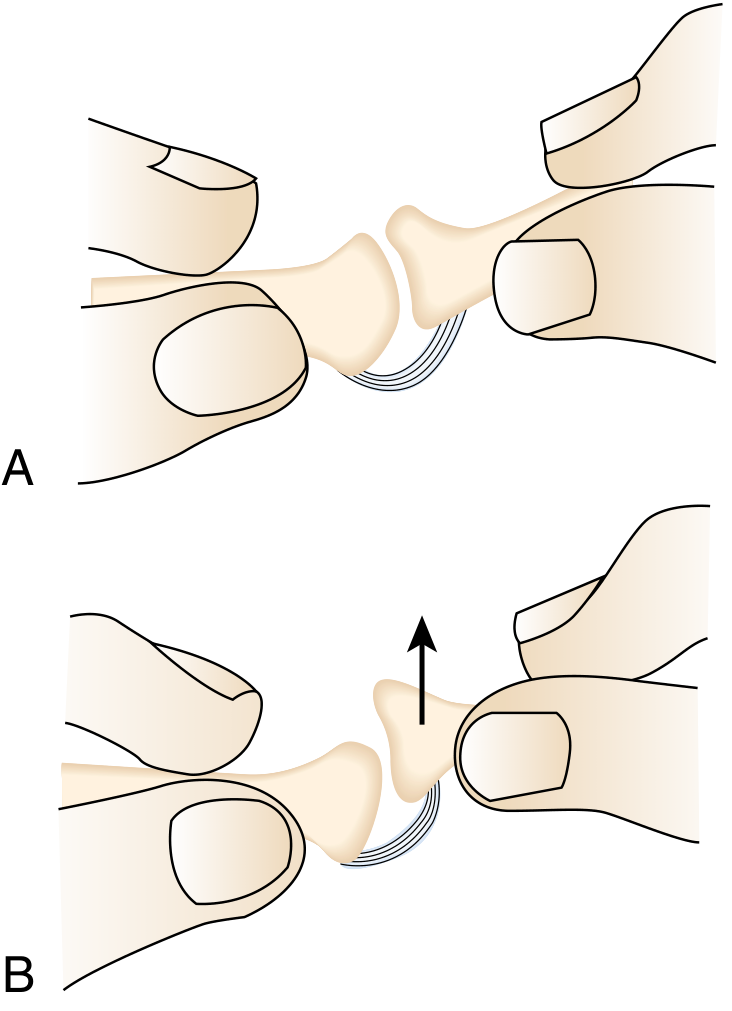
Dorsoplantar drawer test of the lesser MTP joint. Pain or subluxation with upward thrust (B) confirms MTP instability. — Miller's Review of Orthopaedics, 9th Ed.
2. Paper Pull-Out Test (Kelikian Push-Up Test / Toe Purchase Test)
- A sheet of paper is placed under the toes on a flat surface
- The patient pushes all toes down against the paper
- The examiner attempts to pull the paper out from under the affected toe
- Positive: paper slides out easily, indicating loss of flexor purchase due to plantar plate failure
3. Digital Compression / Squeeze Test
- Compress the MTP joint from dorsal to plantar
- Positive: localised plantar tenderness under the metatarsal head
4. Varus/Valgus Stress Testing
- With the MTP joint in neutral, apply medial and lateral stress
- Assesses collateral ligament integrity alongside the plantar plate
- In crossover toe deformity, lateral collateral attenuation is typically found
5. Sagittal Plane Stability Assessment
- Observe the toe in stance and single-leg heel raise
- Note any dorsal float (toe no longer plantarflexing during propulsion)
- Reduction in toe purchase in heel raise = plantar plate incompetence
Investigations & Imaging
| Modality | Finding |
|---|---|
| Plain X-ray (weight-bearing AP, lateral, oblique) | Metatarsal length pattern, metatarsal head shape; possible dorsal subluxation of proximal phalanx |
| MRI | Gold standard — shows plantar plate discontinuity, partial or full-thickness tears, capsular signal change; MR arthrogram improves sensitivity |
| Ultrasound | Dynamic — can demonstrate plantar plate tears and MTP instability in real-time; useful in UK podiatric practice as first-line imaging |
| MR arthrogram | Best for grading partial tears; contrast extravasation into plantar plate confirms tear |
Per Miller's: "If the diagnosis is in question, a Magnetic Resonance Arthrogram of the involved joint will identify any injuries to the plantar plate or collateral ligaments."
Management
Conservative (First-Line — UK Podiatry-Led)
| Intervention | Rationale |
|---|---|
| Toe taping / buddy strapping | Plantarflexes the proximal phalanx, offloads the plantar plate, reduces dorsal subluxation |
| Metatarsal pad / bar | Transfers load proximal to the metatarsal head, reducing shear forces on the plate |
| Lesser-toe orthotics / corrective splints | Reduces deforming forces; can minimise discomfort (note: will not permanently correct established deformity) |
| Footwear advice | Stiff-soled shoes (rocker sole), wider toe box, low heel — reduces MTP dorsiflexion loading |
| Activity modification | Reduce high-impact/propulsive loading in the acute phase |
| NSAIDs / analgesia | Manage pain and synovitis |
| Physiotherapy | Intrinsic muscle strengthening (lumbrical/interossei), calf stretching if equinus present |
Important UK Practice Point: Corticosteroid injection into the MTP joint is contraindicated in suspected plantar plate injury — it can cause iatrogenic plantar plate attenuation and lead to or worsen crossover toe deformity.
Orthotic / Insole Prescription for Plantar Plate Dysfunction
The aim is to: (1) offload the plantar plate, (2) restore sagittal plane stability, (3) reduce dorsiflexory forces at the MTP joint, and (4) correct any underlying biomechanical drivers.
Key Elements of the Prescription:
1. Metatarsal Dome / Metatarsal Pad
- Placed proximal to the metatarsal head(s) — typically at the proximal 1/3 of the metatarsal shaft
- Elevates the metatarsal shaft, decompresses the metatarsal head, and shifts load away from the symptomatic MTP joint
- Size and density adjusted to tolerance
2. Toe Prop / Digit Pad
- Silicone or felt toe prop under the proximal phalanx of the affected digit
- Maintains plantarflexion of the toe, restoring flexor purchase and preventing dorsal drift
- Essential in grade 2–3 dysfunction
3. Morton's Extension / Kinetic Wedge (Reverse)
- A cut-out or recess under the 2nd (or affected) metatarsal head can be added to a custom device to reduce direct pressure
- Kinetic wedge: 1st ray cut-out promotes 1st ray plantarflexion and may redistribute load if 2nd MTP is the primary problem
4. Hallux Valgus Correction / Medial Arch Support
- If hallux valgus is a contributing driver of 2nd MTP overload, medial arch support and toe spacer are incorporated
- Reduces lateral transfer of propulsive load onto the 2nd MTP joint
5. Heel Raise
- Modest heel raise (3–6 mm) reduces ankle equinus contribution to forefoot loading
6. Stiff / Semi-Rigid Shell (Custom Orthosis)
- Custom polypropylene or carbon fibre orthosis with forefoot extension for severe cases
- A stiff forefoot extension (rocker modification) limits MTP dorsiflexion during propulsion — the primary injury mechanism
- Use a full-length orthosis with digital accommodations rather than a 3/4 device in symptomatic cases
7. Footwear Modification
- Rocker-sole shoe or metatarsal bar added to the shoe externally limits MTP extension during toe-off
- Considered when insole modifications alone are insufficient
Operative (When Conservative Fails, Typically >3–6 Months)
| Procedure | Indication |
|---|---|
| Plantar plate repair | Complete (grade 3–4) tears; especially in active/athletic patients. Usually combined with a Weil shortening osteotomy of the distal metatarsal to decompress the joint and aid visualisation |
| Flexor-to-extensor tendon transfer | Severe instability or deformity; provides dynamic stabilisation of the MTP joint |
| EDB tendon transfer | Less severe deformity; rerouted plantar to intermetatarsal ligament; preserves more MTP mobility than flexor-to-extensor |
| Weil osteotomy | Required if severe subluxation or dislocation of the MTP joint |
| MTP synovectomy + capsular reconstruction | Isolated synovitis (grade 0–1) not responding to conservative care |
Summary for UK Podiatric Practice
- Diagnose clinically using the anterior drawer test (most sensitive), toe purchase test, and varus/valgus stress testing
- Image with ultrasound or MRI — MR arthrogram if grading is needed prior to surgical referral
- Grade the injury using the Thompson & Hamilton system to guide management intensity
- First-line: toe taping + metatarsal pad + footwear advice + intrinsic strengthening
- Insole prescription: metatarsal dome proximal to the head + toe prop + rocker/stiff forefoot extension ± hallux valgus correction
- Avoid corticosteroid injection into the MTP joint
- Refer for surgical opinion after 3–6 months failed conservative care, or earlier in grade 3–4 tears with progressive deformity
— Miller's Review of Orthopaedics, 9th Ed. | Imaging Anatomy: Bones, Joints, Vessels & Nerves
what does an Ankle pressure reading show if it is below 100, belo1 70 and below 50 in podiatry
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I have excellent textbook data. Now let me clarify something important for the user — the question asks about absolute ankle pressure in mmHg (not ABI ratio). The textbooks confirm these thresholds clearly. Let me now compile the full answer.
Ankle Pressure Thresholds in Podiatry
Important clarification: You are asking about absolute ankle systolic pressure in mmHg — measured with a handheld Doppler probe and sphygmomanometer cuff placed at the ankle. This is distinct from the Ankle-Brachial Pressure Index (ABPI), which is a ratio. Both are used in UK podiatry vascular assessment, and the absolute pressure values carry specific clinical significance.
How Ankle Pressure Is Measured
A Doppler probe detects the return of flow in either the dorsalis pedis or posterior tibial artery as the ankle cuff is deflated. The pressure at which flow returns = the ankle systolic pressure (in mmHg).
Clinical Significance of Ankle Pressure Thresholds
Ankle Pressure < 100 mmHg
- Indicates haemodynamically significant peripheral arterial disease (PAD)
- In a healthy limb, ankle systolic pressure should be equal to or slightly higher than brachial pressure (the leg is normally ~10–20 mmHg higher due to pulse pressure amplification)
- A value below 100 mmHg suggests arterial insufficiency is present and requires further vascular assessment
- Clinically: the patient may be asymptomatic or have mild-to-moderate claudication
- At this level, wound healing may already be compromised — sufficient for intact skin but not for tissue repair
- In UK podiatric practice, values below 100 mmHg prompt caution with any compressive therapy or sharp debridement
Ankle Pressure < 70 mmHg
- Indicates critical limb ischaemia (CLI) territory when ulceration or tissue loss is present
- Per Schwartz's Principles of Surgery: "For patients with ulcers or gangrene, the presence of CLI is suggested by an ankle pressure less than 70 mmHg or a toe systolic pressure less than 50 mmHg"
- At this level:
- Healing of wounds is severely impaired — active tissue repair demands far more perfusion than intact skin maintenance
- Any existing ulceration is unlikely to heal without vascular intervention
- Urgent vascular surgical referral is indicated
- Corresponds approximately to Fontaine Stage III–IV or Rutherford Category 4–5 (rest pain / minor tissue loss)
- UK podiatry implication: compression bandaging is absolutely contraindicated; no elective podiatric procedures; patient requires immediate onward referral via the vascular pathway
Ankle Pressure < 50 mmHg
- Indicates severe critical limb ischaemia with a high risk of limb loss
- Per Schwartz's: "Ischaemic rest pain most commonly occurs below an ankle pressure of 50 mmHg or a toe pressure less than 30 mmHg"
- At this level:
- The patient will typically have ischaemic rest pain — pain at rest (especially nocturnal), often relieved by hanging the leg dependent
- Existing tissue loss / gangrene is present or imminent
- Limb salvage requires urgent revascularisation (angioplasty, bypass, or stenting)
- Without intervention, major amputation is likely within weeks to months
- Corresponds to Rutherford Category 4–6 / Fontaine Stage III–IV
Summary Table
| Ankle Systolic Pressure | Clinical Interpretation | Podiatry Action |
|---|---|---|
| >100 mmHg | Normal / adequate perfusion | Routine care appropriate |
| 70–100 mmHg | PAD present; compromised healing | Caution; avoid compression; monitor; consider vascular referral |
| < 70 mmHg (with ulcer/tissue loss) | Critical limb ischaemia — wound healing unlikely | Urgent vascular referral; no compression; no elective procedures |
| < 50 mmHg | Severe CLI — rest pain; limb threatened | Emergency vascular referral; risk of amputation |
| < 40 mmHg | Severe CLI — corresponds to Rutherford Cat 4 (rest pain) | Same as above; anticipate rest pain and rapid tissue loss |
Rutherford / Fontaine Classification (for context)
| Fontaine | Rutherford | Clinical | Objective Criteria (Ankle Pressure) |
|---|---|---|---|
| I | 0–1 | Asymptomatic / mild claudication | Normal or >50 mmHg post-exercise |
| IIa/IIb | 2–3 | Moderate–severe claudication | Post-exercise AP <50 mmHg |
| III | 4 | Ischaemic rest pain | Resting AP <40 mmHg |
| IV | 5–6 | Tissue loss / gangrene | Resting AP <60 mmHg (minor loss); <40 mmHg (major loss) |
(AP = ankle pressure; PVR = pulse volume recording)
Important Caveats in UK Podiatric Practice
-
Calcified / non-compressible vessels — Ankle pressures can be falsely elevated in diabetes and renal failure due to medial calcinosis. An ankle pressure >200 mmHg or a non-compressible artery should prompt toe pressure or ABPI with toe brachial pressure index (TBPI) instead (toe pressure <30 mmHg = CLI; toe pressure <70 mmHg = impaired healing)
-
ABPI vs. absolute pressure — The ABPI ratio is more commonly used in UK vascular screening. An ABPI <0.5 roughly correlates with ankle pressures in the CLI range; ABPI <0.9 indicates PAD
-
Wound healing thresholds are higher than rest pain thresholds — tissue repair requires more perfusion than maintaining intact skin, which is why the wound healing threshold (~70 mmHg) is above the rest pain threshold (~50 mmHg)
-
Doppler waveform quality should be assessed alongside the pressure — a monophasic or absent waveform with a borderline pressure carries greater clinical concern than the same pressure with a biphasic waveform
— Schwartz's Principles of Surgery, 11th Ed. | Pfenninger & Fowler's Procedures for Primary Care, 3rd Ed.
what advice can you give a patient with a API of lower than 100
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Excellent — comprehensive information gathered. Here is the patient advice:
Patient Advice: Ankle Pressure Below 100 mmHg (PAD)
Quick note on terminology: You said "API" — I'll assume you mean ankle systolic pressure below 100 mmHg, which indicates peripheral arterial disease (PAD). If you meant ABPI (Ankle-Brachial Pressure Index) below 1.0, the same advice applies — both indicate reduced arterial blood flow to the feet and legs.
An ankle pressure below 100 mmHg means the blood supply to the lower limb is reduced. The advice below covers what to tell the patient across all the key areas.
1. Smoking Cessation — Most Important Single Action
- Stop smoking immediately — smoking is the single most damaging risk factor for PAD and directly causes the arteries to narrow further
- Smoking significantly increases the risk of PAD progressing to critical limb ischaemia, amputation, heart attack, and stroke
- Smoking cessation is associated with decreased mortality and improved amputation-free survival
- Refer to NHS Stop Smoking Services — nicotine replacement therapy, varenicline (Champix), or bupropion can all help
- Even cutting down helps, but complete cessation is the goal
2. Foot Care — Critical in Podiatry Practice
Because the blood supply is reduced, the feet are at risk of ulceration that will not heal:
- Inspect both feet every day — look at the tops, soles, between the toes, and around the heels; use a mirror if needed or ask someone to help
- Report any new sores, blisters, cuts, colour changes, or wounds immediately — do not wait; even a small cut can become serious
- Never walk barefoot — always wear shoes or slippers, even indoors
- Avoid extremes of temperature — do not use hot water bottles, heated insoles, or sit too close to radiators (reduced sensation means burns can go unnoticed)
- Do not cut corns or hard skin yourself — see your podiatrist; home cutting risks unnoticed injury
- Moisturise dry skin daily (but not between the toes — moisture between toes encourages fungal infection)
- Cut toenails straight across — or have them cut by a podiatrist
- Check shoes and socks before putting them on for any objects, rough seams, or debris
3. Footwear Advice
- Wear well-fitting, supportive shoes with a wide toe box — avoid tight, narrow, or pointed shoes
- Avoid high heels — they increase forefoot pressure and reduce circulation
- Seam-free socks reduce friction; avoid tight elastic sock tops that constrict circulation
- Consider podiatric footwear assessment — if there are areas of high pressure, cushioned insoles or off-loading footwear can reduce ulceration risk
4. Exercise
- Supervised walking exercise is recommended — a structured programme of walking to the point of claudication pain, resting, then repeating
- Regular exercise improves collateral circulation, walking distance, and quality of life
- Aim for at least 30 minutes, 3 times per week, gradually increasing
- Refer to a supervised exercise programme (available on the NHS for PAD patients)
- Exercise has been shown to improve symptoms comparably to some interventional procedures in mild-to-moderate PAD
5. Cardiovascular Risk Factor Control
PAD is a cardiovascular disease equivalent — patients with PAD have the same high risk of heart attack and stroke as someone with known coronary artery disease. This must be taken seriously:
| Risk Factor | Target / Action |
|---|---|
| Blood pressure | Target <130/80 mmHg (especially if diabetic or renal disease) |
| Cholesterol (LDL) | Target <1.8 mmol/L (<70 mg/dL); high-intensity statin recommended for all PAD patients |
| Blood sugar (if diabetic) | HbA1c target <53 mmol/mol (7%); poor glucose control accelerates vascular disease |
| Weight | Aim for BMI <25; weight loss reduces cardiovascular load |
- Statins — all patients with PAD should be on a statin; it reduces cardiovascular events, slows PAD progression, and improves walking distance
- Antiplatelet therapy — aspirin (75 mg daily) or clopidogrel (75 mg daily) is recommended to reduce the risk of heart attack, stroke, and death; this is a GP/medical decision
6. Diet
- Heart-healthy diet: low saturated fat, low salt, low refined sugar, high in fruit, vegetables, and wholegrains (Mediterranean-style diet)
- Reduce processed food and red meat
- Stay well hydrated — dehydration thickens blood and worsens circulation
7. When to Seek Urgent Help
Tell the patient to contact their GP or podiatrist urgently (same day) if they notice:
- A new ulcer, wound, or area of skin breakdown that does not heal within 2 weeks
- Sudden worsening of pain in the foot or leg, including pain at rest or at night (rest pain = worsening ischaemia)
- The foot becoming cold, white, blue, or numb suddenly (this is a vascular emergency — call 999)
- Increasing redness, swelling, or discharge from any foot wound (infection in an ischaemic foot is limb-threatening)
8. Monitoring & Follow-Up
- Regular podiatry review — frequency depends on risk level; at minimum annually, more often if wound care is needed
- Vascular review — GP should refer to vascular surgery if symptoms progress or ankle pressure falls further
- Do not ignore symptoms — PAD is a progressive condition, but risk factor control significantly slows progression
Summary Card for the Patient
| Do | Don't |
|---|---|
| Check feet daily | Smoke |
| Wear good-fitting shoes | Walk barefoot |
| Exercise regularly (supervised walking) | Use hot water bottles on feet |
| Take all medications prescribed (statin, antiplatelet) | Cut your own corns or hard skin |
| See your podiatrist regularly | Ignore new wounds or colour changes |
| Control blood pressure, cholesterol, blood sugar | Wear tight socks or elastic-topped hosiery |
| Report rest pain or sudden colour change urgently | Delay seeking help |
— Mulholland & Greenfield's Surgery, 7th Ed. | Sabiston Textbook of Surgery | Fuster & Hurst's The Heart, 15th Ed.
risk factors, pathophysiology, assessment and management, appropriately designed foot orthosis, gait deviations and clinical tests podiatry UK for plantar plate dysfunction
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"plantar plate" AND ("lesser metatarsophalangeal" OR "MTP joint") AND (orthosis OR orthotic OR management)
I now have all the content needed for a comprehensive answer. Let me compile it fully.
Plantar Plate Dysfunction — Comprehensive Podiatry (UK) Reference
1. Anatomy Recap
The plantar plate is a dense fibrocartilaginous thickening of the plantar MTP joint capsule. It attaches firmly distally to the base of the proximal phalanx and loosely proximally to the metatarsal neck — the proximal attachment is the consistent site of tearing. It is the primary static restraint against dorsal subluxation and hyperextension of the MTP joint.
Key connections:
- Deep transverse intermetatarsal ligament → links adjacent plantar plates
- Accessory collateral ligaments (metatarsoglenoid suspensory ligaments) → attach to medial/lateral borders
- Extensor sling (transverse lamina) → connects dorsally
- Flexor tendon sheath and plantar fascia → plantar attachments
2. Risk Factors
Intrinsic (Structural/Biomechanical)
| Risk Factor | Mechanism |
|---|---|
| Long 2nd metatarsal (Greek foot / Morton's foot) | Excessive loading under 2nd MTP during propulsion |
| Hallux valgus | Lateral load transfer to 2nd MTP; hallux no longer shares propulsive load |
| Hypermobile 1st ray | 1st ray dorsiflexes under load → 2nd MTP bears excess forefoot force |
| Short 1st metatarsal (Morton's foot pattern) | Same load transfer mechanism as above |
| Pes planus / overpronation | Medial column collapse increases 2nd MTP stress; prolonged pronation disrupts toe-off mechanics |
| Cavus foot | Rigid forefoot forces — increased metatarsal head loading |
| Equinus deformity / tight gastrocnemius | Ankle plantarflexion restriction increases forefoot compensatory dorsiflexion during propulsion |
| Hammer toe / claw toe | Retrograde pressure from toe contracture drives metatarsal head plantarly |
| Inflammatory arthropathy (RA, gout, psoriatic) | Synovitis and soft tissue attenuation destabilise the joint; pannus erodes fibrocartilage |
Extrinsic (Footwear / Activity)
| Risk Factor | Mechanism |
|---|---|
| High-heeled shoes | Sustained MTP hyperextension loads the plantar plate against the metatarsal neck |
| Narrow toe box | Compresses lesser digits, accelerating deformity |
| Repetitive high-impact loading | Runners, court sports players — cumulative microtrauma |
| Sudden increase in training load | Overuse — common in runners |
Iatrogenic
- Corticosteroid injection into the MTP joint — directly attenuates the plantar plate fibrocartilage; the most well-documented iatrogenic cause of crossover toe deformity
3. Pathophysiology
The injury follows a predictable mechanical cascade:
Stage 1 — Synovitis / Capsulitis (Grade 0)
Repetitive hyperextension forces at the MTP joint cause reactive synovitis. The plantar plate is intact but the capsule is inflamed. Pain and swelling at the MTP joint without instability.
Stage 2 — Plantar Plate Attenuation (Grade 1)
Chronic overloading causes progressive degeneration of the fibrocartilage — particularly at the proximal insertion on the metatarsal neck. Partial thickness tearing begins, initially on the medial or lateral side. The toe begins to show subtle dorsal drift under load.
Stage 3 — Partial Tear with Instability (Grade 2)
A transverse partial-to-full thickness tear develops at the proximal attachment. The intrinsic muscles (lumbricals and interossei) — which normally act plantar to the MTP joint axis to assist plantarflexion — become less effective as the MTP joint subluxes dorsally, eventually migrating dorsal to the axis and actively worsening the deformity (analogous to the intrinsic-minus mechanism in claw toe). The flexor digitorum longus and brevis can no longer maintain toe purchase.
Stage 4 — Complete Tear / Collateral Involvement (Grade 3)
Full thickness tear with extension into the collateral ligaments. If the lateral collateral ligament is also attenuated, the 2nd toe deviates medially toward the hallux — the classic crossover toe deformity (Fig. 6.49 below). The toe subluxes or dislocates dorsally.
Stage 5 — Fixed Dislocation / Deformity (Grade 4)
Button-hole tear with complete MTP dislocation. The proximal phalanx dislocates dorsally. A fixed hammer toe or crossover toe deformity results. Increasing load is transmitted through the metatarsal head, perpetuating plantar metatarsalgia and intractable plantar keratosis.
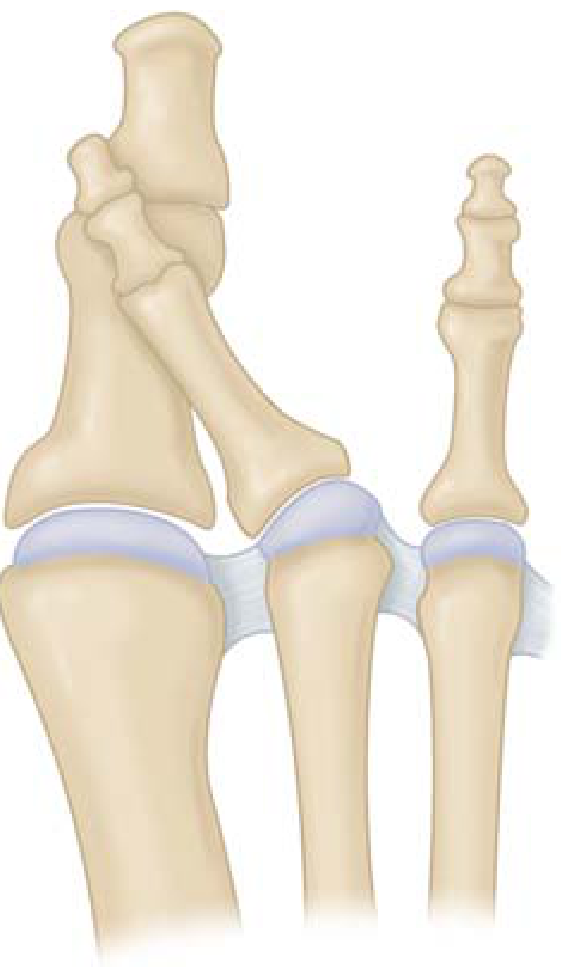
Crossover-toe deformity: the 2nd toe drifts dorsomedially over the hallux when the plantar plate and lateral collateral ligament fail — Miller's Review of Orthopaedics, 9th Ed.
MRI appearance of plantar plate injury:
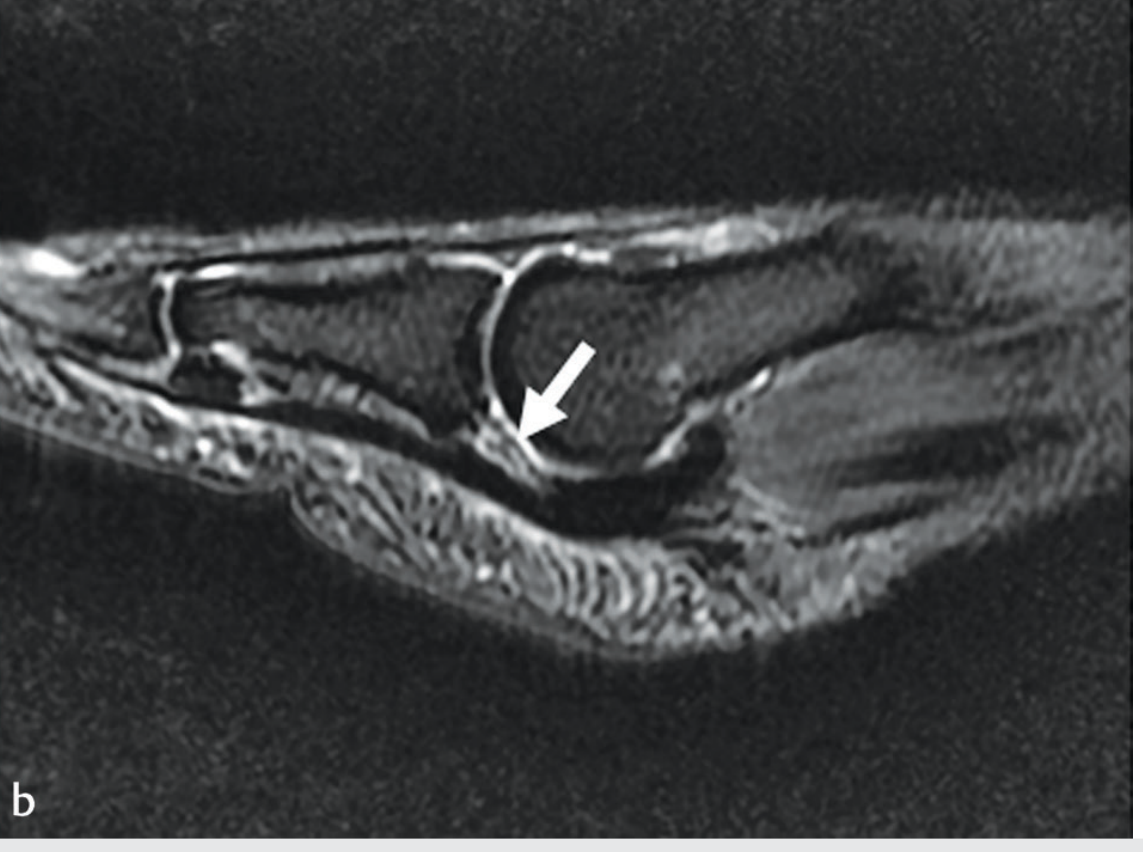
Sagittal MRI showing increased signal at the distal plantar plate (arrow) consistent with tear; the plate is displaced proximally — Imaging Anatomy: Bones, Joints, Vessels & Nerves
4. Assessment
Subjective History
- Location: plantar/plantar-lateral 2nd (most common) or 3rd MTP joint
- Character: aching, pressure-like, "walking on a stone" or "walking on a lump"
- Aggravating factors: barefoot walking, propulsion, heel raise, high heels
- Time course: insidious onset — often weeks to months before presentation
- Footwear history: high heels, narrow toe box
- Activity level: runners, court sports
- Previous injections into or around the MTP joint (iatrogenic risk)
- Associated deformity: progressive toe drift, crossing over hallux
Observation (Static and Dynamic)
| Finding | Significance |
|---|---|
| Plantar callosity under 2nd/3rd metatarsal head | Metatarsal head overloading from plantarly displaced head |
| Toe dorsal float (2nd toe not in contact with floor in stance) | Loss of flexor purchase / dorsal subluxation |
| Crossover toe — 2nd toe medially deviated over hallux | Advanced PPD with collateral ligament attenuation |
| Swelling / fusiform "sausage" toe | Capsular synovitis |
| Hammer toe configuration at the affected digit | Secondary to MTP hyperextension and proximal phalanx dorsal drift |
5. Clinical Tests
Test 1: Anterior (Lachman) Drawer Test — Most Sensitive Test
- Stabilise the metatarsal shaft between thumb and index finger of one hand
- Grasp the proximal phalanx of the affected digit between thumb and index finger of the other hand
- Apply a sharp dorsal thrust — push the toe upwards/dorsally
- Positive: reproduction of the patient's plantar pain at the MTP joint, or excessive dorsal translation (>2 mm versus adjacent toes), or subluxation/dislocation
- Clinical note: a positive result in the absence of visible deformity is the classic presentation of MTP instability / early PPD
Dorsoplantar drawer test. Pain or subluxation on dorsal thrust confirms MTP instability / plantar plate injury — Miller's Review of Orthopaedics, 9th Ed.
Test 2: Paper Pull-Out / Toe Purchase Test (Kelikian Test)
- Place a sheet of paper or thin card under all lesser toes with the patient standing
- Ask the patient to actively push the toes down and grip the paper
- Attempt to pull the paper from under the affected toe
- Positive: paper slides out easily under the affected digit — indicates loss of active flexor purchase (FDB/FDL) due to plate incompetence and dorsal subluxation
Test 3: Varus/Valgus Stress Test
- With the MTP joint held in neutral, apply a medial (varus) then lateral (valgus) stress to the proximal phalanx
- Assess for medial or lateral laxity compared with the adjacent toes
- Positive: excessive medial laxity (lateral collateral attenuation) in crossover toe; or lateral laxity (medial collateral) depending on deformity direction
- Grading: compare bilaterally
Test 4: Digital Compression Test
- Compress the MTP joint from dorsal to plantar using thumb and index finger
- Positive: localised plantar tenderness directly under the metatarsal head
- Useful for differentiating from interdigital neuroma (which has positive Mulder's click, tenderness in the interspace rather than under the metatarsal head)
Test 5: Single-Leg Heel Raise Assessment
- Ask the patient to perform a single-leg heel raise, observing the toe in the sagittal plane
- Positive: the affected digit fails to plantarflex and purchase the ground during the heel raise
- Indicates inability of the flexor complex to maintain sagittal plane stability — confirms functional plantar plate insufficiency
- Compare bilaterally
Test 6: Passive MTP Dorsiflexion Provocation
- With the ankle in neutral, passively dorsiflex the MTP joint to approximately 90°
- Apply downward pressure on the metatarsal head
- Positive: pain reproduced at the plantar MTP joint
- Simulates the loading pattern during toe-off that stresses the plantar plate
Differential Diagnosis to Exclude
| Condition | Differentiating Feature |
|---|---|
| Interdigital (Morton's) neuroma | Mulder's click; pain in interspace not under metatarsal head; 3rd/4th web space typical |
| Freiberg's disease | AVN of metatarsal head; X-ray changes (flattening); adolescent onset common |
| Rheumatoid arthritis | Bilateral; systemic features; RF/anti-CCP positive; multiple MTP joints |
| Stress fracture | Point tenderness on metatarsal shaft; positive tuning fork test; X-ray/MRI |
| Flexor tendon pathology | Pain on resisted plantarflexion; along tendon not under metatarsal head |
6. Gait Deviations
Plantar plate dysfunction produces characteristic gait deviations visible on clinical gait analysis:
| Gait Phase | Deviation | Mechanism |
|---|---|---|
| Loading response | Antalgic gait — shortened stance phase on affected side | Pain avoidance |
| Midstance | Excess supination of forefoot / lateral weight transfer | Offloading the painful 2nd MTP joint |
| Terminal stance / toe-off | Reduced or absent MTP joint dorsiflexion (propulsion avoidance) | Pain during push-off; patient initiates swing early to avoid peak MTP extension |
| Toe-off | Loss of toe purchase — affected digit does not plantarflex or grip the ground | Flexor mechanism incompetence; dorsal float of the digit |
| Swing phase | Compensatory hip hitching or circumduction | Clearing a dorsally subluxed or hammer digit |
| Stance overall | Vaulting gait (early heel rise) | Avoidance of terminal stance MTP loading |
| Foot progression angle | Increased external rotation / toe-out stance | Decreases MTP dorsiflexion demand by altering the axis of propulsion |
| Knee/hip | Increased knee flexion at toe-off; shortened stride length | Downstream compensation for reduced forefoot propulsion |
Clinical observation tip: Observe from the front — a crossover toe drifting over the hallux may only become apparent dynamically in propulsion. Observe from the side during walking for loss of toe purchase in terminal stance.
7. Orthotic / Insole Management
The goals of orthotic prescription are:
- Offload the plantar plate — reduce compressive and shear force at the MTP joint
- Restore sagittal plane toe alignment — maintain the toe in plantarflexion
- Reduce MTP dorsiflexion moment during propulsion
- Address biomechanical drivers — equinus, hallux valgus, hypermobile 1st ray, etc.
Element 1: Metatarsal Dome / Metatarsal Pad
- Placement: proximal to the metatarsal head(s), at the proximal 1/3 of the metatarsal shaft — not under the metatarsal head
- Function: elevates the metatarsal shaft, depresses the metatarsal head relative to ground, redistributes load away from the symptomatic MTP joint
- Specification: 3–5 mm semi-compressed felt or PPT foam dome, teardrop shape; for a custom device, incorporate into the shell as a built-in raise
- Common error: placing the pad too distally (under or distal to the metatarsal head) — this increases loading, not reduces it
Element 2: Toe Prop / Digit Prop
- Placement: under the plantar aspect of the proximal phalanx of the affected digit
- Function: mechanically maintains the proximal phalanx in plantarflexion, restoring the flexor tendon's line of action and preventing dorsal subluxation
- Materials: medical grade silicone (custom moulded), or PPT/plastazote toe prop
- A combined loop-and-prop style silicone device can be prescribed — the proximal loop anchors over the digit, the distal pad sits under the proximal phalanx
- Essential in grade 2–3 dysfunction where passive plantarflexion is lost
Element 3: Forefoot Extension / Stiff Forefoot Platform
- A full-length orthotic shell (polypropylene or carbon fibre) with a rigid forefoot extension limits MTP dorsiflexion during terminal stance
- The stiff forefoot platform acts as a functional rocker — propulsion occurs over the rigid plate rather than through the MTP joints
- Rocker-sole modification to the shoe augments this effect; a forefoot rocker placed proximal to the MTP joints is the most effective shoe modification for offloading PPD
Element 4: Medial Arch Support / Rearfoot Posting
- If pes planus / overpronation is a driver:
- Medial longitudinal arch support — semi-rigid or custom orthosis with a medial skive or medial flange
- Rearfoot varus posting (3–5°) to control subtalar pronation and reduce medial column collapse
- This indirectly reduces the duration and magnitude of the propulsive load on the 2nd MTP joint
- If hallux valgus is contributing: incorporate a 1st ray cutout (Morton's extension reversed) or medial toe spacer
Element 5: First Ray Cutout / Kinetic Wedge
- A 1st ray cutout beneath the 1st metatarsal head encourages 1st ray plantarflexion
- This promotes normal load sharing through the 1st MTP joint, reducing the lateral transfer of load that overloads the 2nd MTP
- Particularly useful when 1st ray hypermobility is the primary driver
Element 6: Heel Raise
- A 3–6 mm heel raise (bilateral to avoid leg length discrepancy) reduces gastrocnemius contribution to equinus and decreases forefoot dorsiflexory demand
- Indicated when ankle equinus is a contributing factor
Summary Orthotic Prescription Template
| Component | Specification | Indication |
|---|---|---|
| Shell | Custom polypropylene, full-length | All grades ≥2 |
| Metatarsal dome | 3–5 mm PPT, proximal to 2nd MTH | All grades |
| Toe prop / digit pad | Silicone or PPT, under proximal phalanx of affected digit | Grade 2–4 |
| Forefoot extension | Semi-rigid EVA or carbon forefoot plate | Moderate–severe |
| Rocker sole (shoe modification) | Forefoot rocker proximal to MTPJ | Severe / surgical bridge |
| Medial arch | Semi-rigid with medial skive | Pronated foot type |
| 1st ray cutout | 3–5 mm recess under 1st MTH | Hypermobile 1st ray / HV |
| Heel raise | 3–6 mm EVA | Equinus present |
8. Conservative Management Summary
| Intervention | Details |
|---|---|
| Buddy taping / plantar-flexion taping | Plantarflexes the proximal phalanx onto the metatarsal head; reduces dorsal shear; use Leukotape P or zinc oxide tape; reassess skin integrity at each visit |
| Foot orthosis | As above — mainstay of podiatric management |
| Footwear advice | Stiff sole, wide toe box, low heel (<2 cm), seam-free; avoid flip-flops and minimalist shoes |
| Activity modification | Reduce hill running, court sports, barefoot activity in the acute phase |
| Intrinsic muscle strengthening | Towel scrunches, marble pick-up, toe spread exercises — strengthens lumbricals and interossei to restore dynamic sagittal plane stability |
| Stretching | Gastrocnemius and soleus stretching — reduces equinus-driven forefoot loading |
| NSAIDs | Short-term for pain and synovitis management |
| Do NOT inject corticosteroid | Contraindicated — risks iatrogenic plate attenuation and accelerated deformity |
| Imaging referral | Ultrasound (dynamic, first-line in UK) or MRI/MR arthrogram if grading needed or surgical referral planned |
| Surgical referral | After 3–6 months failed conservative management; earlier if grade 3–4 or progressive deformity |
9. Classification — Thompson & Hamilton Grading (UK Standard)
| Grade | Pathology | Clinical Findings | Management |
|---|---|---|---|
| 0 | Synovitis/capsulitis — plate intact | Pain, swelling; negative drawer | Conservative: taping, padding, footwear |
| 1 | Partial thickness tear (medial/lateral) | Positive drawer; minimal laxity | Conservative: orthosis, taping, intrinsic rehab |
| 2 | Complete transverse tear, distal | Positive drawer; dorsal float; loss of toe purchase | Orthosis + toe prop; consider surgical referral |
| 3 | Extensive tear + collateral involvement | Crossover toe; varus/valgus laxity | Surgical referral likely |
| 4 | Button-hole tear; MTP dislocation | Fixed crossover/hammer toe | Surgical reconstruction |
— Miller's Review of Orthopaedics, 9th Ed. | Imaging Anatomy: Bones, Joints, Vessels & Nerves (Thieme)
This is a shared conversation. Sign in to Orris to start your own chat.