Autoimmune hepetitis
Reading File
search_medical_text
autoimmune hepatitis etiology pathogenesis clinical features diagnosis criteria
search_medical_text
autoimmune hepatitis treatment management prognosis complications
GradeResponse
GradeResponse
search_medical_text
autoimmune hepatitis type 1 type 2 autoantibodies ANA SMA LKM1 serological subtypes
search_medical_image
autoimmune hepatitis liver histology interface hepatitis plasma cells
GradeResponse
Autoimmune Hepatitis (AIH)
Definition
Autoimmune hepatitis is a chronic, progressive liver disorder characterized by ongoing hepatocellular necrosis and inflammation, typically with fibrosis, capable of advancing to cirrhosis and liver failure. It is driven by an immune-mediated attack on hepatocytes, and many cases historically labeled "cryptogenic" chronic hepatitis are now recognized as autoimmune in origin. (Harrison's, p. 9538)
Epidemiology
- Predominantly affects women (~70–80%)
- Bimodal age distribution: peaks in adolescence/young adulthood and again in the 5th–6th decades
- Can occur at any age, including children and the elderly
- Prevalence: ~10–17 per 100,000 in Western populations
Subtypes
| Type | Autoantibodies | Typical Population | Notes |
|---|---|---|---|
| Type 1 (most common) | ANA, anti-SMA (anti-actin), anti-SLA/LP | Any age; adults predominate | Associated with other autoimmune diseases |
| Type 2 | Anti-LKM-1 (anti-liver-kidney microsomal), anti-LC-1 | Children & young adults | More aggressive course; higher relapse rate |
Pathogenesis
- Molecular mimicry and loss of self-tolerance trigger T-cell-mediated destruction of hepatocytes
- CD4+ T helper cells and autoreactive CD8+ cytotoxic T cells play central roles
- Strong HLA associations: HLA-DR3 and HLA-DR4 (Type 1); HLA-DR7 (Type 2)
- Environmental triggers (viral infections, drugs) may precipitate disease in genetically susceptible individuals
Clinical Features
Presentations vary widely:
- Acute hepatitis-like onset (~40%): fatigue, jaundice, right upper quadrant discomfort, nausea — can mimic acute viral hepatitis
- Insidious/chronic onset: fatigue, arthralgias, amenorrhea — found incidentally on abnormal LFTs
- Acute liver failure: ~5% present with fulminant hepatic failure
- Asymptomatic: discovered on routine blood work
Extrahepatic autoimmune associations (~40%):
- Autoimmune thyroiditis (Hashimoto's, Graves')
- Rheumatoid arthritis
- Ulcerative colitis
- Sjögren's syndrome
- Type 1 diabetes mellitus
Diagnosis
No single test is diagnostic. The International Autoimmune Hepatitis Group (IAIHG) Simplified Score is widely used:
| Feature | Finding | Points |
|---|---|---|
| ANA or SMA | ≥1:40 | +1 |
| ANA or SMA | ≥1:80 | +2 |
| Anti-LKM-1 | ≥1:40 | +2 |
| Anti-SLA | Positive | +2 |
| IgG | >ULN | +1 |
| IgG | >1.10× ULN | +2 |
| Liver histology | Compatible | +1 |
| Liver histology | Typical | +2 |
| Absence of viral hepatitis | Yes | +2 |
- Score ≥7: probable AIH; ≥7 with typical histology: definite AIH
Key laboratory findings:
- Elevated aminotransferases (AST/ALT) — typically 5–50× ULN
- Elevated IgG (polyclonal hypergammaglobulinemia)
- Positive autoantibodies (ANA, SMA, LKM-1)
- Elevated bilirubin and ALP in more advanced disease
Liver biopsy — essential for confirmation:
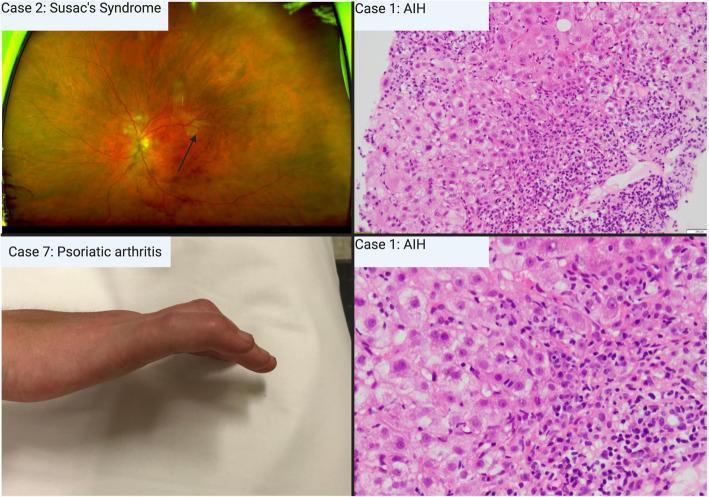
Hallmark histological features:
- Interface hepatitis (periportal lymphoplasmacytic infiltrate)
- Plasma cell-rich portal and lobular infiltrate
- Rosette formation of hepatocytes
- Emperipolesis (lymphocytes penetrating hepatocytes)
Treatment
First-Line: Glucocorticoids ± Azathioprine
(Harrison's, p. 9546)
Therapeutic response expected in up to 80% of patients.
Prednisone regimens:
| Approach | Initiation | Taper |
|---|---|---|
| Monotherapy (prednisone) | 60 mg/day | Taper over weeks to 20 mg/day, then slowly to maintenance |
| Combination (prednisone + azathioprine 50 mg/day) | 30 mg/day | Taper prednisone to 10 mg/day |
- Combination therapy is preferred in most patients — allows lower steroid doses and reduces steroid side effects
- Prednisolone is equivalent to prednisone and may be used interchangeably
Treatment endpoints:
- Complete biochemical remission (normal AST/ALT, IgG)
- Histological remission (requires biopsy)
- Sustained remission off therapy (achieved in ~20% long-term)
Maintenance: Azathioprine 2 mg/kg/day as steroid-sparing agent
Second-Line (Refractory/Intolerant)
| Agent | Notes |
|---|---|
| Mycophenolate mofetil (MMF) | Most common second-line; effective in azathioprine-intolerant patients |
| Tacrolimus | Used in refractory cases |
| Cyclosporine | Particularly in children |
| Budesonide | Alternative first-line in non-cirrhotic patients; fewer systemic steroid effects |
Liver Transplantation
- Indicated for decompensated cirrhosis or acute liver failure unresponsive to medical therapy
- 5-year survival post-transplant: ~80%
- Disease can recur in the allograft (~25–40%)
Monitoring & Complications
- Relapse occurs in ~50–80% after treatment withdrawal — most require long-term maintenance
- Monitor LFTs, IgG, and CBC (for azathioprine myelosuppression — check TPMT enzyme activity before initiating)
- Screen for osteoporosis and glucose intolerance from chronic steroid use
- Progression to cirrhosis and hepatocellular carcinoma (HCC) in cirrhotic patients — surveillance with ultrasound every 6 months
Prognosis
| Population | 10-year Survival |
|---|---|
| Treated patients | 80–98% |
| Untreated patients | ~67% |
- Untreated severe disease: 6-month mortality up to 40% (Harrison's, p. 9538)
- Early diagnosis and prompt treatment dramatically improve outcomes
- Factors predicting poor prognosis: cirrhosis at presentation, HLA-DR3 positivity, delayed treatment
Key Differentials
- Drug-induced liver injury (DILI) with autoimmune features (nitrofurantoin, minocycline, methyldopa)
- Primary biliary cholangitis (PBC) — elevated ALP, anti-mitochondrial antibodies
- Primary sclerosing cholangitis (PSC)
- Wilson's disease (especially in young patients)
- Viral hepatitis (HBV, HCV, EBV, CMV)
- AIH-PBC/PSC overlap syndromes — features of both conditions
This is a shared conversation. Sign in to Orris to start your own chat.