Complications of regional anaesthesia from miller’s Stoelting Morgan and all standard textbooks
Read multiple sections from anesthesiology textbooks about complications of regional anesthesia and return ALL the content. Read the following files at the specified offsets: 1. Miller's Anesthesia block24 - the dedicated "Complications of Regional Anesthesia" chapter: File: /textbooks/9780323935920/9780323935920_block24.md Read from line 2539 onward. Read in chunks of 100 lines each until you reach the end of the section (or 600 lines total). 2. Miller's Anesthesia block30 - COMPLICATIONS section: File: /textbooks/9780323935920/9780323935920_block30.md Read from line 2180 to 2350 (offset=2180, limit=170) 3. Morgan and Mikhail's Clinical Anesthesiology (isbn 9781260473797) - search for complications of regional anesthesia sections. Use this SQL query via query_library_db: SELECT title, book_title, '/textbooks/' || block_file_path AS file_path, line_number, para_line_ranges, para_count FROM headings_fts WHERE headings_fts MATCH 'complication* regional' AND book_isbn = '9781260473797' ORDER BY rank LIMIT 10 4. Barash/Stoelting (isbn 9781975199074) - search for complications of regional anesthesia: SELECT title, book_title, '/textbooks/' || block_file_path AS file_path, line_number, para_line_ranges, para_count FROM headings_fts WHERE headings_fts MATCH 'complication* regional' AND book_isbn = '9781975199074' ORDER BY rank LIMIT 10 Return ALL content you find, organized by source. Include every detail about specific complications, their mechanisms, incidence, prevention and management. Do not summarize or omit details.
An error occurred (internalServerException) when calling the ConverseStream operation: The system encountered an unexpected error during processing. Try your request again.
We encountered an error while processing your request. Please try again or reach out to us for help.
See again
Complications of Regional Anaesthesia
Classification
- Excessive physiological responses to correctly placed drugs
- Complications from needle/catheter placement
- Drug toxicity
A. NEURAXIAL BLOCK COMPLICATIONS
1. Hypotension
- Bradycardia co-exists when cardioaccelerator fibres (T1–T4) are blocked
- Exaggerated in hypovolaemic, elderly, pregnant, and obese patients
- Treatment: IV fluids, left uterine displacement (in obstetrics), vasopressors (phenylephrine, ephedrine, epinephrine), atropine for bradycardia
2. High / Total Spinal Anaesthesia
- Onset is rapid because epidural/caudal doses are 5–10× the intrathecal dose
- Features: severe hypotension, bradycardia, respiratory insufficiency, unconsciousness, apnea
- Apnoea is more often from medullary hypoperfusion than phrenic nerve (C3–C5) paralysis
- Treatment: supportive — airway management, intubation/mechanical ventilation, IV vasopressors, IV fluids, atropine/epinephrine for bradycardia
3. Cardiac Arrest During Spinal Anaesthesia
- Incidence as high as 1:1500 in prospective studies (Morgan & Mikhail)
- Often preceded by bradycardia; notably occurs in young, healthy patients
- Contributed to by oversedation, unrecognised hypoventilation, hypoxia, and rapid vasovagal response
- Prompt treatment of hypotension and bradycardia is mandatory
4. Subdural Injection
- Accidental injection into the potential space between dura and arachnoid
- Much more serious with epidural doses than spinal doses
- Clinical features: similar to high spinal, but onset delayed 15–30 min and block may be "patchy"
- Space extends intracranially — anesthetic can ascend to high levels
- Treatment: supportive; effects last 1 to several hours
5. Urinary Retention
- Block of S2–S4 sacral roots inhibits detrusor contraction
- More common with long-acting agents and intrathecal opioids
- May require urinary catheterisation
6. Horner Syndrome
- Occurs when cervical sympathetic chain (T1 fibres to stellate ganglion) is blocked
- Features: ptosis, miosis, anhidrosis ipsilaterally
- Usually transient and not dangerous per se; alerts clinician to high block
B. POST-DURAL PUNCTURE HEADACHE (PDPH)
- Mechanism: CSF leakage → vascular hyperaemia, migraine-type physiology, traction on pain-sensitive structures
- Character: bilateral, frontal/retroorbital/occipital, extending into neck; throbbing or constant; associated with photophobia and nausea
- Hallmark: postural — worse with sitting/standing, relieved by lying flat
- Onset: typically 12–72 hours after dural puncture
- Incidence: relates to needle size and tip shape (cutting > pencil-point needles); unintentional dural puncture with epidural needle has 30–60% PDPH rate
- Incidence of unintentional dural puncture during labor epidural: 1–1.5%
- Conservative: oral hydration, caffeine (mild vasoconstrictive effect), NSAIDs, acetaminophen, opioids, bed rest
- Definitive: Epidural Blood Patch (EBP) — 15–20 mL autologous blood injected into epidural space; 16.8% require a second patch, 1.5% require three
- If cranial nerve involvement (e.g., diplopia from CN VI palsy), EBP is urgent
- Note: muffled hearing with PDPH is not CN involvement but reflects middle ear pressure change via cochlear aqueduct
C. SPINAL/EPIDURAL HAEMATOMA
- Incidence: ~1:150,000 for epidural blocks; ~1:220,000 for spinal anaesthetics (Morgan & Mikhail)
- Needle/catheter trauma to epidural veins causes bleeding; vast majority in patients with abnormal coagulation (disease or drugs)
- Can occur at catheter insertion or removal
- Onset typically more sudden than abscess
- Sharp back pain + leg pain
- Motor weakness and/or sphincter dysfunction (urinary/bowel)
- Urgent MRI or CT + neurosurgical consultation
- Prompt surgical decompression (laminectomy) — neurological outcome correlates with degree of deficit at time of diagnosis
- Good recovery possible if decompressed promptly
D. MENINGITIS AND ARACHNOIDITIS
- Infection of the subarachnoid space from contamination of equipment, injected solutions, or organisms tracked in from skin
- Indwelling catheters may become colonised with skin organisms
- Strict sterile technique is mandatory
- Symptoms: fever, nuchal rigidity, photophobia, headache
- May initially mimic PDPH — distinction is critical
E. EPIDURAL ABSCESS
- Rare but potentially devastating complication of neuraxial anaesthesia
- Incidence: 1:6,500 to 1:500,000 epidurals
- Most cases involve epidural catheters (mean 5 days from insertion to symptoms, though may be weeks)
- Most common organisms: Staphylococcus aureus and S. epidermidis
- Back pain intensified by percussion over the spine
- Nerve root / radicular pain
- Motor/sensory deficits or sphincter dysfunction
- Paraplegia or paralysis
- Remove catheter (tip for culture), blood cultures, injection site examination
- Anti-Staphylococcus antibiotics empirically
- Urgent MRI/CT
- Surgical decompression (laminectomy) ± percutaneous drainage
- Infectious disease + neurosurgical consultation
- Minimise catheter manipulations; maintain closed system
- Use bacterial filters
- Limit duration of indwelling catheters
F. NEUROLOGICAL INJURY / NERVE INJURY
Neural Injury from Needle/Catheter
- Nerve root damage from direct needle trauma or intraneural injection
- Spinal cord damage — rare; more likely with epidural above the conus medullaris
- Cauda equina syndrome — associated with continuous spinal anaesthesia and hyperbaric lidocaine (maldistribution/pooling of concentrated local anaesthetic in sacral roots)
Transient Neurological Symptoms (TNS)
- Associated especially with intrathecal lidocaine
- Bilateral burning/aching pain in buttocks radiating to legs after recovery from spinal block
- Usually resolves within 72 hours
- More common with lithotomy position
Pre-existing Neurological Disease
- Patients with pre-existing spinal stenosis, disc disease, or prior spine surgery are at higher risk of neurological complications after neuraxial block
- "Double crush" phenomenon — compromised nerve more vulnerable to additional injury
G. LOCAL ANAESTHETIC SYSTEMIC TOXICITY (LAST)
- Perioral tingling, metallic taste, tinnitus
- Light-headedness, visual disturbances, auditory changes
- Agitation, confusion, slurred speech
- Seizures
- CNS depression, coma
- Hypertension, tachycardia initially (from blocked inhibitory neurons)
- Followed by: hypotension, bradycardia, conduction block, ventricular arrhythmias
- Bupivacaine is particularly cardiotoxic — rapid binding to sodium channels; cardiac toxicity may precede or occur without CNS prodrome
- Most toxic: bupivacaine, levobupivacaine, ropivacaine, tetracaine
- Intermediate: lidocaine, mepivacaine
- Least toxic: chloroprocaine (metabolised very rapidly by plasma cholinesterase)
- Stop injection immediately
- Call for help
- Airway management — 100% O₂, secure airway if needed (prevent hypoxia and acidosis, which worsen toxicity)
- Treat seizures: benzodiazepines (first-line); propofol/thiopentone (caution with cardiac depression)
- 20% Intralipid (lipid emulsion rescue): 1.5 mL/kg IV bolus → 0.25 mL/kg/min infusion; additional boluses if cardiac arrest persists; max 10 mL/kg
- Must be immediately available whenever regional blocks are performed
- CPR: prolonged resuscitation may be required; if refractory, consider cardiopulmonary bypass
- For bupivacaine: avoid lidocaine (worsens toxicity), use epinephrine in small incremental doses (1 mcg/kg), avoid vasopressin
- Use the lowest effective dose and concentration
- Aspirate before each injection
- Use test dose (3 mL of 1.5% lidocaine + 15 mcg epinephrine)
- Incremental injection — "every dose is a test dose"
- Use ultrasound guidance to reduce volumes needed
H. BACKACHE
- Results from needle trauma through skin, subcutaneous tissue, muscle, and ligaments → bruising, local inflammation, reflex muscle spasm
- Usually mild and self-limited (may last weeks)
- Important: up to 25–30% of patients after general anaesthesia also report postoperative backache
- Management: paracetamol or NSAIDs
- Clinical significance: persistent or worsening backache may signal haematoma or abscess
I. COMPLICATIONS OF PERIPHERAL NERVE BLOCKS
| Complication | Details |
|---|---|
| Nerve injury | Direct needle trauma, intraneural injection, neurotoxicity of local anaesthetic, compression from haematoma |
| Intravascular injection | Leading to LAST (see above); risk reduced by ultrasound guidance and incremental injection |
| Pneumothorax | Risk with interscalene and supraclavicular brachial plexus blocks; incidence ~0.5–6%; may be delayed up to 24 hours; management: observation if small, chest drain if large |
| Phrenic nerve palsy | 100% incidence with interscalene block; contralateral phrenic or respiratory compromise can be fatal in patients with reduced respiratory reserve |
| Recurrent laryngeal nerve block | Hoarseness; with interscalene block |
| Stellate ganglion block | Horner syndrome, hoarseness (from RLN), phrenic nerve palsy — recognised side effects of interscalene block |
| Haematoma | Especially with axillary and femoral blocks near vascular structures |
| Infection | Rare; particularly with indwelling nerve catheters |
| Block failure / inadequate analgesia | 10–20% failure rates for many peripheral nerve blocks |
J. INCIDENCE DATA (Summary Table from Morgan & Mikhail)
| Technique | Cardiac Arrest | Death | Seizure | Cauda Equina | Paraplegia | Radiculopathy |
|---|---|---|---|---|---|---|
| Spinal (n=40,640) | 26 | 6 | 0 | 5 | 0 | 19 |
| Epidural (n=30,413) | 3 | 0 | 4 | 0 | 1 | 5 |
K. SPECIAL SITUATIONS
Anticoagulation and Neuraxial Blocks
- ASRA guidelines (Horlocker et al., 4th edition) govern timing of neuraxial block relative to anticoagulant drugs
- Neuraxial block is contraindicated with active coagulopathy, significant thrombocytopenia (<50,000/mm³ carries up to 11% upper-bound risk for epidural haematoma), fibrinolytics
- Both insertion and removal of epidural catheters carry haematoma risk in anticoagulated patients
Cauda Equina Syndrome
- Reported with continuous spinal catheters using hyperbaric 5% lidocaine
- Mechanism: maldistribution/pooling of concentrated local anaesthetic around sacral roots
- Features: varying degrees of bowel/bladder dysfunction and lower extremity weakness — often permanent
Catheter Shearing / Retention
- Rare mechanical complication — epidural or nerve block catheter fragments may be retained
- Usually managed conservatively unless causing symptoms
- Auroy Y et al. Serious complications related to regional anesthesia. Anesthesiology 1997;87:479–486.
- Horlocker TT et al. ASRA evidence-based guidelines (4th ed.). Reg Anesth Pain Med 2018;43:263.
- Lee LA et al. Injuries associated with regional anesthesia: ASA Closed Claims Analysis. Anesthesiology 2004;101:143.
Can you divide into early late and intermediate complications and also properly define high spinal. Start with the anatomy of spinal cord.
spinal cord segments vertebral levels conus medullaris cauda equina anatomy
spinal cord cross section white matter gray matter tracts dorsal ventral horn anatomy diagram
dermatomal levels spinal anaesthesia block height sympathetic sensory motor regional anesthesia
Complications of Regional Anaesthesia
With Spinal Cord Anatomy, High Spinal Definition, and Early/Intermediate/Late Classification
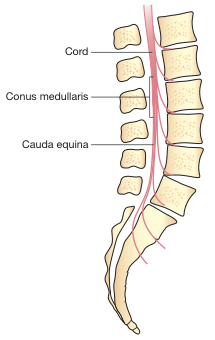
PART I — ANATOMY OF THE SPINAL CORD
Gross Anatomy
- Cervical enlargement (C4–T1): brachial plexus
- Lumbosacral enlargement (L2–S3): lumbosacral plexus
- Pia mater — closely adherent to cord
- Arachnoid mater — separated from pia by the subarachnoid space (contains CSF, site of spinal injection)
- Dura mater — tough outermost layer; between arachnoid and dura is the subdural space (potential space); between dura and vertebral periosteum is the epidural space (contains fat, veins, lymphatics)
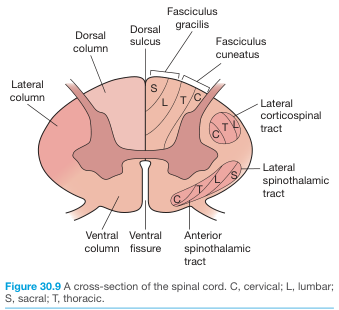
Internal Structure
| Region | Rexed Laminae | Function |
|---|---|---|
| Dorsal (posterior) horn | I–VI | Sensory processing |
| Intermediate zone | VII | Interneurons, autonomic (IML at T1–L2) |
| Ventral (anterior) horn | VIII–IX | Motor neurons (LMN) |
| Central canal region | X | Visceral afferents |
| Column | Major Tracts | Function |
|---|---|---|
| Dorsal (posterior) | Fasciculus gracilis, fasciculus cuneatus | Fine touch, vibration, proprioception (ipsilateral) |
| Lateral | Lateral corticospinal tract (descending); lateral spinothalamic tract (ascending) | Voluntary motor (ipsilateral); pain and temperature (contralateral) |
| Ventral (anterior) | Anterior spinothalamic tract; vestibulospinal tract | Crude touch/pressure; posture |
Vascular Supply
- Anterior spinal artery (single, anterior median fissure): supplies the anterior 2/3 of cord — motor tracts and spinothalamic tract
- Posterior spinal arteries (paired): posterior 1/3 — dorsal columns
- Watershed zone: mid-thoracic cord (T4–T8), most vulnerable to ischaemia
Clinically Relevant Levels for Neuraxial Anaesthesia
| Level | Clinical Significance |
|---|---|
| L1–L2 | Conus medullaris — needle below this level enters subarachnoid space among cauda equina roots (less cord injury risk) |
| T10 (umbilicus) | Minimum for lower abdominal surgery |
| T6 (xiphisternum) | Minimum for upper abdominal surgery |
| T4 (nipple line) | Minimum for caesarean section |
| T1–T4 | Cardioaccelerator fibres — block here causes bradycardia |
| C3–C5 | Phrenic nerve — block causes diaphragmatic paralysis |
PART II — HIGH SPINAL: DEFINITION AND STAGES
Definition
High spinal is defined as cephalad spread of intrathecal local anaesthetic above the intended level, reaching T1 or higher, causing progressive blockade of sympathetic, motor, and sensory fibres with haemodynamic and respiratory compromise.Total spinal (or "massive spinal") is an extreme form where local anaesthetic spreads intracranially, blocking the brainstem respiratory centres and cranial nerves. Intracranial spread is what distinguishes a total spinal from a high spinal (Miller's Anesthesia 10e).
Stages of Progression (Miller's / Barash)
| Stage | Level Blocked | Clinical Features |
|---|---|---|
| 1 | T1–T4 | Bradycardia (cardioaccelerators lost), hypotension worsens |
| 2 | C6–T1 | Tingling/weakness of hands and arms |
| 3 | C3–C5 | Phrenic nerve palsy → diaphragmatic paralysis → apnoea |
| 4 | Cervical cord + brainstem | Unconsciousness, loss of airway reflexes, respiratory arrest, fixed dilated pupils (total spinal) |
Key point (Morgan & Mikhail): Apnoea in high spinal is more often the result of medullary hypoperfusion from severe sustained hypotension than phrenic nerve (C3–C5) paralysis alone.
Causes / Risk Factors
- Accidental intrathecal injection during epidural/caudal technique (epidural doses = 5–10× spinal dose)
- Excessive spinal dose
- Obesity, short stature, pregnancy, spinal deformity
- Spinal after failed epidural; epidural after accidental dural puncture
- Patient repositioning after injection (e.g. Trendelenburg)
Management
- Call for help
- Airway — supplemental O₂, bag-mask ventilation, intubate if unconscious or apnoeic
- Haemodynamic support — rapid IV fluids, vasopressors (ephedrine, phenylephrine, epinephrine), atropine/epinephrine for bradycardia
- Reassurance and psychological support if patient remains conscious
- Maintain support until block resolves (1–3 hours for most agents)
PART III — COMPLICATIONS BY TIME OF ONSET
EARLY COMPLICATIONS (Onset: intra-procedure to within minutes)
1. Hypotension
- Most common complication of neuraxial anaesthesia
- Sympathetic blockade → vasodilation → decreased SVR and venous return
- Worsened by hypovolaemia, high block, pregnancy, obesity, elderly age
- Treatment: pre/co-hydration, left uterine displacement (obstetrics), phenylephrine or ephedrine, leg elevation
2. Bradycardia
- Loss of T1–T4 cardioaccelerator fibres; vagal predominance
- Can precede cardiac arrest
- Treatment: atropine 0.6 mg IV; ephedrine or epinephrine if severe
3. High / Total Spinal
- (Fully described in Part II above)
- Rapid onset when epidural dose accidentally injected intrathecally
- Emergency treatment: intubation, ventilation, cardiovascular support
4. Local Anaesthetic Systemic Toxicity (LAST)
- From intravascular injection or rapid systemic absorption
- CNS prodrome (at lower plasma levels): perioral tingling, metallic taste, tinnitus, lightheadedness → agitation, slurred speech → seizures → CNS depression/coma
- Cardiovascular (higher levels): hypertension/tachycardia → hypotension, conduction block, ventricular arrhythmias, cardiac arrest
- Bupivacaine particularly dangerous — cardiotoxicity may occur without CNS prodrome
- Rank of toxicity (most → least): bupivacaine = levobupivacaine > ropivacaine > tetracaine > lidocaine > mepivacaine > chloroprocaine
- Stop injection; call for help
- 100% O₂, secure airway (prevent hypoxia and acidosis)
- Treat seizures: benzodiazepines (first-line)
- 20% Intralipid (lipid rescue): 1.5 mL/kg IV bolus → infusion 0.25 mL/kg/min; may repeat bolus; max 10 mL/kg
- CPR if arrest — prolonged resuscitation; consider cardiopulmonary bypass if refractory
- Avoid vasopressin; use low-dose epinephrine (1 mcg/kg increments)
5. Inadvertent Intravascular Injection (Epidural-specific)
- Vascular puncture rate approaches 10% with epidural; seizure rate ~1%
- Detected by: aspiration, test dose (3 mL 1.5% lidocaine + 15 mcg epinephrine — intravascular → HR increase ≥20%), incremental dosing
- Reduced by lateral positioning, single-orifice catheter, advancing catheter <6 cm
6. Subdural Injection
- Injection into potential space between dura and arachnoid
- Similar to high spinal but onset delayed 15–30 min; block may be "patchy"
- Space extends intracranially — local anaesthetic can ascend to high levels
- Treatment: supportive (same as high spinal); effects last 1–several hours
7. Failed / Inadequate Block
- Technical failure, inadequate dose, wrong space, catheter malposition
- May require supplementation or conversion to GA
- Must have a prior airway plan (ASA Closed Claims: failure of regional anesthesia without an airway strategy caused serious complications)
8. Pneumothorax (Peripheral blocks)
- Risk with interscalene and supraclavicular brachial plexus blocks
- Incidence: 0.5–6%; may be clinically silent for 6–24 hours
- Management: observation if small; chest drain if large or symptomatic
INTERMEDIATE COMPLICATIONS (Onset: hours to days)
9. Post-Dural Puncture Headache (PDPH)
- Mechanism: CSF leakage through dural defect → intracranial hypotension → vascular hyperaemia, migraine physiology, traction on pain-sensitive structures
- Character: bilateral, frontal/retroorbital/occipital ± neck stiffness; throbbing; ± photophobia, nausea, tinnitus, diplopia
- Hallmark: postural — severe on sitting/standing, relieved immediately on lying flat
- Onset: 12–72 hours after puncture (rarely immediate or >7 days)
- Incidence: after wet tap with epidural needle: 30–60%; incidence of wet tap during labour epidural: 1–1.5%
- Risk factors: large needle, cutting-tip needle (Quincke > Whitacre/Sprotte), young female, prior PDPH, multiple attempts
- Meningitis (fever, nuchal rigidity, CSF pleocytosis)
- Postpartum pre-eclampsia (hypertension)
- Cerebral venous sinus thrombosis
- Subdural haematoma
- Subarachnoid haemorrhage
- Conservative: bed rest, oral hydration, caffeine, paracetamol, NSAIDs, opioids
- Definitive: Epidural Blood Patch (EBP) — 15–20 mL autologous blood; 83% respond to first patch; 16.8% need second; 1.5% need third
- If cranial nerve signs (e.g., diplopia from CN VI palsy): urgent EBP
10. Urinary Retention
- Blockade of S2–S4 parasympathetic fibres → inhibited detrusor → inability to void
- Common with long-acting agents (bupivacaine) and intrathecal opioids
- Management: reassurance, catheterisation if severe
11. Backache
- Tissue trauma from needle insertion through skin, fascia, muscle, and ligaments
- Inflammatory response ± muscle spasm
- Mild, self-limited (days to weeks); occurs in 25–30% after GA as well
- Treatment: paracetamol, NSAIDs
- Important: persistent/worsening backache → investigate for haematoma or abscess
12. Horner Syndrome
- Blockade of cervical sympathetic chain (T1 fibres → superior cervical ganglion → stellate ganglion)
- Features: ptosis, miosis, anhidrosis (ipsilateral)
- Indicates high block level; transient; not independently dangerous
- Also a recognised side-effect of interscalene brachial plexus block (100% incidence)
13. Phrenic Nerve Palsy
- 100% incidence with interscalene block (C3–C5 roots also carry phrenic nerve)
- Ipsilateral hemidiaphragm paralysis — 25% reduction in FVC and FEV1
- Contraindicated/use with extreme caution in: contralateral phrenic palsy, severe COPD, single functioning lung
14. Transient Neurological Symptoms (TNS)
- Burning/aching pain in buttocks radiating to thighs/legs after recovery from spinal anaesthesia
- No objective neurological deficit
- Associated with intrathecal lidocaine (especially hyperbaric 5%), lithotomy position
- Onset: within 24 hours of recovery; resolves within 72 hours
- Management: NSAIDs, reassurance
LATE COMPLICATIONS (Onset: days to weeks; or persistent)
15. Epidural / Spinal Haematoma
- Incidence: ~1:150,000 for epidural; ~1:220,000 for spinal
- Risk factors: coagulopathy, anticoagulants, thrombocytopenia, fibrinolytics, traumatic insertion
- Occurs at insertion or removal of catheter
- Features: sudden sharp back ± leg pain, then progressive motor weakness, sphincter dysfunction (urinary/bowel) — onset more sudden than abscess
- Investigation: urgent MRI (preferred) or CT; neurosurgical consultation
- Treatment: surgical decompression (laminectomy) within 8 hours for best outcome — neurological recovery correlates with severity of deficit at time of diagnosis
- Prevention: follow ASRA anticoagulation guidelines strictly; avoid neuraxial block in coagulopathy
16. Epidural Abscess
- Incidence: 1:6,500 to 1:500,000 epidurals; most with indwelling catheters
- Organisms: S. aureus (most common), S. epidermidis
- Mean time from catheter insertion to symptoms: 5 days (range: days to weeks)
- Back pain — worse on percussion/palpation over spine
- Radicular/nerve root pain
- Motor/sensory deficits, sphincter dysfunction
- Paraplegia/paralysis
- Investigation: MRI spine + blood cultures + catheter tip culture
- Treatment: anti-staphylococcal antibiotics + surgical decompression (laminectomy) ± percutaneous drainage; ID and neurosurgical consultation
- Prognosis correlates with neurological status at time of diagnosis
17. Meningitis / Arachnoiditis
- Infection of subarachnoid space from skin organisms, contaminated equipment/solutions, or oral flora of staff (hence mask requirement)
- Bacterial meningitis: fever, headache, photophobia, nuchal rigidity, CSF pleocytosis
- Arachnoiditis: sterile inflammation → fibrosis → progressive neurological deficits months later; associated with contamination (detergents, antiseptics) and repeated procedures
- Prevention: strict asepsis — hand washing, cap, mask, sterile gloves, chlorhexidine-alcohol skin prep, sterile draping (ASA/ASRA guidelines)
18. Neurological Injury (Persistent)
- Nerve root damage: radiculopathy, paraesthesia, weakness in a dermatomal/myotomal distribution
- Spinal cord injury: rare; direct needle trauma (more likely if needle above conus), intraneural injection
- Cauda equina syndrome: perineal/saddle anaesthesia, bladder/bowel dysfunction, lower extremity weakness; associated with continuous spinal catheters and hyperbaric 5% lidocaine (maldistribution/pooling in sacral roots) — often permanent
- Double crush phenomenon: pre-existing spinal stenosis, disc disease, or prior spine surgery increases vulnerability to needle/pressure injury
19. Anterior Spinal Artery Syndrome
- Ischaemia of the anterior spinal cord following severe hypotension during neuraxial anaesthesia + increased intraspinal pressure
- Loss of anterior cord function: bilateral motor loss (paralysis) + loss of pain/temperature (spinothalamic) below the level
- Dorsal columns (proprioception, fine touch) spared (posterior spinal arteries unaffected)
- Often permanent; poor recovery
20. Peripheral Nerve Injury (Delayed)
- Demyelination or axonal injury from: direct needle trauma, intraneural injection, haematoma compression, neurotoxic additives
- Risk reduced by: ultrasound guidance, paresthesia avoidance, injection pressure monitoring, avoiding injection during patient complaint of pain
Summary Classification Table
| Complication | Timing | Key Feature |
|---|---|---|
| Hypotension | Early (minutes) | Sympathetic block; most common |
| Bradycardia / cardiac arrest | Early (minutes) | T1–T4 block; up to 1:1500 incidence |
| Total spinal / high spinal | Early (minutes) | Intracranial spread = total spinal |
| LAST / intravascular injection | Early (minutes) | Seizures → cardiac arrest; lipid rescue |
| Subdural injection | Early/intermediate (15–30 min) | Patchy high block, delayed onset |
| Pneumothorax | Early to intermediate (hours) | Interscalene/supraclavicular block |
| PDPH | Intermediate (12–72 h) | Postural headache; EBP definitive |
| Urinary retention | Intermediate (hours) | S2–S4 block |
| TNS | Intermediate (24–72 h) | Bilateral buttock/thigh burning; lidocaine |
| Backache | Intermediate (days) | Self-limiting; exclude haematoma/abscess |
| Horner syndrome / phrenic palsy | Intermediate | Interscalene block; high neuraxial |
| Epidural haematoma | Late (hours–days) | Sudden back pain + weakness → emergency surgery |
| Epidural abscess | Late (days–weeks) | 4 stages; S. aureus; laminectomy |
| Meningitis / arachnoiditis | Late (days–weeks) | Aseptic failure; fever + meningism |
| Cauda equina syndrome | Late (persistent) | Saddle anaesthesia; bladder/bowel; lidocaine |
| Anterior spinal artery syndrome | Late (persistent) | Motor + pain/temp loss; proprioception spared |
| Persistent peripheral nerve injury | Late (persistent) | Direct trauma or compression |