plantar plate dysfunction
Reading File
Finding Sources
Finding Sources
Searching Images
plantar plate anatomy metatarsophalangeal joint
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of plantar plate dysfunction, based on authoritative orthopaedic and imaging anatomy sources.
Plantar Plate Dysfunction
Anatomy
The plantar plate is a fibrocartilaginous thickening of the plantar joint capsule at the metatarsophalangeal (MTP) joint. It is:
- Distally attached firmly to the plantar base of the proximal phalanx
- Proximally attached loosely to the metatarsal neck (via synovial tissue)
- Interconnected to adjacent plantar plates by the deep transverse metatarsal ligaments
- Connected dorsally to the accessory collateral ligament and the extensor sling (transverse lamina)
- Plantar to it run the flexor digitorum longus and brevis in their sheaths
- Reinforced laterally by proper and accessory collateral ligaments
At the first MTP joint, the plantar plate incorporates the sesamoid apparatus — each sesamoid is embedded in the flexor hallucis brevis tendon, with the intersesamoid ligament crossing the proximal plate and sesamophalangeal ligaments thickening its sides.
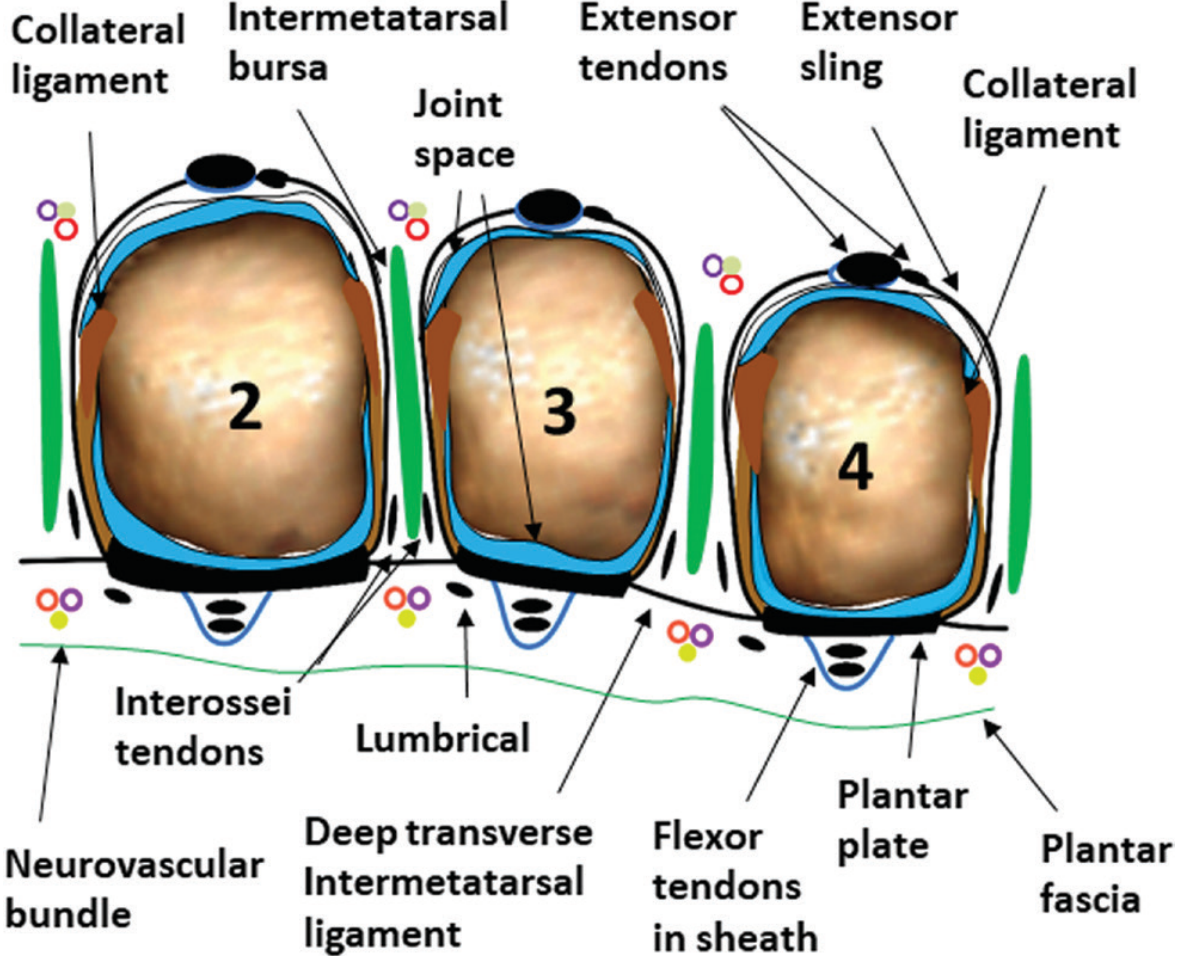
Schematic of lesser MTP joints (2–4). The plantar plate sits plantar to the joint capsule, deep to the flexor tendons, interconnected by the deep transverse intermetatarsal ligament. — Imaging Anatomy: Bones, Joints, Vessels and Nerves
Pathomechanics
The plantar plate is the key stabiliser of the MTP joint against dorsal subluxation. Disruption occurs via:
- Chronic overload / degenerative attrition — most common in lesser toes, especially the 2nd
- Acute hyperextension (turf toe) — in the hallux, during athletic push-off on artificial turf
- Plantar flexion injury ("sand toe") — hallux, less common
- Iatrogenic attenuation — from intra-articular steroid injections into the MTP joint
Tears typically originate at the distal insertion (phalangeal base) and progress proximally.
Clinical Presentations
| Condition | Features |
|---|---|
| MTP joint instability | Pain and swelling without deformity; mild subluxation; common in runners and racquet sport athletes |
| Crossover-toe deformity | 2nd toe deviates dorsomedially over the hallux; requires plantar plate disruption + lateral collateral ligament attenuation |
| Hammer toe / dorsal dislocation | Progressive dorsal subluxation of the MTP joint as the plantar plate fails; increased load on metatarsal head causing metatarsalgia |
| Turf toe | Hallux MTP hyperextension injury; acute plantar plate/capsule tear or avulsion; inability to push off forcefully |
Diagnosis
Clinical examination:
- Anterior drawer test (dorsoplantar) — most sensitive test; positive when pain is reproduced with dorsal displacement of the proximal phalanx on the metatarsal head
- Swelling, plantar tenderness at the MTP joint
- Deformity (crossover toe, dorsal subluxation) in advanced cases
Imaging:
- Plain radiographs — assess alignment, subluxation, dislocation
- MRI / MR arthrogram — gold standard for soft-tissue assessment; identifies plantar plate tears, collateral ligament injuries, and synovitis. MR arthrogram preferred when diagnosis is uncertain. On MRI, tears appear as focal hyperintensity (T2) within the normally hypointense plate, or morphological thickening/heterogeneity
- Ultrasound — useful for dynamic assessment of MTP joint instability
Grading of Plantar Plate Tears
| Grade | Description |
|---|---|
| 0 | Attenuation/elongation; no frank tear |
| 1 | Transverse partial tear < 50% width |
| 2 | Transverse partial tear > 50% width |
| 3 | Complete transverse tear |
| 4 | Extensive tear with button-hole deformity |
Management
Non-operative:
- Toe taping in plantarflexion / corrective splints — reduce pain but do not permanently correct deformity
- Lesser-toe orthotics, metatarsal pads
- Activity modification
- Steroid injections are contraindicated — risk of iatrogenic plantar plate attenuation and crossover-toe deformity
Operative:
- MTP synovectomy + capsular reconstruction — for isolated synovitis/instability without deformity
- Plantar plate repair — for complete tears; typically requires a shortening (Weil) osteotomy of the distal metatarsal to decompress the joint and aid visualization; results are promising, especially in high-level athletes
- Flexor-to-extensor tendon transfer — with medial collateral ligament release for crossover-toe deformity; provides good MTP joint stability
- EDB tendon transfer (rerouted plantar to intermetatarsal ligament) — for less severe deformities; preserves more MTP joint mobility than flexor-to-extensor transfer
- Weil osteotomy alone — for severe MTP subluxation/dislocation
— Miller's Review of Orthopaedics, 9th Edition; Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3
This is a shared conversation. Sign in to Orris to start your own chat.